
Simplifying the Confusion of Overdenture Restorative Space
Practice guidelines — based on the current literature — are provided on restorative space requirements for implant mandibular overdentures.
Mandibular implant overdentures are the standard of care for complete denture patients who may not have the finances to proceed with a more complex approach. This treatment modality is also well liked by patients.1 In order to properly restore the patient, enough restorative space for the prosthetic components is needed.
Overdenture restorative space was initially defined by Ahuja et al2 as “the three-dimensional (3D) oral space available to receive the proposed prosthodontic restoration … For implant overdenture patients, this space must accommodate a denture base of sufficient dimensions, appropriately positioned denture teeth, and an implant attachment system.”
The current literature on overdenture restorative space notes varying restorative space numbers. Chaimattayompol and Arbree3 state a minimal overdenture restorative space as low at 7.17 mm for unsplinted overdentures while Misch4 recommends 12 mm as the minimum restorative space for unsplinted overdentures. Literature on splinted overdentures cites14 mm for bar and clip overdentures and 16 mm for a bar with ball attachments.4,5 There seems to be no disagreement regarding splinted overdentures, however, there is a great deal of variability surrounding the minimum restorative space for unsplinted overdentures. This brief review of the available literature intends to determine the cause of this inconsistency, as well as provide practical guidelines.
MATERIAL AND METHODS
An electronic search was completed in the following databases for studies published in English from January 1980 until December 2024: Science Direct, Pub Med, EBSCO host Academic Search Complete, ProQuest, Cochrane Library, GALILEO Search, Web of Science, Google Scholar, and the Wiley Online Library. The search strategy included the following key word combinations: “overdenture restorative space,” “overdenture interarch space,” and the following Boolean search alternatives: “overdenture” AND “restorative” AND “space,” “overdenture” AND “interarch” AND “space.”
All abstracts were reviewed for inclusion by two independent and calibrated reviewers. Afterward, the two reviewers met to discuss and evaluate the papers for full-text reading.
The following inclusion criteria were used:
- Studies discussing or describing overdenture restorative space
- Studies defining overdenture restorative space
- Systematic reviews regarding overdentures
- Papers about success and effectiveness of overdentures
The following exclusion criteria were used:
- Papers that quoted restorative space requirements from other original sources
DISCUSSION
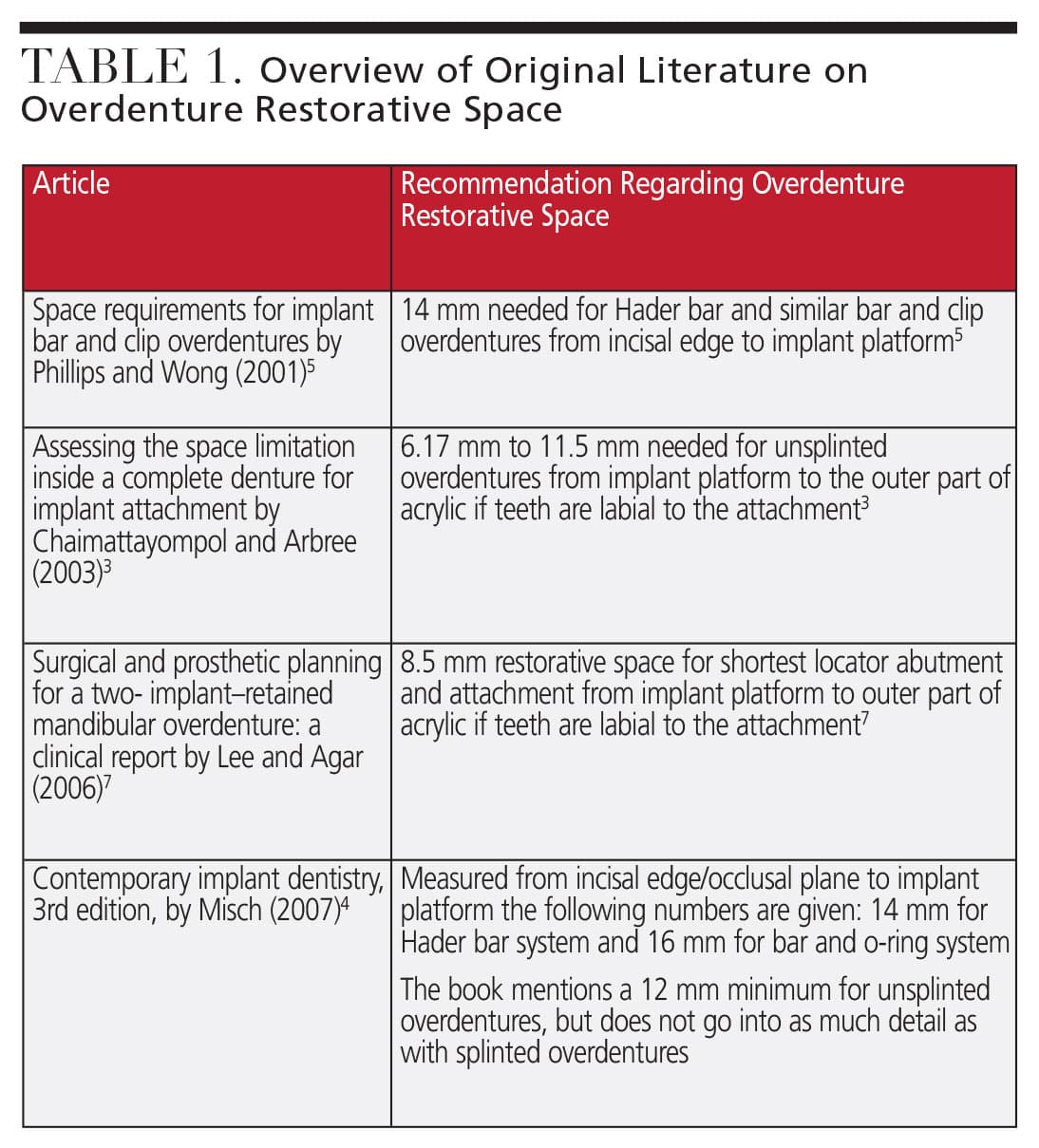
The consequences of inadequate treatment planning for restorative space in overdentures has been discussed.6,7 Bidra6 specifies that “inadequate prosthetic space can result in problems such as an overcontoured prosthesis, compromise in the neutral zone and tongue space, fractured prosthetic teeth, fractured prostheses, excessive occlusal vertical dimension … need for additional corrective surgeries and overall patient dissatisfaction.” After dissection of the information, we concluded that the variation in numbers for overdenture restorative space is simply because different authors use different reference points as noted in Table 1 (page 12). Furthermore, there is a great degree of variability in the types of overdenture abutments and bar designs available in the market, all of which have different dimensions and therefore different restorative space requirements.
 Most clinicians prefer to add 1 to 2 mm of additional restorative space above the minimal recommendations to compensate for any errors in fabrication of surgical bone reduction guide or errors in fabrication of reference denture. An added benefit of adding 1 to 2 mm above the minimal recommendation is because this allows the clinician a wide range of restorative options to choose from. The following minimal recommendations are based on a review of the literature:
Most clinicians prefer to add 1 to 2 mm of additional restorative space above the minimal recommendations to compensate for any errors in fabrication of surgical bone reduction guide or errors in fabrication of reference denture. An added benefit of adding 1 to 2 mm above the minimal recommendation is because this allows the clinician a wide range of restorative options to choose from. The following minimal recommendations are based on a review of the literature:
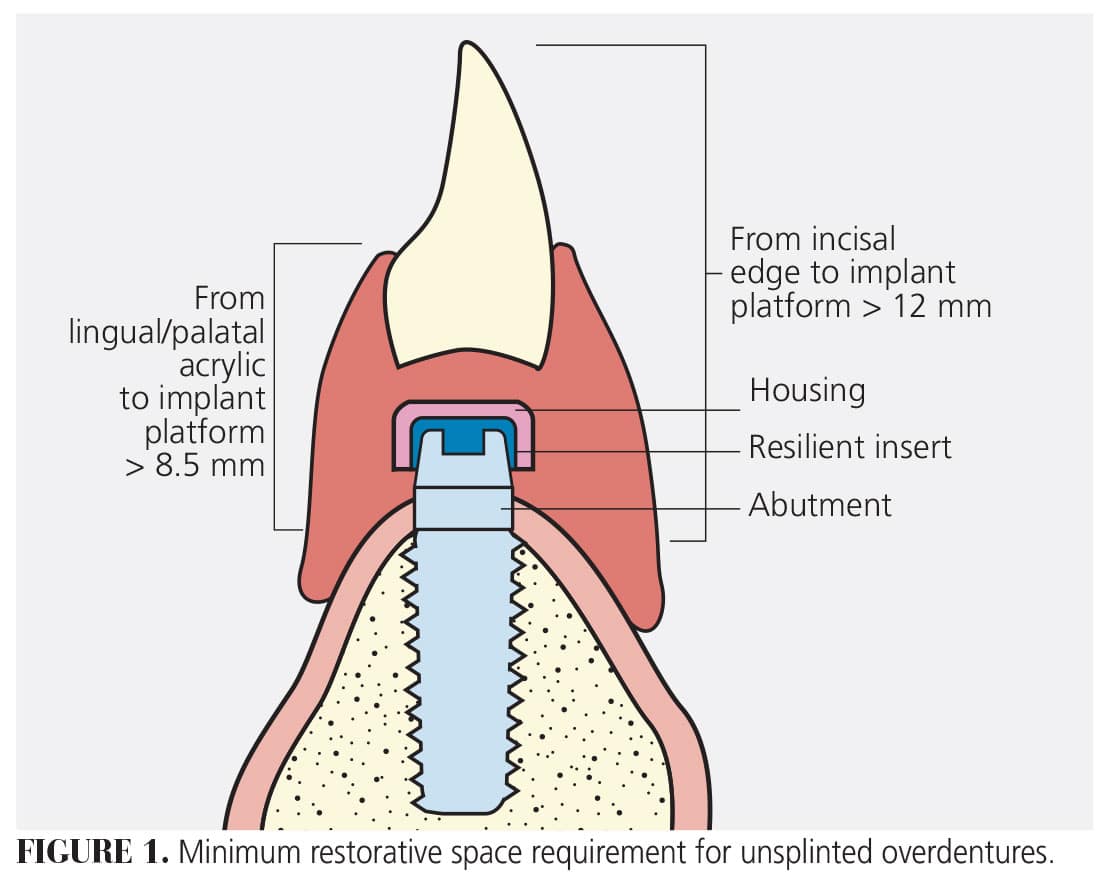
Unsplinted Overdentures: 12 mm from incisal edge/occlusal plane to implant platform and 8.5 mm from implant platform the top of acrylic if teeth are placed labial or buccal to the ridge. This allows for enough space for the solitary abutment, the housing, and at least 2 mm of acrylic above the housing (Figure 1).
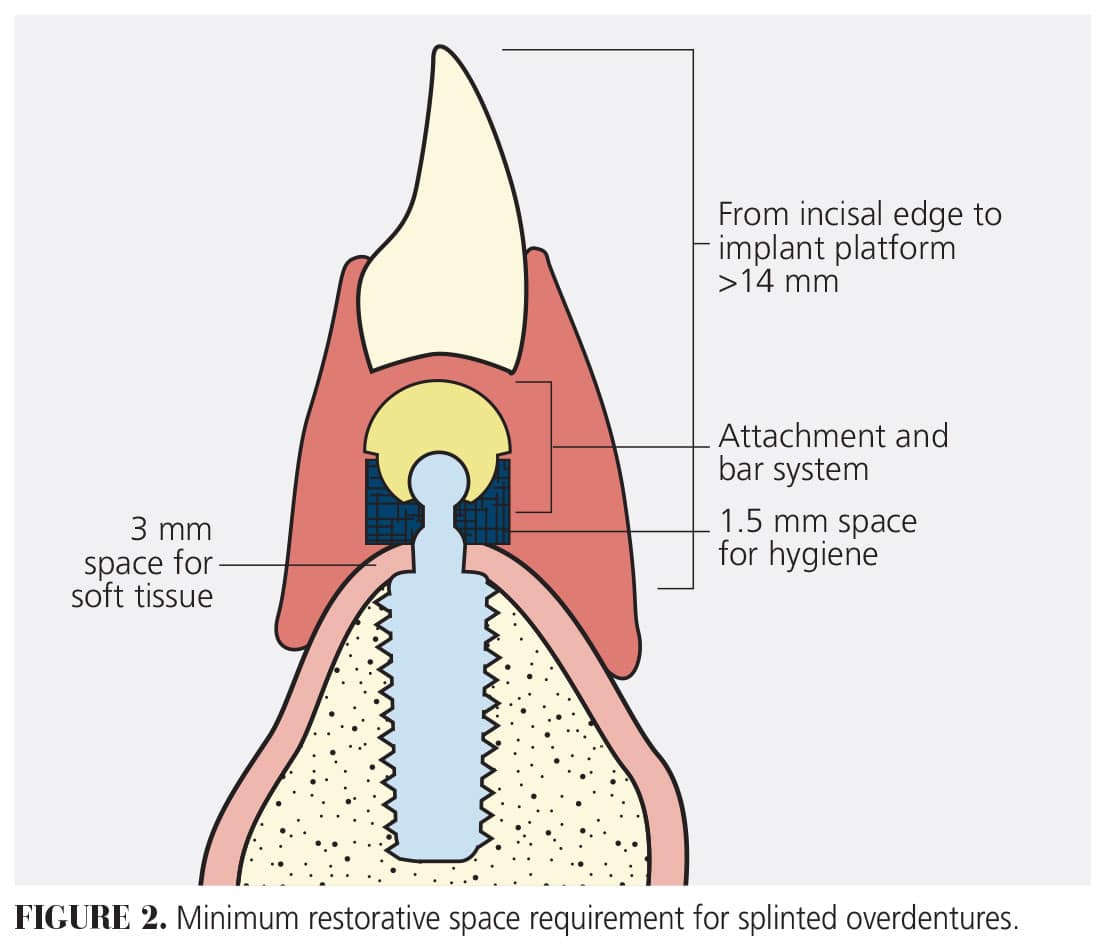
Splinted Overdentures: 14 mm for Hader bar system and 16 mm for bar and o-ring system from implant platform to incisal/occlusal plane. Some labs that provide these services give guidelines on the amount of restorative space necessary. Those labs have guidelines of restorative space for bar restorations, however, some guidelines are given for the space needed for the bar component only.
To determine how much space is necessary, use 14 mm as the baseline based on a 4.5 mm Hader bar system as described by Phillips and Wong5 that consists of a metal rider, nylon clip, and the Hader bar. The milled locator bar requires 5 mm for the bar system, so a minimum of 14.5 mm is required or restorative space from incisal edge to implant platform. This approach will allow enough room for the components (Figure 2, page 10) without having to remember all the numbers in order to calculate restorative space for the desired prosthesis.
No in vitro studies discuss a difference in restorative space between anterior teeth and posterior teeth, however, to prevent breakage of the prosthesis or over-reduction of the intaglio of the prosthetic teeth, follow the same recommendations stated for both anterior and posterior teeth.
SUGGESTED GUIDELINES
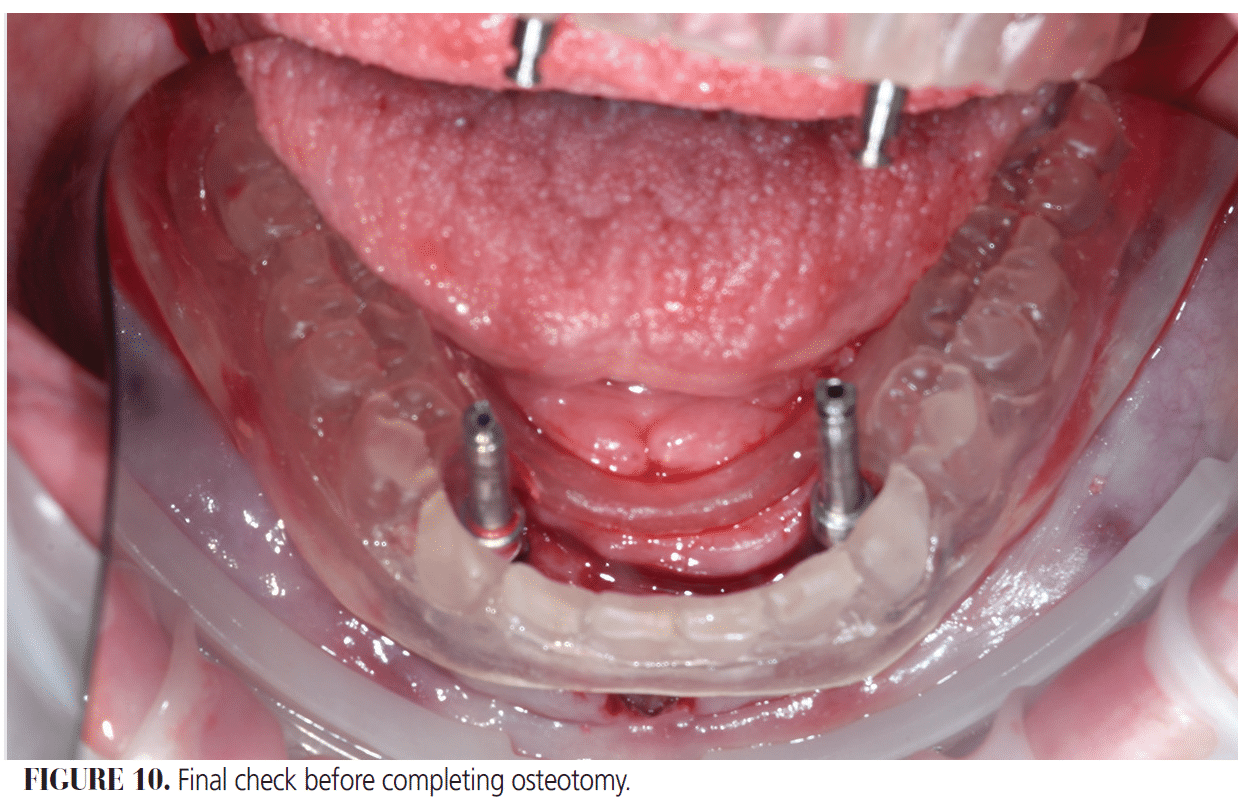
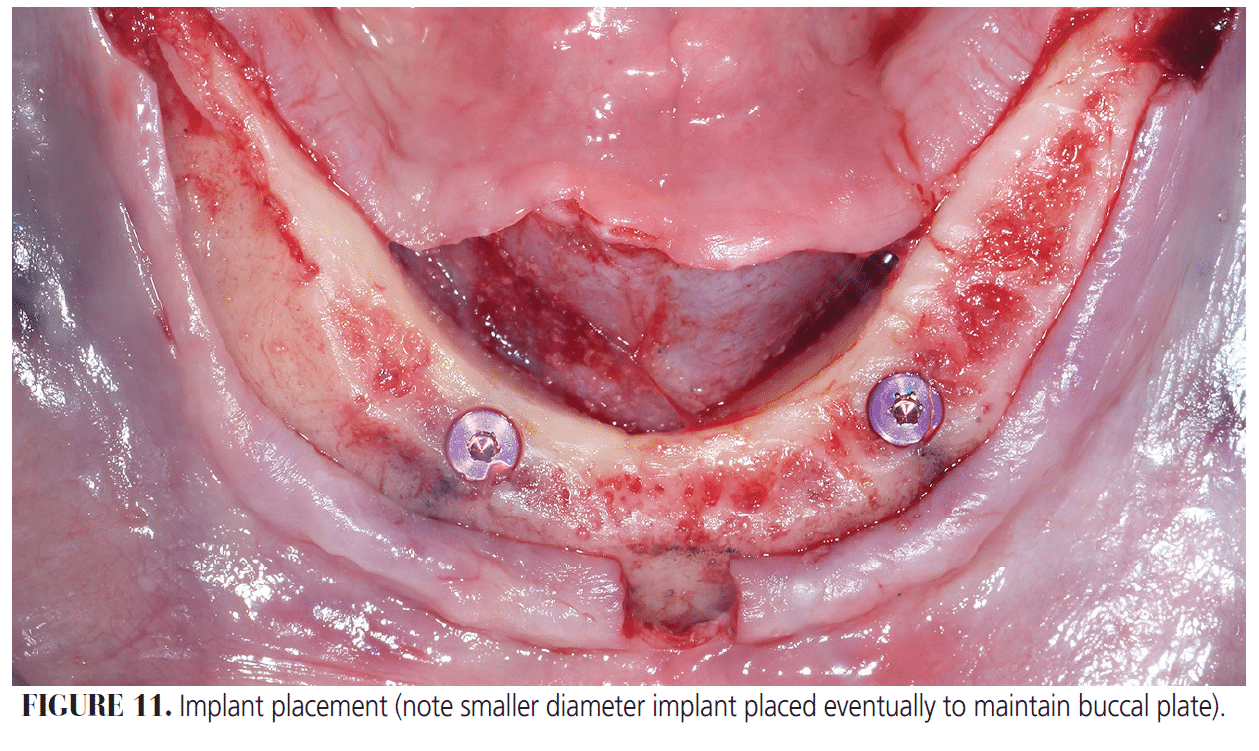
Based on this brief review of the literature, we suggest clinicians consider these practical guidelines, which are illustrated in Figures 3 through 11.
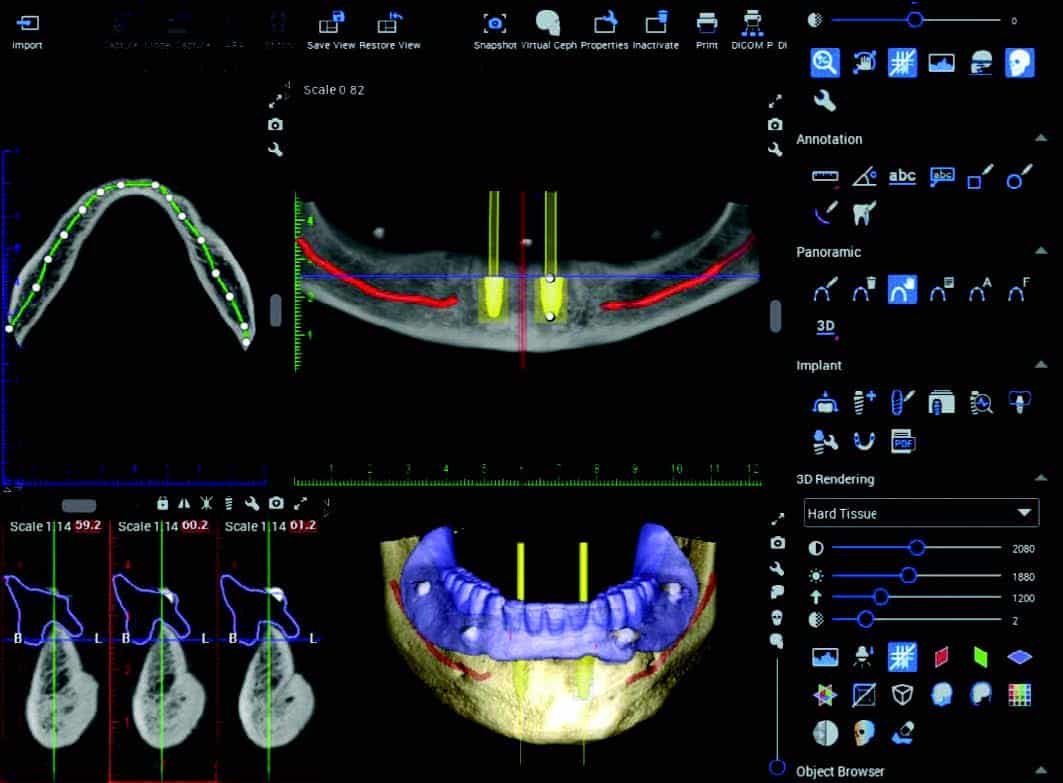
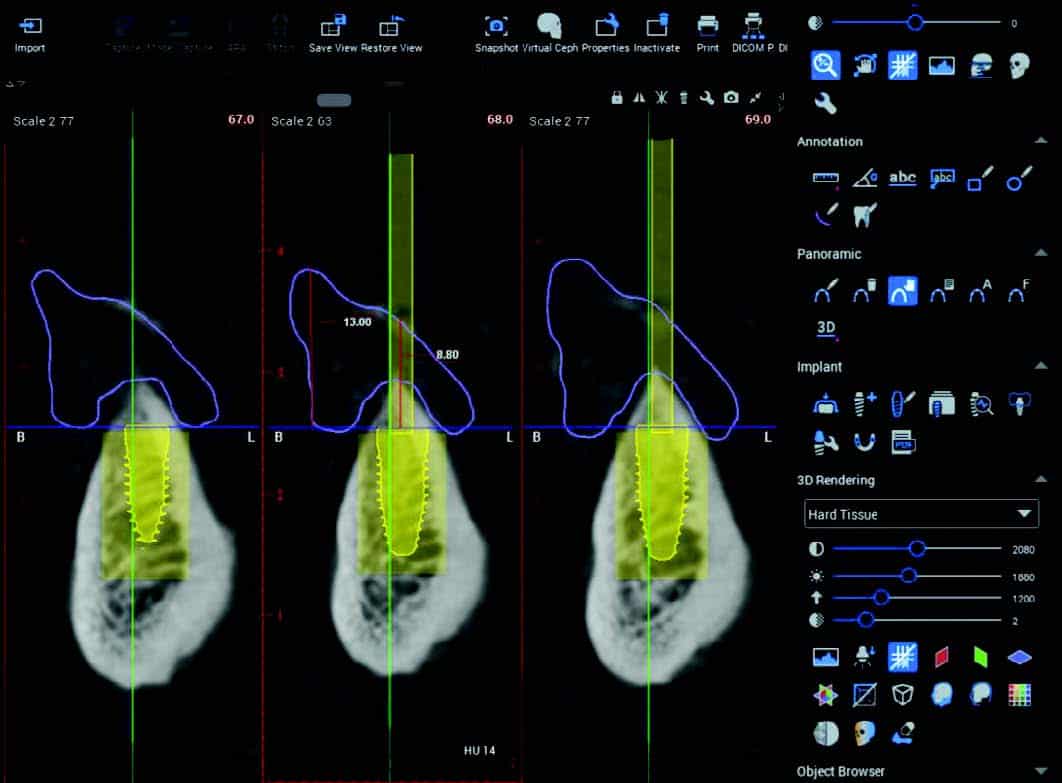
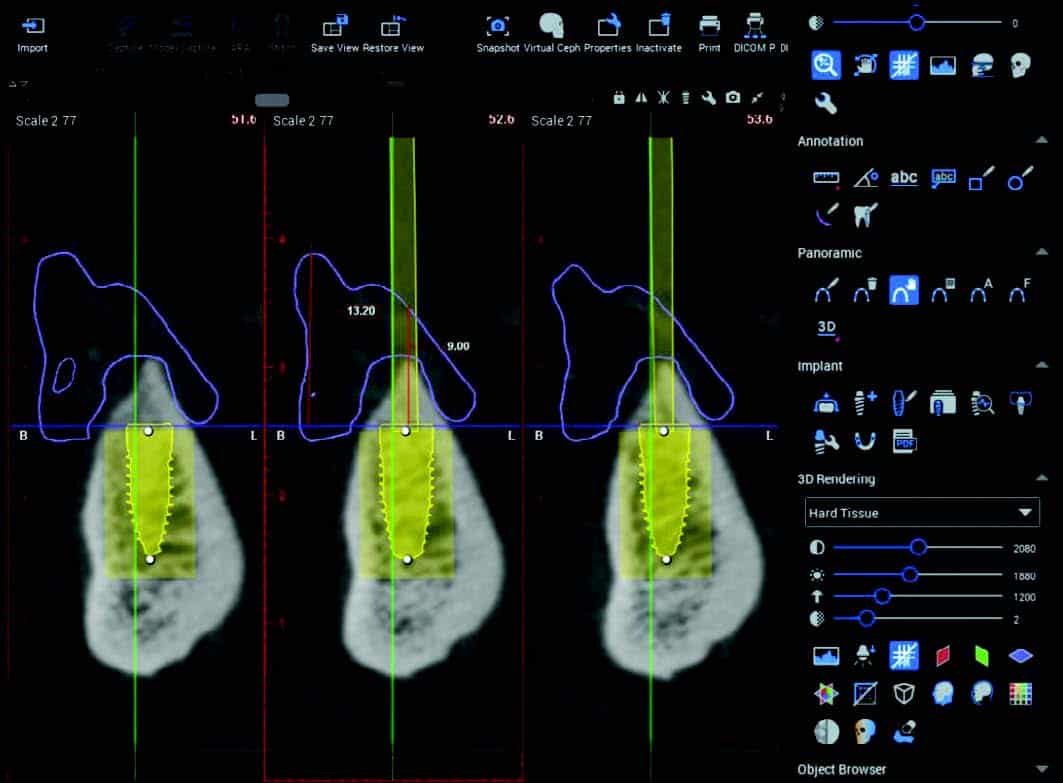
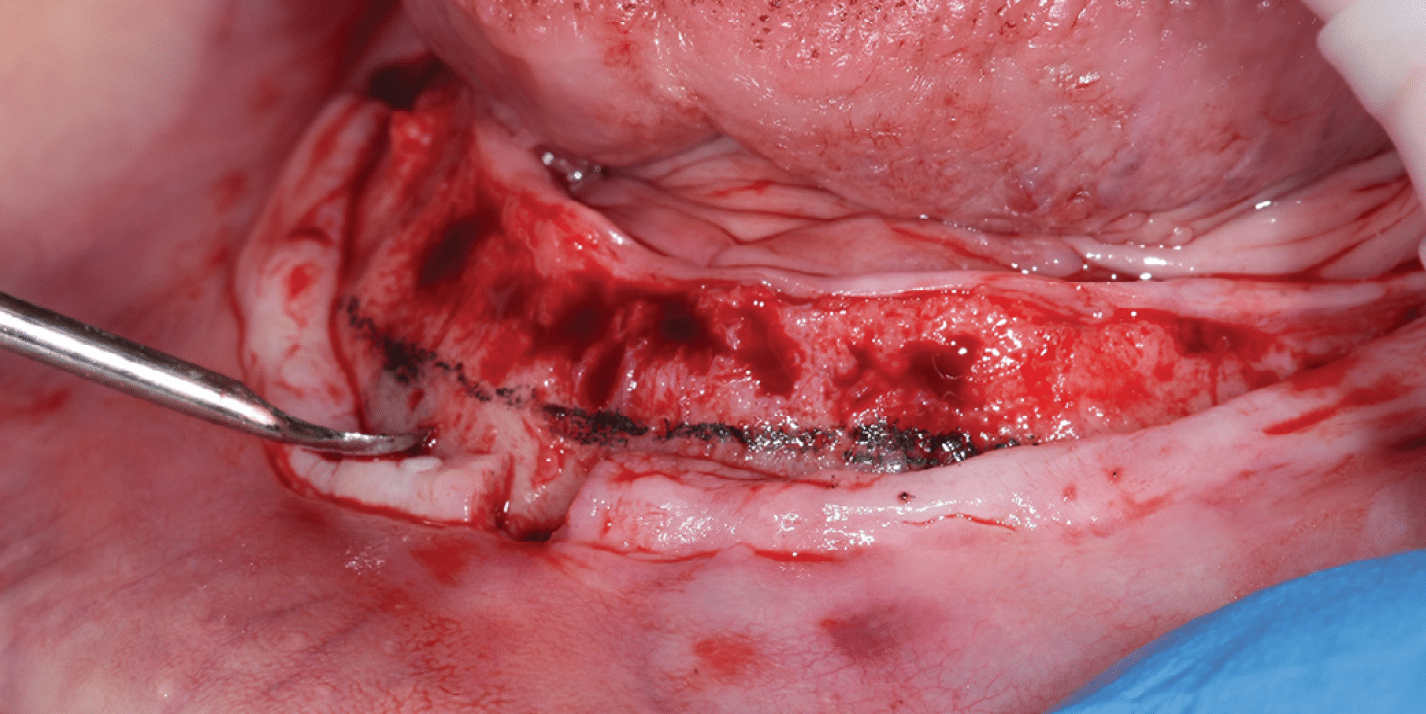
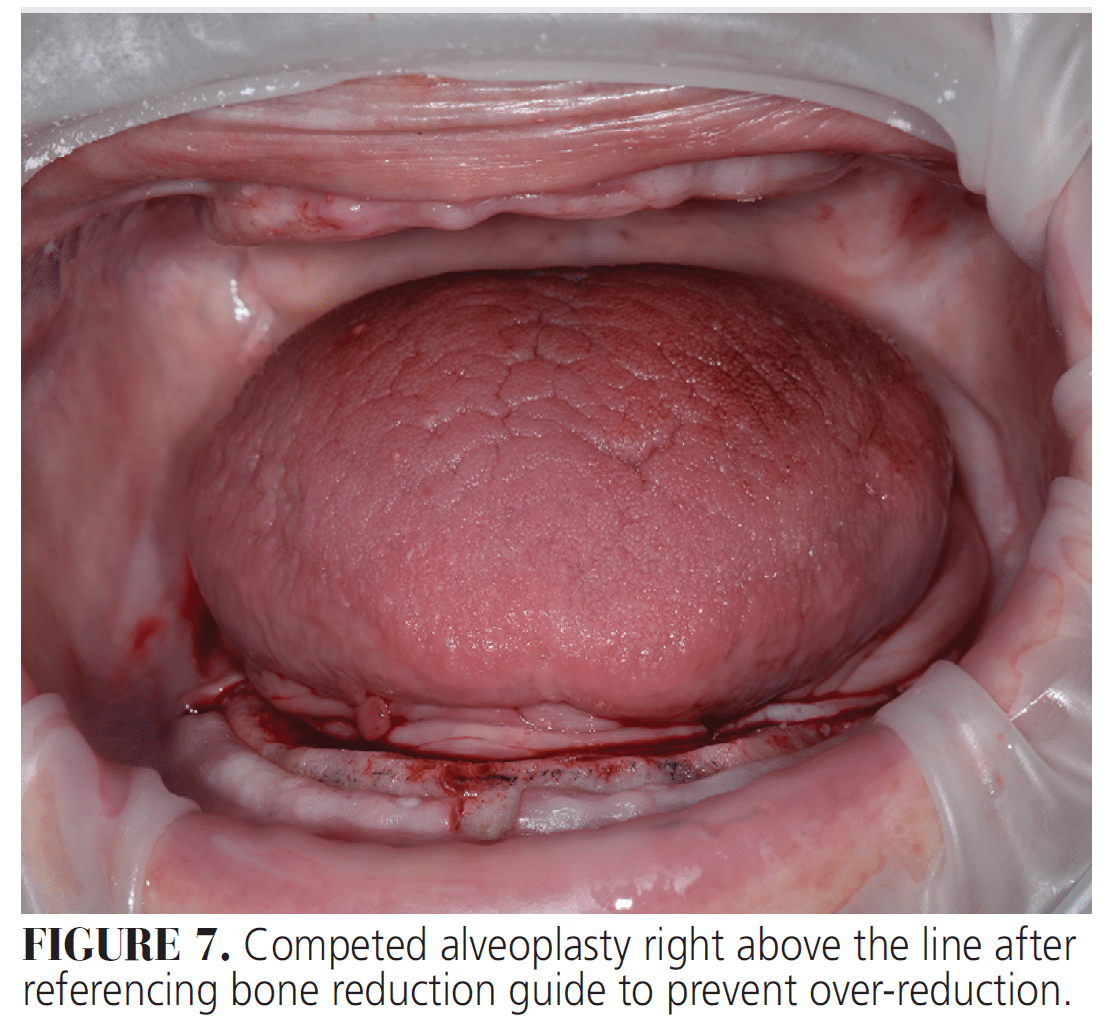
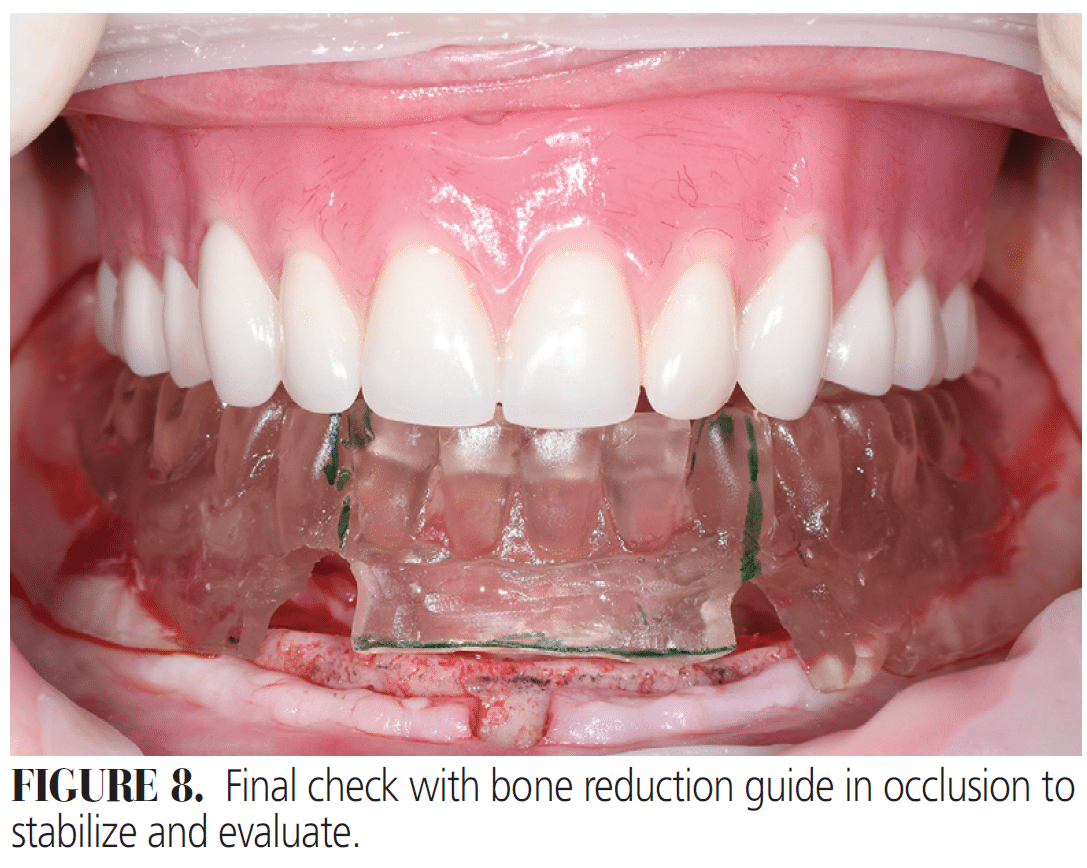
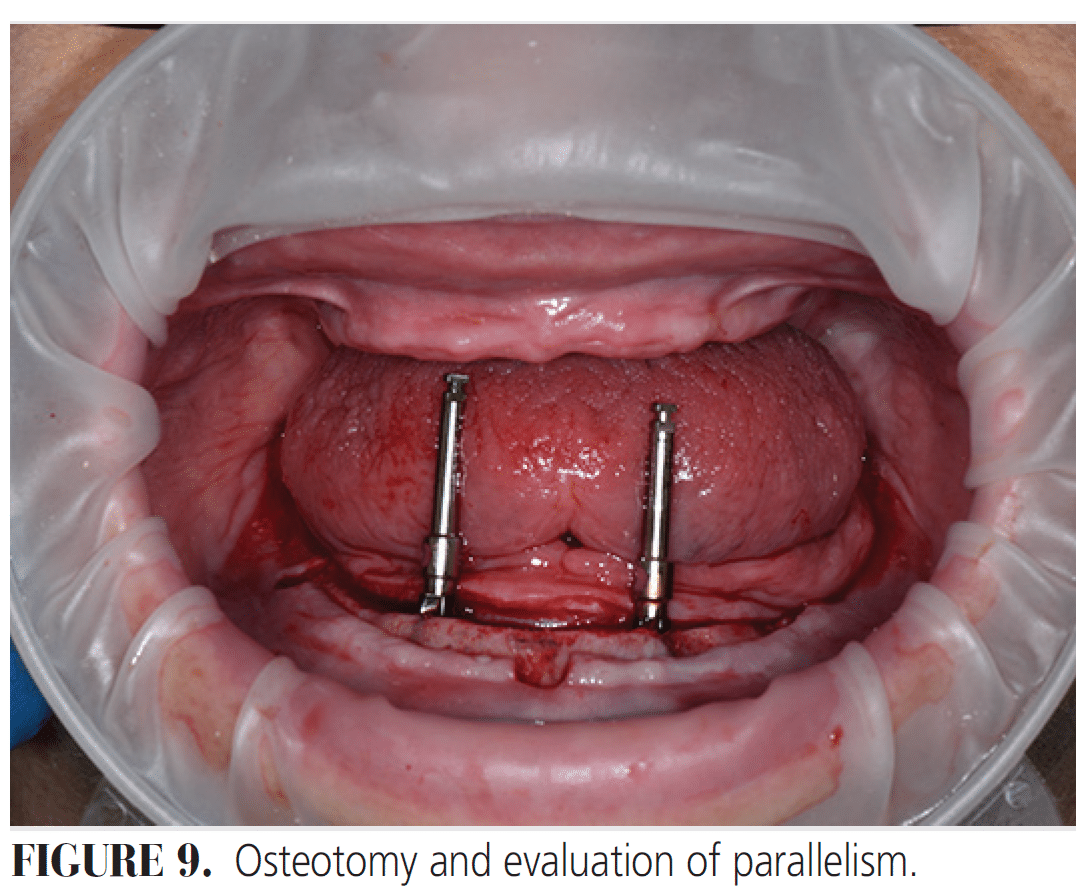
It is best to use the reference point of the implant platform to the incisal edge for restorative space measurements. This approach also allows for predictability in measurement to create a streamlined flow of information from the treatment planning (Figures 3 through 5, page 12-13) all the way to the surgical treatment. This creates simple communication from the restorative clinician to the surgical clinician so the surgical clinician can easily see where to complete the alveoplasty by measuring from incisal edge down and completing alveoplasty to that point (Figures 6 through 8), followed by implant placement (Figures 9 through 11).
CONCLUSION
Overdenture restorative space seems to create a bit of confusion among clinicians because multiple sources cite different values. This paper dissected available literature on overdenture restorative space in order to address the confusion. The primary reason for the discrepancy in values is the difference in the reference points used by individual authors. Some authors measure from incisal/occlusal edge to implant platform while others measure from the top of the acrylic to the implant platform if denture teeth are placed buccal/labial to the ridge.
The secondary reason is the variety of abutment and bar designs available with different restorative space requirements. This article presents findings to minimize the confusion and recommend guidelines on the appropriate minimum restorative space for splinted and unsplinted overdentures. This paper also acts as a guide to restorative and surgical clinicians about which reference points to use to create predictability from the surgical planning to the surgical treatment, leading to successful restorative outcomes for patients needing overdenture treatment.
References
- Raghoebar GM, Meijer HJA, Hof MV, Stegenga B, Vissink A. A randomized prospective clinical trial on the effectiveness of three treatment modalities for patients with lower denture problems: a 10 year follow-up study on patient satisfaction. InJ J Oral Maxillofac Surg. 2003;32:498-503.
- Ahuja S, Cagna D R. Defining available restorative space for implant overdentures. J Prosthet Dent. 2010;104:133-136.
- Chaimattayompol N, Arbree Nancy S. Assessing the space limitation inside a complete denture for implant attachments. J Prosthet Dent. 2003;89:82-85.
- Misch CE. Contemporary Implant Dentistry. 3rd ed. St. Louis: Mosby; 2007:297-298.
- Phillips, Wong KM. Space requirements for implant-retained bar-and-clip overdentures. Compendium of Continuing Education in Dentistry. 2001;22(6):516-518.
- Bidra AS. Consequences of insufficient treatment planning for flapless implant surgery for a mandibular overdenture: a clinical report. J Prosthet Dent. 2011;105:286-291.
- Lee CK, Agar JR. Surgical and prosthetic planning for a two-implant-retained mandibular overdenture: a clinical report. J Prosthet Dent. 2006;95:102-105.
From Decisions in Dentistry. March/April 2025;11(2):9-17.
