

Taking Emergency Departments Out of Oral Health Care
These strategies will help ensure that vulnerable children receive routine and preventive oral care in dental — rather than medical — settings.
The following strategies will help ensure that vulnerable children receive routine and preventive oral care in dental — rather than medical — settings.
PURCHASE COURSE
This course was published in the November 2016 issue and expires 11/30/19. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Identify the reasons children utilize hospital emergency departments (ED) for dental treatment.
- Discuss strategies for expanding access to dental care in an attempt to encourage treatment by oral health professionals, rather than ED staff.
- Explain the impact of the Patient Protection and Affordable Care Act’s essential benefit for children’s oral health services.
Dental professionals are well aware of the relationship between oral and overall health. Strategies have been implemented to improve the oral health of children in the United States. These initiatives range from the provision of preventive dental care in school-based settings to the inclusion of pediatric dental services as an essential health benefit under the Patient Protection and Affordable Care Act (ACA). Yet, despite these efforts, the oral health of the nation’s most vulnerable children remains in jeopardy.
Access to professional dental care is the cornerstone of improving and maintaining oral health among all patient populations. One indicator of ease of access to dental care is the number of people who visit hospital emergency departments (EDs) for dental problems. This article examines why the use of EDs for dental treatment is ineffective. It will also explore strategies for increasing access to care, and offer suggestions for more effective ways to ensure children receive necessary oral health care services.
The Nationwide Emergency Department Sample (NEDS) contains information from approximately 30 million hospital ED discharges.1 In 2014, my colleagues and I published a study that utilized the NEDS database to identify the characteristics of children who visited EDs to receive treatment for dental conditions.2 The results showed that 215,073 children visited the ED for treatment of dental problems in 2008. This group consisted of more than 91,000 children covered by Medicaid, and 68,000 children without insurance.2 Among children who sought dental care in EDs, 72% were from families from regions with mean household incomes of $49,000 or less. Compared to families whose mean incomes are higher, members of these households tend to have less education and low oral health literacy.3
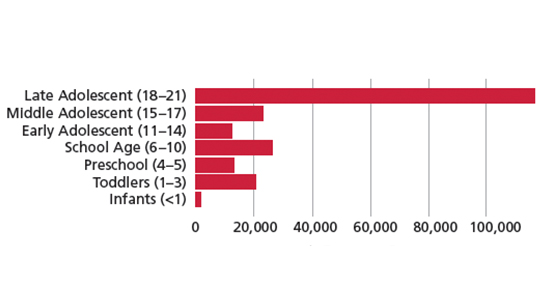
The study also showed that late adolescents (ages 18 to 21) were most likely to visit EDs for dental treatment (Figure 1). Late adolescents are often without parental supervision, as more than 50% of individuals ages 18 to 23 live independently.4 Karimi et al5 found that 18- to 24-year-olds have the lowest health care utilization among adults. Moreover, many in this age group have limited financial means, little credit history, and may face challenges paying for health care.6Additionally, Wolf et al7 report that late adolescents may not have adequate oral health literacy, which is critical for developing and maintaining effective health practices.
There are two primary reasons for ED dental visits by children and adolescents. First, the pain has become so severe that emergency treatment is necessary. Second, the patient does not have regular access to dental care, which may be due to a lack of insurance/funding, absence of a dental care provider with appointment availability in the patient’s area, or lack of transportation. Most ED visits for dental treatment are necessitated by untreated dental caries, pulpal and periapical disease, gingival and periodontal disease, and mouth cellulitis — all of which are preventable.
RESULTS OF EMERGENCY DEPARTMENT CARE
Perhaps the most obvious reason that EDs should not be a source for dental treatment is cost. The overall charges for the ED visits analyzed in our study were $104.2 million, and the average hospital charge was $564 per visit.2A typical preventive or corrective dental office visit ranges from $50 to $350, depending on location. In addition, the use of EDs does not eliminate the need to see a dental professional. Research by Cohen et al8 shows that 96% of patients who visited the ED for a dental problem still needed follow-up care from a dentist. This demonstrates that ED treatment doesn’t typically serve as an alternative to visiting the dental office; rather, it simply increases the overall cost of care.
Another important finding is what happens after the ED visit. While the vast majority of the 215,073 ED visits resulted in routine discharge, 8723 patients were admitted to long- or short-term care facilities or enrolled in home health care.2 In other words, these ED visits were further dispersed into the health care system, which adds to the overall cost of care. In fact, the 7195 ED visits that resulted in hospitalizations had a 4.6-day mean length of stay and incurred $162 million in hospital charges — 55.5% more than the hospital charges for all of the 215,073 ED visits.2 Perhaps the most important part of this data analysis is to identify the characteristics of the patients who were hospitalized in order to facilitate early identification of dental problems. The overarching goal is to prevent the need for ED visits and hospitalizations.
Another concern is the quality of care provided in EDs. Only 1% of U.S. dentists practice in hospitals,9 and research shows that hospital EDs poorly manage dental conditions.10A study by Al-Khabbaz et al,11 for example, found that physicians’ knowledge of oral health is low.
IMPACT OF IMPLEMENTED STRATEGIES
It was hoped the ACA would improve children’s access to dental care. Theoretically, the ACA ensures the availability of coverage for pediatric dental services, but it does not require individuals or families to purchase dental insurance, and many have declined coverage.12,13 For example, households whose mean income is $49,000 or less are more likely to decline coverage under the ACA than families with higher incomes. This supports the theory presented in Maslow’s Hierarchy of Needs, which suggests that individuals whose low-level needs are not being met will not consider high-level matters important.14If individuals are concerned about their personal safety because they’re living in a dangerous neighborhood, for example, they are not likely to view pediatric dental visits as important. Additionally, implementation of the ACA varies from state to state. Utah’s ACA model is a case in point, as it covers only preventive services and not general or restorative dental care.12
The ACA’s expansion of Medicaid and inclusion of pediatric dental benefits was also expected to improve access to care for vulnerable populations. Data from the American Dental Association (ADA) show the number of Medicaid-covered children who visited the dentist rose from 29% in 2000 to 48% in 2013.15 Although this represents significant improvement, 48% is still a low level of utilization. The results of our study found that while Medicaid did not insure every child for routine and emergency dental care, it was the largest payer for patients who sought dental treatment in EDs.2 Additional ADA data suggest that Medicaid’s share of dental ED visits has actually increased.16 In fact, another study indicates the number of ED visits for dental care is trending upward.
FIXING THE PROBLEM
The oral health care profession needs to develop more effective strategies to keep children out of hospital EDs for dental treatment and get them into dental homes. A major challenge is the fact that 69% of U.S. dentists practice in a traditional solo practice setting.18 Although patients may value their personal relationship with their family dentist, this structure doesn’t help expand access to care. Large group practices can offer weekend and after-hours appointments that may improve utilization by at-risk populations. These expanded hours would be difficult for a solo practitioner to provide.
Increasing collaboration between oral health care providers to facilitate 24-hour emergency dental care for children would effectively solve this problem, but it seems difficult to imagine how this could be accomplished. A more practical alternative is to integrate dental hygienists into medical practice, where they can provide preventive treatments, such as the application of fluoride varnish and placement of dental sealants, while also providing critical oral health education to parents/caregivers and patients.19
In addition, broadening the ability of dental hygienists to provide care outside of the traditional dental offices and expanding the concept of midlevel practitioners could help alleviate access-to-care problems. Today, 38 states allow dental hygienists to provide care directly to patients, and 16 states have approved payment from Medicaid for these services.20,21 The ADA, however, has historically opposed such efforts.22–24
Our evaluation revealed some important patterns among children regarding insurance status associated with ED visits and hospitalizations due to dental conditions. Patients covered by Medicaid represented 43% of the ED visits for dental treatment and 50% of the hospitalizations.2 These data suggest that providing oral health education and preventive care to children covered by Medicaid is critical to improving oral health outcomes.
Analysis of NEDS data from 2008 show that of the children visiting EDs for dental treatment, 96% did not have other health problems.2 Among patients who were hospitalized, 15% had one comorbid condition, 4% had two, and 1% had three or more.2Clearly, providing specialized care for dental-related ED visits to individuals with preexisting conditions could help reduce hospitalizations and health care resource utilization. Additional or mandated dental Medicaid support for children with comorbidities may help prevent these patients from visiting EDs for dental problems. Patients with comorbidities may also be more likely to visit physicians for medical care, which supports the concept of integrating dental professionals into medical practice.
CONCLUSION
In review, factors that increase children’s use of EDs for dental conditions include being covered by Medicaid, the presence of comorbidities, being between the ages of 18 and 21, and having a mean household income of $49,000 or less. In an attempt to minimize cases requiring hospitalization, children meeting three or more of these criteria should be given special care in preventive dental services, and also receive more aggressive, customized care if they present to the ED for dental treatment.
Additional strategies must be developed to ensure vulnerable children have access to oral health care services from dental professionals. Otherwise, hospital EDs will continue to be used for dental treatment, children and parents/caregivers will experience more lost days from school and work, and children will go on to experience significant health problems caused by preventable dental diseases.
Pediatric Dental Benefits Under the Affordable Care Act
Enacted in 2010, the Patient Protection and Affordable Care Act (ACA) considers dental care as one of 10 “essential health benefits” for children 18 and under. This means children eligible under Medicaid or the State Children’s Health Insurance Program (CHIP) are afforded some level of dental coverage, and that pediatric dental benefits must be available to families purchasing insurance in the federal or state-run marketplaces. While the American Dental Association reports that 8.7 million children are expected to gain some form of dental benefit by 2018 as a result of the ACA,25 it is important to note that families are not necessarily required to purchase pediatric dental insurance. Although policies must be offered through the exchanges, unless states mandate coverage, families may be able decline pediatric dental benefits.26
According to the Children’s Dental Health Project, a Washington, D.C.-based advocacy group, 43 million pediatric patients had public health coverage through Medicaid or CHIP in 2013, and 3 million children and “young people” are expected to enroll in ACA benefits by 2018.26
REFERENCES
- Healthcare Cost and Utilization Project. About the NEDS. Available at: hcupus.ahrq.gov/nedsoverview.jsp#about. Accessed September 28, 2016.
- Allareddy V, Nalliah RP, Haque M, Johnson H, Rampa SB, Lee MK. Hospital based emergency department visits with dental conditions among children in the United States: nationwide epidemiological data. Pediatr Dent.2014;36:393–399.
- Naghibi Sistani MM, Yazdani R, Virtanen J, Pakdaman A, Murtomaa H. Determinants of oral health: does oral health literacy matter? ISRN Dent.2013;249591.
- Jones JM. In U.S., 14% of Those Aged 24 to 34 Are Living With Parents. Available at: gallup.com/poll/167426/aged-living-parents.aspx. Accessed September 28, 2016.
- Karimi S, Keyvanara M, Hosseini M, Jazi MJ, Khorasani E. The relationship between health literacy with health status and healthcare utilization in 18–64 years old people in Isfahan. J Educ Health Promot. 2014;3:75.
- Advisor Perspectives. Median Household Incomes by Age Bracket: 1967–2014. Available at: advisorperspectives.com/dshort/updates/Household-Incomesby-Age-Brackets.php. Accessed September 28, 2016.
- Wolf MS, Wilson EA, Rapp DN, et al. Literacy and learning in health care. Pediatrics. 2009;124(Suppl 3):S275–S281.
- Cohen LA, Bonito AJ, Eicheldinger C, et al. Comparison of patient centeredness of visits to emergency departments, physicians, and dentists for dental problems and injuries. J Am Coll Dent. 2010;77:49–58.
- Solomon E. Dental workforce trends and the future of dental practices. Available at: dentaleconomics.com/articles/print/volume-105/issue-2/macroeconomics/dental-workforce-trends-and-the-future-of-dentalpractices.html. Accessed September 28, 2016.
- Tulip DE, Palmer NO. A retrospective investigation of the clinical management of patients attending an out of hours dental clinic in Merseyside under the new NHS dental contract. Br Dent J. 2008;205:659–664.
- Al-Khabbaz AK, Al-Shammari KF, Al-Saleh NA. Knowledge about the association between periodontal diseases and diabetes mellitus: contrasting dentists and physicians. J Periodontol. 2011;82:360–366.
- American Dental Association. Affordable Care Act, Dental Benefits Examined. Available at: ada.org/en/publications/ada-news/2013-archive/august/affordable-care-act-dental-benefits-examined. Accessed September 28, 2016.
- Obamacare Facts. Dental Insurance. Available at: obamacarefacts.com/dental-insurance/dental-insurance. Accessed September 28, 2016.
- Green CA. A Theory of Human Motivation. Available at: psychclassics.yorku.ca/Maslow/motivation.htm. Accessed September 28, 2016.
- American Dental Association. The Oral Health Care System: a State-by-State Analysis: Key Findings. Available at: ada.org/~/media/ ADA/Science%20 and%20Research/HPI/ OralHealthCare-StateFacts/Oral-Health-Care-System-Key-Findings.ashx. Accessed September 28, 2016.
- Wall T, Vujicic M. Emergency Department Use for Dental Conditions Continues to Increase. Available at: ada.org/~/ media/ADA/ Science%20 and%20Research/HPI/Files/ HPIBrief_0415_2.ashx. Accessed September 28, 2016.
- Allareddy V, Rampa S, Lee MK, Allareddy V, Nalliah RP. Hospital-based emergency department visits involving dental conditions: profile and predictors of poor outcomes and resource utilization. J Am Dent Assoc.2014;145:331–337.
- American Dental Association. ADA explores growth of large group practices. Available at: ada.org/en/publications/ada-news/2012-archive/april/ada-exploresgrowth-of-large-group-practices. Accessed September 28, 2016.
- Braun PA, Kahl S, Ellison MC, Ling S, Widmer-Racich K, Daley MF. Feasibility of colocating dental hygienists into medical practices. J Public Health Dent.2013;73:187–194.
- American Dental Hygienists’ Association. Medicaid Direct Reimbursement of Dental Hygienists. Available at: adha.org/reimbursement. Accessed September 28, 2016.
- American Dental Hygienists’ Association. Direct Access States. Available at: adha.org/resources-docs/7513_Direct_Access_to_Care_from_DH.pdf. Accessed September 28, 2016.
- Levine D. Why Are Dentists Opposing Expanded Dental Care? Available at:governing.com/topics/health-human-services/gov-why-are-dentists-opposing-expanded-dental-care.html. Accessed September 28, 2016.
- American Dental Association. American Dental Association Statement on Accrediting Dental Therapy Education. Available at: ada.org/en/pressroom/news-releases/2015-archive/august/american-dental-associationstatement-on-accrediting-dental-therapy-education-programs. Accessed September 28, 2016.
- American Dental Association. Do Midlevel Providers Improve Oral Health? Available at: ada.org/en/publications/ada-news/2013-archive/january/domidlevel-providers-improve-oral-health. Accessed September 28, 2016.
- Nasseh K, Vujicic M, O’Dell A. Affordable Care Act Expands Dental Benefits for Children But Does Not Address Critical Access to Dental Care Issues. Available at: ada.org/~/media/ADA/Science and Research/HPI/Files/HPIBrief_0413_3.pdf. Accessed September 28, 2016.
- Children’s Dental Health Project. FAQ: Pediatric Oral Health Services in the Affordable Care Act (ACA). Available at: cdhp.s3.amazonaws.com/ resource/165/attachment_1/original.pdf?. Accessed September 28, 2016.
From Decisions in Dentistry. November 2016;2(11):32–35.

