

Surgical Guide Techniques for Dental Implant Placement
When properly used, surgical guides can increase the predictability of dental implant treatment.
When properly used, surgical guides can increase the predictability of dental implant treatment outcomes
A dilemma faced by every implant clinician is the choice to place implants freehand or with the aid of a surgical guide. With good technique, the use of surgical guides can be a confidence-building and predictable method for implant placement. It can assist the practitioner in avoiding damage to anatomic structures, as well as limiting fenestration and dehiscence of the alveolar ridge at potential implant sites. However, the surgeon must be confident in his or her ability to place dental implants prior to using surgical guides due to the increased number of steps and processes involved — as each step can result in slight inaccuracies that can ultimately lead to misplacement and require guideless corrections.
Guided surgery allows clinicians to develop a restoratively driven surgical plan, with the ultimate goal of patient-centered, positive outcomes. Several guided options are available, and the dentist must choose the option leading to the best outcome for each specific case. The choice between a tooth-, mucosal- or bone-borne guide is unique to the clinical situation, and all have inherent inaccuracies. These may involve the type of hard- or soft-tissue support available, quality of the diagnostic image, implant planning software, and potential errors in the fabrication process. There are advantages and disadvantages to each type of guide.
TOOTH-BORNE GUIDES
Tooth-borne surgical guides (Figure 1 and Figure 2) are common and easily adaptable to various clinical situations. One benefit is that consistently reproducible landmarks (namely, teeth) can be used for support, stability and retention. The improved accuracy and precision of implants placed through tooth-borne guides have been evaluated in both benchtop and clinical models.1,2 The most common utilization of tooth-borne guides is for single or multiple implants for fixed restorations. Although these guides have been shown to result in predictable restorative outcomes, it is important for the practitioner to be cognizant of available space and additional guided drill length, especially when placing posterior implants.3
place implants fully guided.

guide fabricated from a thermoplastic material.
MUCOSAL-BORNE GUIDES
As the name suggests, a mucosal-borne surgical guide (Figures 3A and 3B) uses intraoral soft tissues for support and stability. This guide is commonly fabricated based on an existing removable prosthesis. Possible concerns with mucosal support involve the lack of retention during surgery and variation in tissue thickness and quality — which is a common complaint also seen with complete dentures.4,5 A mucosal-borne guide has the potential to undergo movement in varying directions that could increase the inaccuracy of implant placement. This, along with flap reflection, may introduce additional complexity during implant placement.

BONE-BORNE GUIDES
A bone-borne surgical guide (Figure 4 and Figure 5) is generally used for full-arch edentulous implant cases. This type of guide derives its support from load bearing areas and/or the natural divergence of the alveolar ridge seen in both maxillary and mandibular arches in a corono-apical direction. Bone-borne guides are difficult to fabricate and accurately place intraorally due to the extent of flap reflection needed for access, as well as inaccuracies that can result from the digital workflow. Although the difficulties associated with bone-borne guides are well reported,1 they may be mitigated with proper planning, accurate imaging and operator experience.
TREATMENT PLANNING
When the decision is made to use a surgical guide, there are no standards that suggest a specific design. One of the advantages of planning cases digitally is the ability to utilize a combination of supporting structures during the treatment planning and design process; these can include teeth, mucosa, bone, and possibly existing implant components.
Treatment planning in cases involving a completely edentulous patient provides several options. Stackable guides are becoming increasingly popular due to their ease of use and adaptability. These guides derive support from a single foundational guide. The foundation guide is placed first, generally with support from bone, and followed by the sequential placement of required guides. For example, the first component may be a guide that could direct any needed reduction of the alveolar ridge, while the second component allows the placement of implant fixtures. Additional components can allow the accurate placement of restorative components, and the ability to index the prosthesis on the foundation guide.

edentulous case.
stabilization pins secured in the alveolus.
transitioned into a bone-supported guide.
Another possibility includes the transition from a mucosal-borne guide (with the use of stabilization pins) to a designed guide that derives support from mucosa and adjacent bony structures. With advances in implant planning software, it is now feasible for clinicians to plan and print elaborate, multilayered guides in-house. An example of this treatment option (Figure 6, Figure 7 and Figure 8) involved an intraoral scan used in combination with digital planning software, followed by the fabrication of the surgical guide with a three-dimensional printer. A unique property of this guide system is the ability to align the guide, place stabilization pins, and allow the guide to remain fixated until after the implants are placed. This might eliminate the possibility of compounding inaccuracies that can occur when the surgical guide is removed and inserted multiple times throughout a procedure.
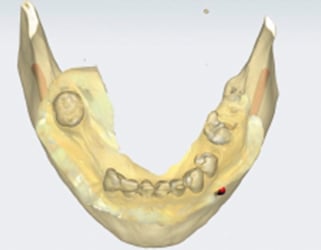
arch, with treatment planned for a
mandibular overdenture.

with combined STL and DICOM files.

surgical guide planned in preparation for two mandibular implants.
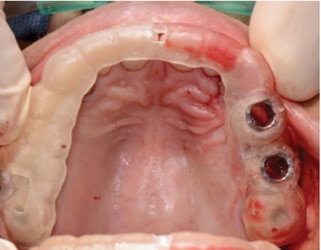
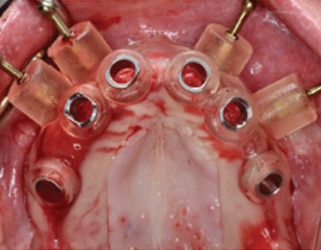
Surgical guides may also be used to help treat patients transitioning from a failing dentition to an interim, implant-supported prosthesis. In a patient undergoing full-arch extractions followed by two implants to support a mandibular overdenture, a guide can be supported using multiple nonrestorable, but intact, teeth, as well as mucosa. A traditional treatment option in this scenario could include extraction and alveoloplasty, followed by freehand implant placement. An alternative to this method might include the use of implant planning software (Figure 9, Figure 10 and Figure 11) to virtually extract teeth #22 and #27, where future implants were planned to be used in an overdenture. In this case, the canines and adjacent teeth will be extracted first, the surgical guide fitted, and osteotomy preparations made to depth at the #22 and #27 sites. Implants will be placed in a parallel fashion, and the remaining teeth will be extracted after implant placement. This method could reduce surgical time and improve accuracy in aligning implants. Patients may benefit from this approach by reducing the number of resilient components needed during follow-up visits.

with treatment planned for extractions and
immediate implants.

surgical guide.

preparation for implant placement.
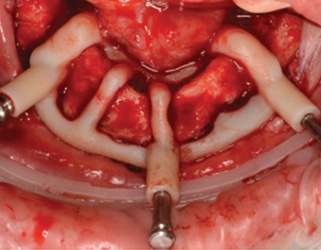
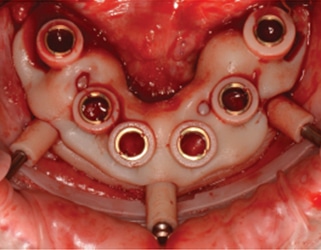
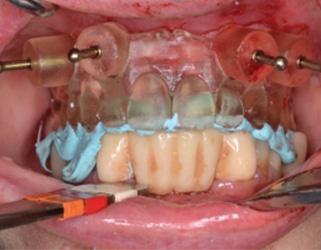
A final application involves a situation similar to the previous case. Partially dentate patients might present with implants already integrated, but are now in need of transition to a full-arch, implant-supported prosthesis. Again, with the use of intraoral scanners, a combination of implant abutments and teeth can be used to support the surgical guide. This method was used to place three immediate implants to support an implant-supported interim prosthesis. The guide was supported by teeth and implant abutments that were in place during the initial scan (Figure 12, Figure 13, Figure 14 and Figure 15).

CLOSING THOUGHTS
The use of implant planning software for guide fabrication in these cases improved the predictability and efficiency of implant placement. It also contributed to better patient-centered outcomes related to reduced surgical exposure and improved prosthesis fit. This model allows the clinician to develop a favorable surgical plan that is restoratively driven. Surgical guide options include tooth-, mucosal- or bone-borne guides — or a combination of these approaches. The cases presented here demonstrate an opportunity for clinicians to be innovative and think creatively when developing surgical plans and fabricating implant guides.
KEY TAKEAWAYS
- With good technique, guided surgery using a tooth-, mucosal- or bone-borne guide — or a combination of these approaches — can be a predictable method for dental implant placement.
- Although it increases the number of steps compared to freehand placement, guided implant surgery allows clinicians to develop a restoratively driven surgical plan, with the ultimate goal of patient-centered, positive outcomes.
- Surgical guides can assist the practitioner in avoiding damage to anatomic structures, as well as limiting fenestration and dehiscence of the alveolar ridge at potential implant sites.
- When the decision is made to use a surgical guide, there are no standards that suggest a specific design is best.
REFERENCES
- Vermeulen J. The accuracy of implant placement by experienced surgeons: guided vs freehand approach in a simulated plastic model. Int J Oral Maxillofac Implants. 2017;32:617–624.
- Nickenig HJ, Wichmann M, Hamel J, Schlegel KA, Eitner S. Evaluation of the difference in accuracy between implant placement by virtual planning data and surgical guide templates versus the conventional free-hand method — a combined in vivo — in vitro technique using cone-beam CT (Part II). J Craniomaxillofac Surg. 2010;38:488–493.
- Raico Gallardo YN, da Silva-Olivio IR, Mukai E, Morimoto S, Sesma N, Cordaro L. Accuracy comparison of guided surgery for dental implants according to the tissue of support: a systematic review and meta-analysis. Clin Oral Implants Res. 2017;28:602–612.
- Cassetta M, Giansanti M, Di Mambro A, Stefanelli LV. Accuracy of positioning of implants inserted using a mucosa-supported stereolithographic surgical guide in the edentulous maxilla and mandible. Int J Oral Maxillofac Implants. 2014;29:1071–1078.
- Ochi M, Kanazawa M, Sato D, Kasugai S, Hirano S, Minakuchi S. Factors affecting accuracy of implant placement with mucosa-supported stereolithographic surgical guides in edentulous mandibles. Comput Biol Med. 2013;43:1653–1660.
The authors have no commercial conflicts of interest to disclose.
Featured Image by VIDI STUDIO / ISTOCK / GETTY IMAGES PLUS
From Decisions in Dentistry. August 2018;4(8):11—13.

[…] specifically, for dental, we can also distinguish between tooth, mucosa or bone supported surgical guides. The surgical guides considers also few stages which […]