

Strategies for Immediate Implant Placement
An approach to immediate implant placement based on the socket shield technique and buccal bone morphology.
An approach to immediate implant placement based on the socket shield technique and buccal bone morphology
PURCHASE COURSE
This course was published in the March 2019 issue and expires March 2022. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the March 2019 issue and expires March 2022. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Explain risk assessment and treatment objectives for dental implant therapy in the esthetic zone.
- Discuss indications for immediate implant placement using the socket shield technique.
- List possible complications of immediate implant placement using the socket shield technique.
The benefits of dental implants include restoring function and esthetics, avoiding preparation of abutments adjacent to missing teeth, long-term favorable prognosis, and a high level of patient satisfaction. The primary objective of implant therapy in the esthetic zone is an optimal esthetic outcome, with high predictability and a low risk of complication.1 Secondary objectives include minimal surgical interventions (open-flap procedures, in particular), the least possible pain and mobility for the patient, short treatment time, and cost effectiveness.2 The efficacy of immediate implant placement has been shown to be predictable, assuming reasonable guidelines are followed.3 The literature demonstrates high success rates with extraction and immediate implant placement, followed by immediate provisionalization in the esthetic zone.4
Immediate implant placement may be the treatment of choice for a tooth with endodontic failure, internal and/or external root resorption, extensive subcrestal caries or root fracture.5 The International Team for Implantology (ITI) Consensus Conference 2013 clearly indicated that implants should be placed in the early time frame following tooth extraction, using either an immediate or early implant placement approach.2 Late implant placement should only be used if there are patient- and site-specific reasons,2 and may lead to pain, swelling, bleeding, hematoma,6 infection, soft tissue dehiscense, multiple surgical interventions and longer treatment.
This paper presents indications for immediate implant placement and strategies utilized in two cases in which classification of pre-extraction buccal bone morphology helped predict postextraction bone morphology. Although the socket shield technique is a new approach that needs further validation,7 it may be a treatment of choice for the esthetic zone because it offers the advantages of immediate implant placement, comparatively low morbidity, a favorable cost/benefit ratio, and reduced risk regarding the esthetic outcome.8
The ITI Consensus Conference offers clear recommendations for when immediate implant placement is indicated.9 These include a fully intact facial bone wall at the extraction site, with a thick wall phenotype (> 1 mm); thick gingival biotype; no acute infection at the extraction site; and sufficient volume of bone apical and palatal of the extraction site to allow implant insertion in a correct three-dimensional position, with sufficient primary stability.2
However, the average thickness of the buccal plate of the anterior maxilla from the central incisors to first premolars ranges from 0.50 to 0.73 mm.10 Another study found the mean thickness of the buccal plate of the central incisor and lateral incisors ranges from 0.6 to 0.9 mm.11
The buccal plate mainly consists of bundle bone and receives its blood supply from the periodontal ligament. When a tooth is extracted, the bundle bone and periodontal ligament are lost; thus, the buccal bone plate and covering soft tissues will be thinned — and even reduced in height — as the bundle bone extends into the tip of the buccal bone wall. Because the coronal aspect of the maxillary anterior teeth often consists solely of bundle bone, its loss will not only lead to thinning, but also complete resorption of the buccal bone.12 Due to the unpredictable amount of bone loss in the buccal plate following extraction, implant treatment in the esthetic zone can be challenging.
A problem often encountered with immediate implant placement in the esthetic zone is that approximately 1 mm of recession of the buccal soft tissue margin is observed over an 18-month period.13 This may be due to thin or missing buccal plate, an implant placed toward the buccal, and/or a thin soft tissue biotype. Ross et al4 suggest that implant diameter, gingival biotype, surgical technique, and/or the reason for tooth loss can influence the amount of gingival recession occurring in single immediate implant placement.
BUCCAL BONE MORPHOLOGY
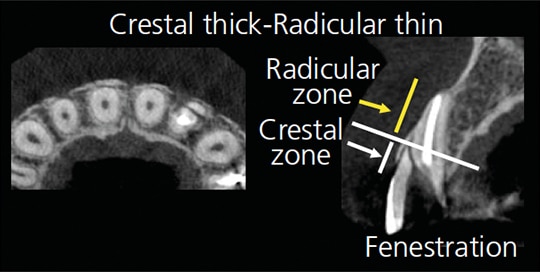
The system proposed by Mandelaris et al14 categorizes facial bone thickness between the crestal and radicular zones of the dentoalveolar compartments for risk assessment in interdisciplinary therapy involving orthodontics and implantology. The crestal zone is the region from the cementoenamel junction extending to a point 4 mm apical.14 The radicular zone extends from the base of the crestal zone to the root apex. Buccal bone morphology for the crestal and radicular zones are assessed separately, and classified as crestal thick-radicular thick, crestal thick-radicular thin, crestal thin-radicular thick, or crestal thin-radicular thin.14
Results have shown that thick-thick and thin-thick have thick bone in the radicular zone. This type of bone may have limited buccal bone loss following extraction. By comparison, thick-thin and thin-thin types have thin bone in the radicular zone, therefore, there may be more buccal bone loss after extraction. Examining the relationship between the two zones of the buccal plate and predicting the amount of bone loss following extraction will help clinicians select an effective, predictable procedure for implant surgery.
Risk assessment for immediate implant placement generally focuses on the position and thickness of the alveolar crest. Kois15 reports the so-called “thick-flat” gingival biotype is a prognostic factor for esthetically successful implant outcomes. Evans and Chen16 note that patients with “thin-scalloped” labial gingiva around the implant shoulder have a higher risk for recession after immediate implant placement.16 The caveat of classifying the soft tissue thickness is that it does not consider the buccal bone morphology, which is affected by the position and angulation of the anterior tooth. It also does not predict bone loss following extraction. Therefore, in addition to considering soft tissue thickness, dividing the buccal bone in the crestal and radicular zones and classifying its thickness prior to extraction may be helpful in predicting the amount of bone loss following extraction.
Descriptions, indications and recommended surgical techniques for the four types of bone combinations are described below:
Crestal thick-radicular thick — The buccal bone in the crestal and radicular zones is thick, thus, a small amount of postextraction buccal bone is subject to resorption. Either immediate or delayed implant placement causes minimum esthetic problems and provides a high level of predictability when implants are placed deeper and more palatal.
Crestal thin-radicular thick — There is a small amount of postextraction buccal bone resorption due to the thick buccal plate in the radicular zone. Although small, localized crestal dehiscence may exist, and minor contour augmentation is possible and predictable.
Crestal thick-radicular thin — The buccal bone in the radicular zone is thin, which may increase the risk of an apical fenestration when the bone resorbs. Due to alveolar ridge anatomy, postextraction ridge augmentation is likely to result in an unnatural alveolar morphology and low predictability. As the concavity of the buccal alveolar process becomes severe, bone loss increases proportionately. If the buccal root fragment is healthy, the socket shield technique is recommended.
Crestal thin-radicular thin — Because a large amount of postextraction buccal bone resorption is expected (due to thin buccal plate in both the crestal and radicular zones), this often leads to a large, flat bone defect and need for extensive bone augmentation. However, the predictability of bone augmentation is low due to a high risk of resorption caused by several factors, including lip pressure. The socket shield technique is recommended only for cases involving a healthy buccal root fragment.

CASE 1: SEVERE BUCCAL BONE LOSS — CRESTAL THICK-RADICULAR THIN
A 30-year-old female’s chief complaint was a fracture on tooth #10. From the labial view, the buccal marginal gingiva was thick and exhibited normal texture. An intact buccal alveolar process and marginal bone were observed (Figure 1). Using cone beam computed tomography (CBCT), a sagittal view showed a 2-mm fracture below the buccal crest. The buccal bone was thick in the crestal zone, but the radicular zone was thin, with fenestration, so the amount of buccal bone loss following extraction was likely to be significant (Figure 2). The treatment plan included using the socket shield technique and immediate implant placement to preserve bone around the radicular zone and maintain the alveolar process as much as possible.
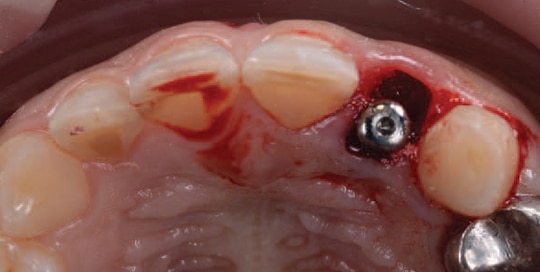

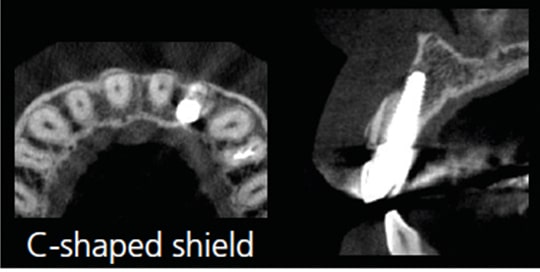
The root was mesial-distally sectioned with a diamond bur. The palatal root portion was fractured carefully toward the palate with a periotome so the buccal root portion would retain with an intact free gingival margin. The buccal root portion had a C-shape, leaving the mesial-buccal and distal-buccal transitional line angles intact due to the thick crestal bone. A 4.0×11.5-mm implant with a sandblasted and acid-etched surface incorporated with calcium ions was placed palatally and 4 mm below the most apical area of the buccal gingival margin (Figure 3A). The implant was carefully placed to avoid contact with the remaining buccal root portion, as such contact may result in failure. The 2-mm gap between the buccal root portion and implant was filled with synthetic bone mix of hydroxyapatite (60%) and beta-tricalcium phosphate (40%). The implant had an implant stability quotient of 65. A healing abutment was placed and, in order to maintain the gingival margin, a provisional restoration was bonded to the adjacent teeth without contacting the implant and opposing teeth (Figure 3B).
At the eight-week postoperative appointment, the implant stability quotient was more than 75, so an impression was taken. A screw-retained zirconia restoration was placed 12 weeks postoperatively, at which point clinical observation indicated the interdental papilla was maintained, as was the natural alveolar process.
Postoperative CBCT imaging at six months showed minimal or no bone loss on the buccal plate, and bundle bone that had been maintained with the buccal root portion due to use of the socket shield technique (Figure 4). A buccal root portion that is intact long-term may minimize bone loss due to preservation of bundle bone. However, if conventional extraction was done on a thick-thin buccal plate, not only would bundle bone be lost, bone grafts, guided bone regeneration, alternative ridge augmentation surgeries, and connective tissue grafts may be indicated due to fenestration.
CASE 2: CRESTAL THIN-RADICULAR THIN
A 50-year-old female presented with a failed upper anterior bridge due to missing teeth #7 and #10. Periapical radiographs showed the site #6 abutment was restorable, but the remaining teeth were nonvital (and with no ferrules), so they were deemed unrestorable (Figure 5).
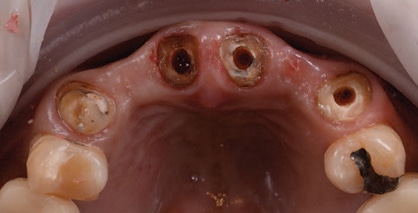
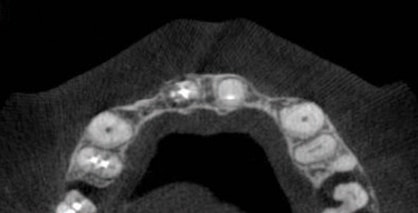
A horizontal view from the CBCT showed a thin ridge in the #7 and #10 areas, making implant placement difficult. Clinically, #8, #9 and #11, which were abutments for the bridge, were observed as thin-thin-type bone, thus, the amount of bone loss after extraction was likely to be significant (Figures 6A and 6B). The treatment plan was to use the socket shield technique5 on #8, #9 and #11 with immediate implant placement, followed by fabrication of a bridge.
After the coronal aspect of the labial roots of #8, #9 and #11 were probed to check the labial bone position, the roots of #8, #9 and #11 were sectioned mesial-distally with a diamond bur. The palatal half of the root was fractured toward the palatal and removed with a periotome. The mesial-buccal and distal-buccal transitional line angles of #8, #9 and #11 were removed to create a flat buccal root portion, along with an intact free gingival margin due to the thin crestal bone. Three 4.0×13-mm implants with a sandblasted and acid-etched surface incorporated with calcium ions were placed palatally and as parallel as possible for a screw-retained bridge. A synthetic bone mix of hydroxyapatite and beta-tricalcium phosphate was placed in the gap, which was less than 1 mm between the buccal root portions and implants. The entire procedure was done flaplessly. All three implants showed implant stability quotients of more than 75, and thus were immediately provisionalized.
Impressions were taken at the 12-week postoperative appointment, and a screw-retained zirconia bridge was placed 16 weeks postoperatively. There was overall light contact in centric occlusion, anterior guidance and lateral movements. The fit was checked via radiographs. In this case — which involved extraction, immediate implants and immediate provisionalization — the socket shield technique helped maintain the natural alveolar process. Treatment time from extraction to the final prosthesis was four months.
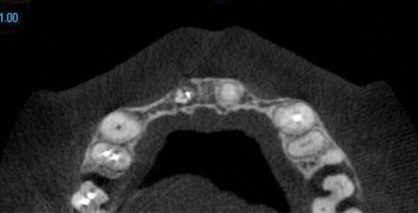
The patient was satisfied with the esthetic outcome (Figure 7). At the subsequent recall, the CBCT scan was compared with that of the preoperative image. In this crestal thin-radicular thin type — where significant buccal bone loss after extraction was likely to occur — keeping a small, thin buccal root portion with a bone graft using the socket shield technique maintained bundle bone and the natural alveolar process (Figure 8).


DISCUSSION
The patient in Case 1 had a thick-thin buccal bone, therefore, apical fenestration was predicted following extraction. If the socket shield technique was not the treatment of choice, surgeries (such as guided bone regeneration, bone grafting or other ridge augmentation procedures) may be necessary. As noted in the thin-thin type in Case 2, the patient may have a large, flattened bone defect after extraction, which suggests staged horizontal ridge augmentation as another option. Complications of bone augmentation procedures include soft tissue dehiscense, infection and additional augmentation procedures.17 Jensen et al17 note additional ridge augmentation procedures were needed in 37% of cases involving staged horizontal ridge augmentation. By comparison, the socket shield technique can be done simultaneously with extraction and can be effective in maintaining the natural alveolar process. Common complications include buccal/crestal bone loss (reported in 78.8% of cases), and shield exposure/failure (noted in 12.1% of cases).18
When the crest is thick, such as in Case 1, the buccal root portion has an intact C-shaped shield from the mesial to distal transitional line angles. The buccal root portion and implant surface are not in contact to help prevent complications. However, when the crest is thin, as in Case 2, making a C-shaped shield on the buccal root portion creates a potential risk for the implant surface to contact the shield (due to the thin buccal-lingual buccal bone). By making the mesial-distal width narrow, with a flat shield, the interdental papilla — along with a natural alveolar process — may be maintained. At the two-year follow-up, the examination revealed the interdental papilla and natural alveolar process were still maintained, even with a thin, scalloped case with a flat shield.
CONCLUSION
Prediction of postextraction buccal bone loss during the treatment planning phase is essential for immediate implant cases. Dividing the buccal bone into crestal bone and radicular bone, and determining the thickness — crestal thick-radicular thick, crestal thick-radicular thin, crestal thin-radicular thick or crestal thin-radicular thin — may prove helpful in treatment planning. This information may support therapy involving extraction, immediate implant placement and immediate provisionalization using the socket shield technique.
Crestal thick-radicular thin and crestal thin-radicular thin types are indicated for the socket shield technique. This approach helps maintain buccal bone, as well as the natural alveolar process, free gingival margin and interdental papilla — although it may have complications, including bone loss or buccal shield exposure and failure. As noted at the outset, this is a new technique that needs further validation. Thus, it is important to use an individualized approach to diagnosis and treatment planning, including a prediction of the extent of buccal bone loss following extraction. This approach may support additional indications for immediate implant placement — and with less trauma, shorter treatment and increased patient satisfaction.
REFERENCES
- Buser D, Chen ST. Implant Placement in Postextraction Sites. In: 20 Years of Guided Bone Regeneration in Implant Dentistry, 2nd edition. Buser D, ed. Quintessence Publishing Co Inc, Chicago: 2009;153–194.
- Buser D, Chappuis V, Belser UC, Chen S. Implant placement post extraction in esthetic single tooth sites: when immediate, when early, when late? Periodontol 2000. 2017;73:84–102.
- Becker W. Immediate implant placement: diagnosis, treatment planning and treatment steps for successful outcomes. J Calif Dent Assoc. 2005;4:303–310.
- Ross SB, Pette GA, Parker WB, Hardigan P. Gingival margin changes in maxillary anterior sites after single immediate implant placement and provisionalization: A 5-year retrospective study of 47 patients. Int J Oral Maxillofac Implants. 2014;29:127–134.
- Funato A, Salama MA, Ishikawa T, Garber DA, Salama H. Timing, positioning, and sequential staging in esthetic implant therapy: a four-dimensional perspective. Int J Periodontics Restorative Dent. 2007;8:313–323.
- Cosyn J, Eghbali A, Hanselaer L, et al. Four modalities of single implant treatment in the anterior maxilla: a clinical, radiographic, and aesthetic evaluation. Clin Implant Dent Relat Res. 2013;15:517–530.
- Hürzeler MB, Zuhr O, Schupbach P, Rebele SF, Emmanouilidis N, Fickl S. The socket-shield technique: A proof-of-principle report. J Clin Periodontol. 2010;37:855–862.
- Bäumer D, Zuhr O, Rebele S, Hürzeler M. Socket shield technique for immediate implant placement — clinical, radiographic and volumetric data after 5 years. Clin Oral Implants Res. 2017;28:1450–1458.
- Morton D, Chen ST, Martin WC, Levine RA, Buser D. Consensus statements and recommended clinical procedures regarding optimizing esthetic outcomes in implant dentistry. Int J Oral Maxillofac Implants. 2014;29(suppl):216–220.
- Braut V, Bornstein MM, Belser U, Buser D. Thickness of the anterior maxillary facial bone wall — a restrospective radiographic study using cone beam computed tomography. Int J Periodontics Restorative Dent. 2011;31:125–131.
- El Nahass H, Naiem S. Analysis of the dimensions of the labial bone wall in the anterior maxilla: A cone-beam computed tomography study. Clin Oral Implants Res. 2015;26:e57–e61.
- Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol. 2005;32:212–218.
- Ferrus F, Cecchinato D, Pjetursson EB, Lang NP, Sanz M, Lindhe J. Factors influencing ridge alterations following immediate implant placement into extraction sockets. Clin Oral Implant Res. 2010;21:22–29.
- Mandelaris GA, Vence BS, Rosenfeld AL, Forbes DP. A classification system for crestal and radicular dentoalveolar bone phenotypes. Int J Periodontics Restorative Dent. 2013;33:289–296.
- Kois JC. Predictable single-tooth peri-implant esthetics: five diagnostic keys. Compend Contin Educ Dent. 2004; 25:895–896,898,900.
- Evans CD, Chen ST. Esthetic outcomes of immediate implant placements. Clin Oral Implants Res. 2008;19:73–80.
- Jensen AT, Jensen SS, Worsaae N. Complications related to bone augmentation procedures of localized defects in the alveolar ridge. A retrospective study. Oral Maxillofac Surg. 2016;20:115–122.
- Gharpure AS, Bhatavadekar NG. Current evidence on the socket-shield technique: a systematic review. J Oral Implantol. 2017;43:395–403.
From Decisions in Dentistry. March 2019;5(3):26–29.

