
 EDWARDOLIVE/ISTOCK/GETTY IMAGES PLUS
EDWARDOLIVE/ISTOCK/GETTY IMAGES PLUS
Provisional Removable Prostheses Fabricated From A Digital Impression
This case report presents a patient for whom interim removable partial dentures replacing maxillary and mandibular anterior teeth were fabricated based on digital intraoral imaging.
Technological advances, such as computer aided design/computer aided manufacturing (CAD/CAM) and digital intraoral imaging, are changing nearly all aspects of restorative dentistry. In regard to crown and bridge fabrication, studies have now reported that digital impressions are equal to — or more accurate than — conventional impressions made with elastomeric materials.1–3 Moreover, the master models fabricated with sequential layering of a polymer resin, called stereolithography (SLA) or three-dimensional (3D) printing, were verified to be as accurate as stone models fabricated from conventional impressions.4,5
Intraoral scanners and CAD/CAM technology have been widely used for fabricating fixed dental prostheses, but much less for fabricating removable partial prostheses,6 as intraoral scanning poses challenges in capturing the mobile soft tissue portion.7,8 A few papers reported a technique for using digital impressions to fabricate partial removable prostheses for Kennedy Class III patients,9,10 or to fabricate complete dentures.6,11
While making impressions is the first step to fabricate an intraoral appliance, some patients who have teeth exhibiting Class 3 mobility express concerns about the loss of teeth from impressions made using traditional elastomeric materials. As intraoral digital imaging allows operators to make the impression without applying elastomer around teeth, the impression can be obtained in a manner that avoids the unintentional extraction of periodontally compromised anterior teeth. This clinical report presents a patient in whom interim removable partial dentures replacing maxillary and mandibular anterior teeth were fabricated based on digital intraoral imaging.


CASE REPORT
A 63-year-old female presented to the general practice clinic at the University of Maryland School of Dentistry in Baltimore complaining that her “front teeth were very loose.” She had previously been diagnosed with hypertension, hypothyroidism and rheumatoid arthritis. The patient was taking lisinopril for hypertension, levothyroxine for hypothyroidism, and hydroxychloroquine for rheumatoid arthritis. Her medical history and medications did not pose contraindications for dental procedures. She presented with multiple missing teeth, severe periodontitis, and Class 3 mobility in multiple teeth.




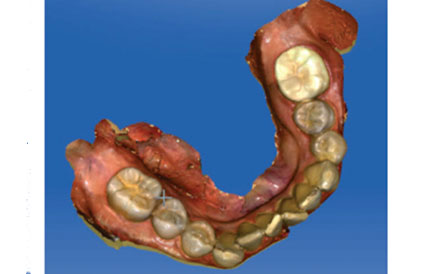
The patient’s missing teeth included the maxillary right second molar, maxillary left canine, maxillary left first and second molars, and the mandibular right and left second molars (Figure 1 and Figure 2). The two maxillary lateral incisors, as well as the two central mandibular incisors, exhibited Class 3 mobility due to severe periodontal bone loss (Figure 3 through Figure 6). Labial displacement and fremitus were noted on the two maxillary lateral incisors in maximum intercuspal position — defined as the position of the occlusal relationship in which the teeth of both arches are mostly interposed, independent of condylar position12 (Figure 7). Pathologic tooth migration was also observed for the two maxillary lateral incisors due to the patient’s severe periodontitis and secondary occlusal trauma (Figure 1 and Figure 7).13
The prognosis for the two maxillary lateral incisors, as well as the two mandibular central incisors, was deemed hopeless.14 Therefore, extraction of these teeth was recommended. As the treatment plan called for several anterior teeth to be extracted, interim partial removable dentures were offered. The patient expressed concerns, however, about losing teeth from making alginate impressions to fabricate the interim partial prostheses. A digital impression was suggested as an alternative technique.

A full-arch digital impression of the maxilla and mandible was made with an intraoral scanner (Figures 8 and Figure 9). Special attention was paid to capturing the palate (Figure 8). A digital buccal interocclusal record was made to articulate the maxilla and mandible (Figure 10). The digital impressions were then sent electronically to an outside laboratory to fabricate 3D-printed resin casts. The clinical team requested unaltered resin master casts in order to estimate the dimension of residual ridge after extraction of the teeth.
After the resin master casts were received from the laboratory, the two maxillary lateral incisors and mandibular central incisors were carefully removed from the resin master casts utilizing an acrylic bur. A thin layer of petroleum ointment was applied to the casts. Next, the interim maxillary and mandibular partial prostheses were fabricated at the in-school laboratory utilizing pink acrylic resin and denture teeth (Figures 11 through 13).


At the next appointment, the patient presented for the extractions (Figure 14). The interim partial dentures were delivered immediately after the two maxillary lateral and two mandibular central incisors were extracted (Figure 15). The intaglio surfaces were adjusted and polished, and the clasps were adjusted until the interim appliances were seated passively. Enameloplasty of the mandibular right canine was performed as the maxillary right lateral incisor was positioned palatially. This was done to close the space between the maxillary right central and lateral incisors. Enameloplasty on the maxillary right central incisor was also performed to correct the discrepancy of the incisal edges level of the two maxillary central incisors (Figure 14 and Figure 15).
The occlusion was checked to ensure no alterations were made to the patient’s interocclusal relationship in maximum intercuspal position. After the intaglio surfaces and clasps were adjusted at the delivery, the fitting of the interim removable prostheses was deemed clinically acceptable. Adjustment for the interim dentures was performed one time after delivery of the interim prostheses.

DISCUSSION
Using intraoral scanning to obtain edentulous area digital impressions poses some limitations. Because the intraoral scanner stitches narrow areas, it is difficult to scan the distally extended flat and broad edentulous area, and a functional impression is not possible with an intraoral scanner, as the technique is purely image-based.7
That noted, the use of a digital workflow in fabricating removable partial dentures offers potential benefits. Digital scanning captures the soft tissues located in edentulous areas in a passive state.9 Patients who have a tendency to gag during conventional impression procedures, as well as those with special needs or dental anxiety, should tolerate the intraoral scanning process better than having a conventional impression made with elastomeric materials. The digital impression technique worked well in the Kennedy Class III case presented here, as the need to capture border-molded extensions of the soft tissue was not critical with this patient.10
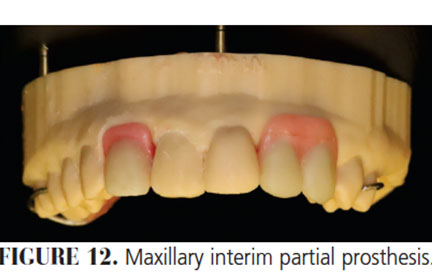

A nonadhesive agent, such as petroleum ointment, must be applied when resin-based removable prostheses are fabricated on the resin casts made from SLA. Even though an autopolymerizing polymethyl methacrylate denture base material was used, the interim dentures were still placed in a hot water bath after the initial polymerization in order to improve the degree of resin cure. The patient used the maxillary interim removable prostheses for eight months until a maxillary cast partial prosthesis was delivered to replace the maxillary right and left lateral incisors, maxillary left canine, and the maxillary left first molar. As the patient was satisfied with the mandibular interim prosthesis replacing two mandibular incisors and with the first molar occlusion (Figure 11 and Figure 13), she decided not to make a mandibular cast partial prosthesis.


SUMMARY
This clinical report describes how digital intraoral impressions can be used to fabricate interim partial prostheses and avoid the unintended extraction of hopeless teeth upon removal of a conventional elastomeric impression.
KEY TAKEAWAYS
- In regard to crown and bridge fabrication, studies have reported that digital impressions are equal to — or more accurate than — conventional impressions made with elastomeric materials.1–3
- Intraoral scanners have been widely used for fabricating fixed dental prostheses, but much less for fabricating removable partial prostheses,6 as intraoral scanning poses challenges in capturing the mobile soft tissue portion.7,8
- A few papers reported a technique for using digital impressions to fabricate partial removable prostheses for Kennedy Class III patients,9,10 or to fabricate complete dentures.6,11 This case report describes the clinical application of this technique.
- Patients who have teeth exhibiting Class 3 mobility may express concerns about the loss of teeth from impressions made using traditional elastomeric materials.
- As intraoral digital imaging allows operators to make the impression without applying elastomer around teeth, the impression can be obtained in a manner that avoids the unintentional extraction of periodontally compromised teeth.
REFERENCES
- Henkel GL. A comparison of fixed prostheses generated from conventional vs digitally scanned dental impressions. Compend Contin Educ Dent. 2007;28:422–424,426–428,430–431.
- Syrek A, Reich G, Ranftl D, Klein C, Cerny B, Brodesser J. Clinical evaluation of all-ceramic crowns fabricated from intraoral digital impressions based on the principle of active wavefront samplingJ J Dent. 2010;38:553–559.
- Ender A, Mehl A. Full arch scans: conventional versus digital impressions — an in-vitro study. Int J Comput Dent. 2011;14:11–21.
- Santoro M, Galkin S, Teredesai M, Nicolay OF, Cangialosi TJ. Comparison of measurements made on digital and plaster models. Am J Orthod Dentofac Orthop. 2003;124:101–105.
- Kim SY, Kim MJ, Han JS, Yeo IS, Lim YJ, Kwon HB. Accuracy of dies captured by an intraoral digital impression system using parallel confocal imaging. Int J Prosthodont. 2013;26:161–163.
- Kim JE, Kim NH, Shim JS. Fabrication of a complete, removable dental prosthesis from a digital intraoral impression for a patient with an excessively tight reconstructed lip after oral cancer treatment: a clinical report. J Prosthet Dent. 2017;117:205–208.
- Lee JW, Park JM, Park EJ, Heo SJ, Koak JY, Kim SK. Accuracy of a digital removable partial denture fabricated by casting a rapid prototyped pattern: a clinical study. J Prosthet Dent. 2017;118:468–474.
- Patzelt S, Vonau S, Stampf S, Att W. Assessing the feasibility and accuracy of digitizing edentulous jaws. J Am Dent Assoc. 2013;144:914–920.
- Kattadiyil MT, Mursic Z, AlRumaih H, Goodacre CJ. Intraoral scanning of hard and soft tissues for partial removable dental prosthesis fabrication. J Prosthet Dent. 2014;112:444–448.
- Mansour M, Sanchez E, Machado C. The use of digital impressions to fabricate tooth-supported partial removable dental prostheses: a clinical report. J Prosthodont. 2016;25:495–497.
- Fang JH, An X, Jeong SM, Choi BH. Development of complete dentures based on digital intraoral impressions — case report. J Prosthodont Res. 2018;62:116–120.
- Garrido García VC, García Cartagena A, González Sequeros O. Evaluation of occlusal contacts in maximum intercuspation using the T-Scan system. J Oral Rehabil. 1997;24:899–903.
- Oh SL. An interdisciplinary treatment to manage pathologic tooth migration: a clinical report. J Prosthet Dent. 2011;106:153–158.
- McGuire MK, Nunn ME. Prognosis versus actual outcome. II. The effectiveness of clinical parameters in developing an accurate prognosis. J Periodontol. 1996;67:658–665.
The authors have no commercial conflicts of interest to disclose.
From Decisions in Dentistry. January 2020;6(1):22–24.
