

Pathology of Gingival Cancer
While gingival cancer can be difficult to detect, survival rates depend on early treatment.
While gingival cancers can be difficult to detect, survival rates depend on early treatment
A collaborative relationship between all members of the oral health care team is fundamental to the provision of high-quality dental care — and one of the most crucial collaborative efforts is performing a thorough head and neck exam. In many practices, dentists rely on dental hygienists to perform a systematic examination of the oral cavity and the entire head and neck complex, and they are often the first clinicians to note any variations from normal. Yet even with this systematic approach, some gingival cancers may be challenging to identify when inflammatory components are involved and their initial presentation appears as a dental abscess, trauma or periodontal disease.1–3
Gingival cancers are rare and their initial presentation may be missed due to their location. Unfortunately, a delay in early intervention may adversely affect survival rates. This article outlines a gingival cancer that initially presented with features of periodontal disease and, thus, hindered a definitive diagnosis. Consequently, treatment was delayed.
In this case study, an 85-year-old woman was seen for comprehensive care in a dental residency clinic. The patient was hypertensive and reported occasional alcohol consumption and no tobacco use. After an initial examination, she was diagnosed with generalized moderate periodontitis and localized severe periodontitis in the mandibular left quadrant. Pocket depths ranged from 6 mm for teeth #20 and #21 to 9 mm for #18 and#19. Scaling and root planing was performed, along with extractions of #18 and #19 due to their severe attachment loss and mobility.
The treatment plan included a mandibular removable partial denture to replace #18 and #19. The patient returned within two weeks for study models. The healing of the extractions sites was favorable. A final impression for the mandibular removable partial denture was obtained a week later. The patient returned for a six-week reevaluation of the scaling and root planing therapy. Tissue response was favorable for the maxillary arch and mandibular right quadrant, but there was moderate plaque accumulation and severe inflammation of the gingival tissue in the mandibular left quadrant on #20 and slightly distal on the edentulous segment. Pocket depths ranged from 3 mm to 4 mm.
As the nature of the lesion aroused suspicion, the clinic’s oral surgeon was summoned to evaluate the site. The oral surgeon thought the inflammation was caused by the accumulation of plaque and residual subgingival calculus, and the patient admitted she had avoided brushing the area after the extractions of #18 and #19. The area was scaled again, and the patient was reinstructed on proper oral hygiene care. A mandibular partial denture was inserted at this visit, and the patient received instructions on its care.
FOLLOW-UP FINDINGS
The patient was scheduled for a two-week follow-up of the removable partial denture and evaluation of the mandibular left quadrant. At the second visit, the tissue in the mandibular left quadrant was inflamed and erythematous, and the texture had changed with noticeable white specks and a pebbly appearance distal to #20. The patient complained of moderate pain, which was due to irritation and inflammation caused by the partial denture. The pressure spots were relieved on the partial denture. However, the severe erythema and dramatic change of the gingiva prompted a referral to an oral surgeon for a second opinion. The oral surgeon biopsied the lesion, and the pathology report noted verrucous carcinoma — a type of squamous cell carcinoma — as the definitive diagnosis.
Typically, a suspicious lesion is recommended for biopsy after it has been present for two weeks or longer. With this patient, in the two-week interval after the extractions and initial scaling and root planing, tissue response had been favorable. At the six-week reevaluation, however, the tissue revealed severe inflammation, moderate plaque and residual subgingival calculus, which led the oral surgeon to suspect periodontal disease — not gingival cancer. To compound the issue, the pressure spots from the removable partial denture contributed to the inflammation and misdiagnosis. The appearance of the lesion changed more dramatically in the following two weeks, at which point the referral for biopsy was made. This case reinforces the need to review oral pathology, particularly gingival cancer.
SQUAMOUS CELL CARCINOMA
More than 90% of oral cancers present as squamous cell carcinoma.4 Lesions range from a white plaque-like appearance to a red and white exophytic appearance that can develop anywhere in the oral cavity, but most frequently occurs on the tongue, tonsils, oropharynx and floor of the mouth.4 Examination of these specific areas may lead to entirely missing gingival lesions when an inflammatory component and initial impression of periodontal disease are present. Emphasis should be placed on evaluating gingival and inflammatory lesions more closely for the possibility of gingival cancers. The patient may be asymptomatic in the early stages. But with progression of the gingival cancer, symptoms may include a swelling or mass, pain, and mobility of teeth due to destruction of underlying bone.5 At late stages, the prognosis is poor.
Squamous cell carcinoma of the gingiva may be difficult to diagnose in its early stages when inflammatory components and bone loss are present.6 White lesions are usually recognized more readily. Figure 1 demonstrates a white plaque-like lesion on the facial of #9, which was caused by anaspirin burn. Figure 2 and Figure 3 demonstrate white plaque-like lesions with erythematous components on the facial and palatal gingival margins of #9, #10 and #11. When evaluating lesions with this clinical presentation, practitioners should ask a series of questions to aid in definitive diagnosis. For example, if trauma or a chemical burn is suspected, the following questions should be asked:
- Have you noticed the change in color of your gingiva in this area?
- If so, how long has this lesion been present?
- Does it hurt?
- Did you place aspirin in the area of discomfort?
Some patients erroneously think that direct topical application of a pain reliever will be more effective than taking it orally. This is precisely what the patient did in Figure 1. Most dental professionals would recommend the patient return in two weeks to reevaluate the area, and, in the absence of resolution, a referral for a biopsy would be indicated. This is the ideal scenario, but often not the case. Prime examples are illustrated in Figure 2 and Figure 3, where the lesion had been present for some time before a definitive diagnosis of squamous cell carcinoma of the gingiva was confirmed through biopsy. This lesion presented at an advanced stage of cancer that is now more challenging to treat.

COURTESY OF SOL SILVERMAN JR., MA, DDS
COURTESY OF DARREN COX, DDS, MBA

COURTESY OF DARREN COX, DDS, MBA
Figure 4 through Figure 6 demonstrate various forms of squamous cell carcinoma that may be initially mistaken for frictional keratosis or pyogenic granuloma. Any suspicious lesion or ulcerated tissue should be followed up with another evaluation within two weeks of presentation. If a lesion persists, and/or is nonhealing, a referral to an oral surgeon or oral pathologist is indicated. Thorough documentation regarding the color, location, size and texture of the lesion will make it easier to evaluate during subsequent visits.

COURTESY OF SOL SILVERMAN JR., MA, DDS

COURTESY OF SOL SILVERMAN JR., MA, DDS

COURTESY OF SOL SILVERMAN JR., MA, DDS
Taking a photograph of the initial lesion is recommended. If dental practitioners routinely take photos of oral lesions, a helpful library of images can be developed that may prove invaluable. If a biopsy is indicated, the picture can be forwarded to the oral pathologist to aid in the diagnosis. Asking questions is crucial and may trigger the patient’s memory, providing information helpful to arriving at a diagnosis.
ORAL VERRUCOUS HYPERPLASIA AND CARCINOMA
Oral verrucous hyperplasia presents as a white, plaque-like lesion. It is difficult to distinguish from oral verrucous carcinoma and tends to precede verrucous carcinoma.7 People who use smokeless tobacco and drink one or more alcoholic beverages per month are predisposed to verrucous hyperplasia.7 For this reason, these lesions should be closely evaluated and not dismissed as benign.

COURTESY OF DARREN COX, DDS, MBA
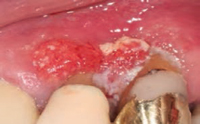
Oral verrucous carcinoma is a form of squamous cell carcinoma with a variable appearance and unknown etiology.7 It may present as a white, plaque-like lesion or a mixed white-red lesion with a pebbly, wart-like surface.7 Figure 7 illustrates a more advanced form of verrucous carcinoma. It occurs more frequently in the mandibular posterior alveolar ridge and retromolar region, but can also present in the buccal mucosa, palate, floor of the mouth and lip.7
The case study patient had a partial denture and the site of the verrucous carcinoma occurred on the gingiva distal to #20 and on the alveolar ridge. In partially edentulous patients, areas of concern include the gingival tissue of the abutment teeth retaining the removable appliance and the alveolar ridge area. Patients with removable partial dentures or full dentures should be scrutinized closely for these types of lesions. While it is true that some of the lesions associated with removable appliances are due to pressure spots or ill-fitting dentures, various precancerous or cancerous lesions may present similarly.
CONCLUSION
The gingival cancer in this case study initially presented as periodontal disease with local etiologic factors of inflammation, bone loss and subgingival calculus. No risk factors for gingival cancer were evident. An accurate diagnosis was delayed, as completion of periodontal therapy and reevaluation of treatment took two to three months. This case illustrates the need to be highly diligent when evaluating gingival lesions. If the lesion is still present after two weeks, the patient should be referred to an oral surgeon or oral pathologist for biopsy. Early detection of cancer is crucial to an increased survival rate. It behooves all oral health professionals to promptly refer when gingival lesions are unresponsive to the usual treatment modalities.
key takeaways
- One of the most crucial collaborative efforts in daily practice is performing a thorough head and neck exam — yet even with this systematic approach, some gingival cancers may be challenging to identify when inflammatory components are involved.
- More than 90% of oral cancers present as squamous cell carcinoma.4 Lesions range from a white plaque-like appearance to a red and white exophytic appearance that can develop anywhere in the oral cavity, but most frequently occurs on the tongue, tonsils, oropharynx and floor of the mouth.4
- The patient may be asymptomatic in the early stages, but, as gingival cancer symptoms progress, they may include a mass or swelling, pain, and tooth mobility due to destruction of underlying bone.5
- Squamous cell carcinoma of the gingiva may be difficult to diagnose in its early stages when inflammatory components and bone loss are present.6
- Any suspicious lesion or ulcerated tissue should be followed up with another evaluation within two weeks of presentation. If a lesion persists and/or is nonhealing, a referral to an oral surgeon or oral pathologist is indicated.
- Thorough documentation regarding the color, location, size and texture of the lesion will make it easier to evaluate during subsequent visits. Taking a photograph of the initial lesion is recommended.
References
- Seoane J, Varela-Centelles PI, Walsh TF, Lopez-Cedrun JL, Vazquez I. Gingival squamous cell carcinoma: diagnostic delay or rapid invasion? J Periodontol. 2006;77:122–133.
- Lee JJ, Cheng SJ, Lin SK, Chiang CP, Yu CH, Kok SH. Gingival squamous cell carcinoma mimicking a dentoalveolar abscess: report of a case. J Endod. 2007:33:177–180.
- Cox D. Introduction to a Diagnostic Approach to Oral and Maxillofacial Pathology: A Programmed Text [iBook]. 2012. Based on: Rovin S, Sabes WR, Howell RM. The Programmed Textbook of Oral Pathology. 2nd ed. Lexington, Kentucky: OP Enterprises; 1973.
- Oral Cancer Foundation. Oral Cancer Facts. Available at: http://www.oralcancerfoundation.org/facts/. Accessed November 9, 2015.
- Daneshi M, Beylin S, Zemnick C, Emde K. Misdiagnosis of gingival squamous cell carcinoma presenting as a periodontal lesion of the anterior palate. Columbia Dental Review. 2009/2010;14(6):12–15.
- Fitzpatrick SG, Neuman AN, Cohen DM, Bhattacharyya I. The clinical and histologic presentation of gingival squamous cell carcinoma: a study of 519 cases. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114:509–515.
- Alkan A, Bulut E, Gunhan O, Ozden B. Oral verrucous carcinoma: a study of 12 cases. Eur J Dent. 2010;4:202–207.
