

Soft Tissue Graft Alternatives for Treating Mucogingival Defects
While autogenous soft tissue grafts remain the gold standard, non-autogenous graft alternatives show promise for treating mucogingival defects.
PURCHASE COURSE
This course was published in the January 2023 issue and expires January 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the January 2023 issue and expires January 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 490
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss mucogingival defects, along with their prevalence and etiology.
- Describe various management approaches when treating mucogingival defects.
- Explain alternative grafting techniques for patients presenting with gingival recession or other mucogingival conditions.
Mucogingival defects are characterized by the deviation of the normal dimension and morphology between the gingival margin and mucogingival junction. Gingival recession and lack of attached gingiva are among the most commonly diagnosed mucogingival defects. Gingival recession is described as the apical migration of the gingiva beyond the cementoenamel junction and appears to be prevalent in more than 50% of adults.1 If left untreated, the prevalence, severity and extent of recession could increase with age.2 It has been observed that accumulation of bacterial plaque around the gingival margin could lead to periodontal inflammation and tissue breakdown, resulting in gingival recession.3 However, contributing factors — including toothbrush abrasion, history of orthodontic therapy, aberrant frenal attachment, and lack of attached gingiva — can also lead to recession.4–7 The undesired consequences of gingival recession include dentinal hypersensitivity, poor esthetics, root caries, and development of other mucogingival defects, such as lack of attached gingiva, rendering the area vulnerable to inflammation and plaque retention.8
Attached gingiva is the zone of keratinized tissue extending from the free gingival margin to the alveolar mucosa that is firmly attached to the underlying bone. Attached gingiva increases resistance to injury and stabilizes the gingival margin; it also helps bind the margin and enhances plaque removal around gingival margins.9 Lack of attached gingiva can be diagnosed when, upon probing, the periodontal probe invades the mucogingival junction. Less than 2 mm of attached gingiva has been shown to exhibit clinical gingival inflammation and accelerate tissue breakdown.7
Biologic width is the dimension of the soft tissue that extends from the sulcus to the crest of the alveolar bone. The sum of this epithelial and connective tissue is approximately 2 mm.10 Violations of biologic width often occur when restorative margins are extended far below the gingival crest, impinging on the attachment apparatus. This could lead to chronic inflammation and recession, which could be worse in patients with a thin gingival phenotype.11 When considering subgingival restorations, it is imperative to maintain at least a 2 mm zone of attached gingiva to minimize gingival inflammation and tissue breakdown and help maintain gingival health.12

SOFT TISSUE AUGMENTATION
Gingival recession and lack of attached gingiva can coexist; therefore, it is important to treat these defects to prevent further tissue and tooth loss. Soft tissue augmentation has been commonly used for managing mucogingival defects. The techniques for treating gingival recession have evolved from traditional procedures, such as the semilunar technique, coronally advanced flap, lateral pedicle flap, and double papilla flap, to more minimally invasive methods, such as tunneling and vestibular incision subperiosteal tunnel access techniques. These approaches can often be used in combination with an autograft, allograft or xenograft.
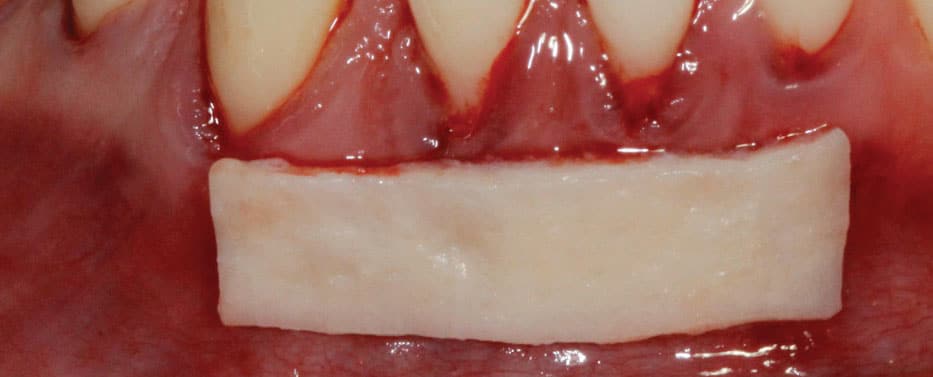
Autogenous grafts, such as free gingival grafts, are traditionally used for the purpose of gaining attached gingiva, while subepithelial connective tissue grafts (SCTG) are considered the gold standard for root coverage procedures.13–15 This could be attributed to SCTG’s properties, predictability in clinical attachment and keratinized tissue gain, and long-term result.15,16 Autogenous grafts are harvested from either the palate (between the canine and premolar region) or maxillary tuberosity (Figure 1), requiring the need for an additional surgical site.17 Additionally, the quality and quantity of tissue obtained can vary depending on palatal thickness, thereby potentially compromising the surgical outcome and limiting the number of teeth that can be treated in a single surgical procedure.18

AUTOGENOUS GRAFT ALTERNATIVES
As an alternative, non-autogenous soft tissue grafts — such as allografts and xenografts — are gaining popularity due to their palate-free approach. Their advantages include reduced morbidity, shorter chairtime, unlimited availability, and consistent graft thickness.19 The advantages and comparable outcomes of non-autogenous soft tissue grafts have led clinicians to utilize this alternative method when treating mucogingival defects.16 Commonly used non-autogenous grafts include acellular dermal matrix (ADM), enamel matrix derivatives (EMD), and xenogeneic collagen matrix (XCM).16,20,21
Acellular Dermal Matrix — As a decellularized regenerative human dermal tissue matrix, ADM has historically been used by surgeons for treating burns.22 It is composed of the dermal layer and extracellular matrix of thin layers of donated skin that have had the epidermal layer and cellular material removed, which minimizes immunological response in ADM recipients. It consists of a structurally intact connective tissue matrix composed of type I collagen, which acts as a scaffold to facilitate the migration of, and repopulation by, the host’s fibroblasts, blood vessels and epithelial cells. It is subsequently replaced by, and fully integrated into, the host tissues.23,24 Studies have reported similar recession coverage and keratinized tissue gain when comparing ADM with SCTG using various techniques.25,26 Furthermore, the 2015 consensus report from the American Academy of Periodontology Regeneration Workshop also concluded that while SCTG provides the best root coverage outcomes, ADM can be used as an alternative.16
Enamel Matrix Derivative — An EMD graft is derived from embryonal enamel of porcine origin, based on the high degree of homology between porcine and human enamel proteins.27 The ability of EMD to induce acellular cementum formation during tooth development and eruption is also why it is used as a clinical treatment to promote periodontal regeneration.28 This graft material is available in a gel formulation containing porcine-derived enamel matrix proteins, propylene glycol alginate and water.29 Studies investigating the role of EMD and its potential for treating gingival recession alone, and in conjunction with SCTG, reported that EMD can provide root coverage and keratinized tissue gain in both scenarios.30,31
Xenogeneic Collagen Matrix — Made with types I and III collagen without cross-linking or chemical treatment, XCM is a resorbable, two-layer, three-dimensional porcine-derived collagen. It has two components, a compact structure of denser collagen and smooth texture to enhance wound healing and facilitate cell adhesion, and a porous surface facing the host tissue that supports clot formation, tissue integration and angiogenesis.32 This material has been shown to promote regeneration of keratinized gingiva (in both width and thickness), not only around natural teeth, but also around dental implants. As a result, it is commonly used for treating gingival recession,33 as it has shown promising results and is thought to be a suitable substitute for mucogingival surgical procedures.

CASE REPORT 1
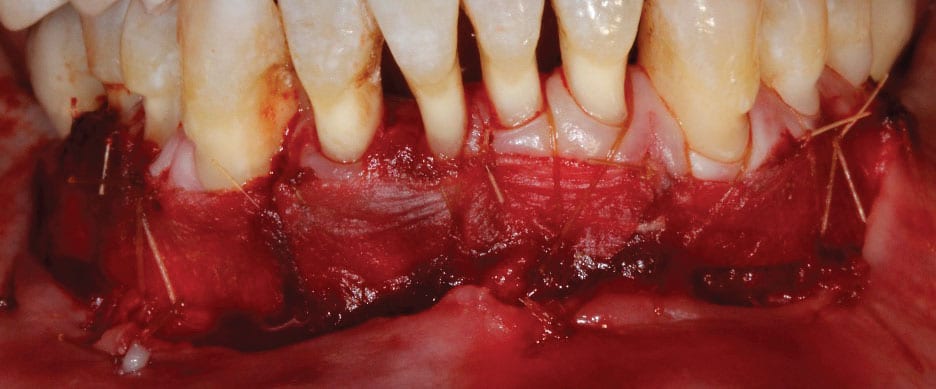
Figure 2A shows a patient with generalized recession and a thin phenotype extending from teeth #19 to 30. Additionally, there is lack of attached gingiva in the areas of #19, 25, 26 and 30. Teeth #19 and 30 presented with Grade I incipient furcation involvement. The primary goal of the procedure was to gain root coverage, with a secondary goal of gaining attached gingiva. Due to the number of teeth involved, ADM was selected as the graft material of choice.
A subperiosteal tunneling technique was used extending from teeth #19 to 30. Care was taken to ensure passive coronal mobility of the tunnel. Figure 2B depicts the tunneled recipient site prior to ADM insertion. Once the ADM was inserted, the tunnel was coronally sutured at the level of the cementoenamel junction with non-resorbable 5-0 polypropylene sutures. A subpapillary continuous sling suturing technique was utilized to suture the tunnel to the graft, with external and internal application of EMD (Figure 2C). A surgical dressing was not required in this case, as the graft was secured to the overlying soft tissue and remained unexposed.
Postoperative instructions included a soft diet, no brushing and flossing in the area, and utilization of an antibacterial mouthrinse. The sutures were retained for four weeks, and oral hygiene instructions were reviewed with the patient at the four-week postoperative visit. The three-month follow-up appointment showed complete root coverage in the anterior region, and a wide zone of attached gingiva in the area of teeth #19, 25 and 26 (where previously it was absent). An improvement in the patient’s gingival phenotype was also observed (Figure 2D).

CASE REPORT 2
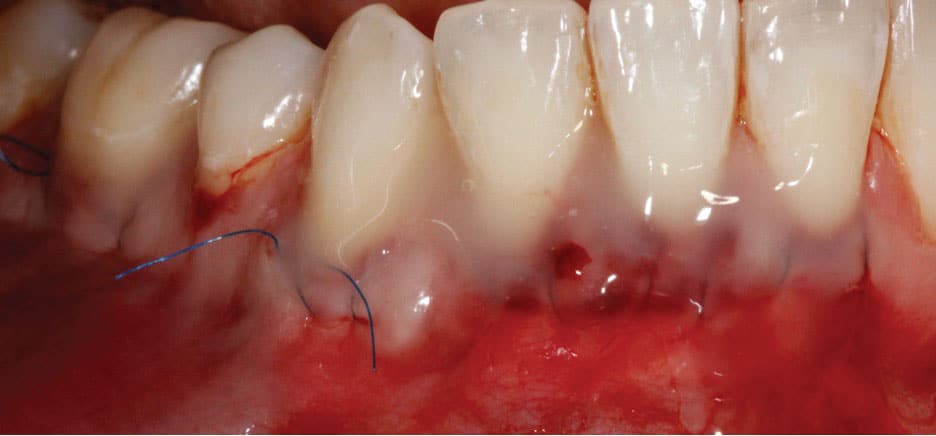
Figure 3A depicts an older adult patient with a history of periodontitis resulting in generalized interdental attachment loss, gingival recession, and a lack of attached gingiva that resulted in a shallow vestibule. The patient’s lack of attached gingiva led to persistent inflammation and sensitivity around the gingiva. Due to the extent of interdental attachment loss, the predictability of obtaining root coverage was significantly reduced. Therefore, the primary goal of the procedure was to increase the zone of attached gingiva, thereby improving vestibular depth and preventing her recession from progressing. This would also support the patient’s oral hygiene efforts.
The recipient site was prepared by performing a split-thickness dissection from teeth #19 to 30. The alveolar mucosa was sutured to the periosteum using resorbable chromic gut sutures. Next, XCM was secured to the recipient site with resorbable 5-0 chromic gut sutures (Figure 3B). A surgical dressing was placed over the recipient site because the graft was secured to the recipient bed and left exposed. This also protected the area from external irritation or trauma, allowing the site to heal uneventfully.
Postoperative instructions included a soft diet, no brushing and flossing in the area, and utilization of an antibacterial mouthrinse. The surgical dressing and remaining sutures were removed after two weeks. At the six-month follow-up appointment, a wide zone of attached gingiva was observed extending from teeth #19 to 30. Restoration of vestibular depth and improvement in the patient’s soft tissue phenotype were also noted (Figure 3C). Gingival sensitivity and tissue susceptibility to inflammation were significantly improved following the procedure.

CONCLUSION
Autogenous soft tissue grafts remain the gold standard for managing mucogingival defects; however, they have limitations in terms of quality and quantity of palatal donor tissue. As an alternative, non-autogenous soft tissue grafts can be used to overcome the aforementioned limitations. As a result, these options are gaining popularity due to the palate-free approach, the materials’ unlimited availability, and their ability to treat larger areas.
Non-autogenous tissue grafts eliminate the need for a second surgical site, thereby improving patients’ overall experience and tolerance. As documented in the literature, ADM, EMD and XCM represent viable materials that provide results similar to autogenous soft tissue grafts. That said, in-depth knowledge of the indications of the various graft alternatives is crucial prior to selection and application. As with all facets of care, it is important to integrate evidence-based dentistry and patient expectations when selecting the appropriate surgical approach to treating mucogingival defects.
REFERENCES
- Loe J, Anerud A, Boysen H. The natural history of periodontal disease in man: prevalence, severity, and extent of gingival recession. J Periodontol. 1992;63:489–495.
- Serino G, Wennström JL, Lindhe J, Eneroth L. The prevalence and distribution of gingival recession in subjects with a high standard of oral hygiene. J Clin Periodontol. 1994;21:57–63.
- Baker DL, Seymour GJ. The possible pathogenesis of gingival recession. A histological study of induced recession in the rat. J Clin Periodontol. 1976;3:208–219.
- Litonjua LA, Andreana S, Bush PJ, Cohen RE. Toothbrushing and gingival recession. Int Dent J. 2003;53:67–72.
- Steiner GG, Pearson JK, Ainamo J. Changes of the marginal periodontium as a result of labial tooth movement in monkeys. J Periodontol. 1981;52:314–320.
- Ewen SJ. Frena: their roles especially in periodontics. N Y State Dent J. 1968;34:626–630.
- Lang NP, Loe H. The relationship between the width of keratinized gingiva and gingival health. J Periodontol. 1972;43;623–627.
- Clerehugh V, Tugnait A, Genco RJ. Periodontology at a Glance. Oxford: Wiley-Blackwell; 2009:64,66.
- Carnio J, Camargo PM, Passanezi E. Increasing the apico-coronal dimension of attached gingiva using the modified apically repositioned flap technique: a case series with a 6-month follow-up. J Periodontol. 2007;78:1825–1830.
- Gargiulo AW, Wentz FM, Orban B. Dimensions and relations of the dentogingival junction in humans. J Periodontol. 1961;32:261–267.
- Jorgic-Srdjak K, Plancak D, Maricevic T, Dragoo MR, Bosnjak A. Periodontal and prosthetic aspect of biological width Part I: Violation of biologic width. Acta Stomatol Croat. 2000;34:195–197.
- Stetler KJ, Bissada NF. Significance of the width of keratinized gingiva on the periodontal status of teeth with submarginal restorations. J Periodontol. 1987;58:696–700.
- Nabers JM. Free gingival grafts. Periodontics. 1966;4:243–245.
- Langer B, Langer L. Subepithelial connective tissue graft technique for root coverage. J Periodontol. 1985;56:715–720.
- Chambrone L, Chambrone D, Pustiglioni FE, Chambrone LA, Lima LA. Can subepithelial connective tissue grafts be considered the gold standard procedure in the treatment of Miller Class I and II recession-type defects? J Dent. 2008;36:659–671.
- Tatakis DN, Chambrone L, Allen EP, et al. Periodontal soft tissue root coverage procedures: a consensus report from the AAP Regeneration Workshop. J Periodontol. 2015;86(Suppl 2):S52–S55.
- Studer SP, Allen EP, Rees TC, Kouba A. The thickness of masticatory mucosa in the human hard palate and tuberosity as potential donor sites for ridge augmentation procedures. J Periodontol. 1997;68:145–151.
- Aichelmann-Reidy ME, Yukna RA, Evans GH, Nasr HF, Mayer ET. Clinical evaluation of acellular allograft dermis for the treatment of human gingival recession. J Periodontol. 2001;72:998–1005.
- Suárez-López Del Amo F, Rodriguez JC, Asa’ad F, Wang HL. Comparison of two soft tissue substitutes for the treatment of gingival recession defects: an animal histological study. J Appl Oral Sci. 2019;27:e20180584.
- Rotundo R, Pini-Prato G. Use of a new collagen matrix (mucograft) for the treatment of multiple gingival recessions: case reports. Int J Periodontics Restorative Dent. 2012;32:413–419.
- McGuire MK, Scheyer ET, Nunn M. Evaluation of human recession defects treated with coronally advanced flaps and either enamel matrix derivative or connective tissue: comparison of clinical parameters at 10 years. J Periodontol. 2012;83:1353–1362.
- Wei PC, Laurell L, Geivelis M, Lingen MW, Maddalozzo D. Acellular dermal matrix allografts to achieve increased attached gingiva. Part 1. A clinical study. J Periodontol. 2000;71:1297–1305.
- Cummings LC, Kaldahl WB, Allen EP. Histologic evaluation of autogenous connective tissue and acellular dermal matrix grafts in humans. J Periodontol. 2005;76:178–186.
- Gallagher SI, Matthews DC. Acellular dermal matrix and subepithelial connective tissue grafts for root coverage: A systematic review. J Indian Soc Periodontol. 2017;21:439–448.
- Gapski R, Parks CA, Wang HL. Acellular dermal matrix for mucogingival surgery: A meta-analysis. J Periodontol. 2005;76:1814–1822.
- Moslemi N, Jazi MM, Haghighati F, Morovati SP, Jamali R. Acellular dermal matrix allograft versus subepithelial connective tissue graft in treatment of gingival recessions: a 5-year randomized clinical study. J Clin Periodontal. 2011;38:1122–1129.
- Esposito M, Grusovin MG, Papanikolaou N, Coulthard P, Worthington HV. Enamel matrix derivative (Emdogain) for periodontal tissue regeneration in intrabony defects. Cochrane Database Syst Rev. 2009;2009:CD003875.
- Hammarström L, Heijl L, Gestrelius S. Periodontal regeneration in a buccal dehiscence model in monkeys after application of enamel matrix proteins. J Clin Periodontol. 1997;24:669–677.
- Brookes SJ, Robinson C, Kirkham J, Bonnas WA. Biochemistry and molecular biology of amelogenin proteins of developing dental enamel. Arch Oral Biol. 1995;40:1–14.
- Rasperini G, Silvestri M, Schenk RK, Nevins ML. Clinical and histologic evaluation of human gingival recession treated with a subepithelial connective tissue graft and enamel matrix derivative (Emdogain): a case report. Int J Periodontics Restorative Dent. 2000;20:269–275.
- Alkan EA, Parlar A. EMD or subepithelial connective tissue graft for the treatment of single gingival recessions: a pilot study. J Periodontal Res. 2011;46:637–642.
- Nevins M, Nevins ML, Kim SW, Schupbach P, Kim DM. The use of mucograft collagen matrix to augment the zone of keratinized tissue around teeth: a pilot study. Int J Periodontics Restorative Dent. 2011;31:367–373.
- Atieh MA, Alsabeeha N, Tawse-Smith A, Payne AG. Xenogeneic collagen matrix for periodontal plastic surgery procedures: a systematic review and meta-analysis. J Periodontal Res. 2016;51:438–452.
From Decisions in Dentistry. January 2023;9(1)26-29.

