
 PRUDENCIOALVAREZ/ISTOCK/GETTY IMAGES PLUS
PRUDENCIOALVAREZ/ISTOCK/GETTY IMAGES PLUS
Overview of X-Linked Hypophosphatemia For Oral Health Professionals
As part of a comprehensive care team, dental providers play an essential role in preventing and treating the oral health complications of X-linked hypophosphatemia.
PURCHASE COURSE
This course was published in the February 2021 issue and expires February 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the February 2021 issue and expires February 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Explain X-linked hypophosphatemia (XLH), its prevalence and typical onset.
- Discuss the clinical presentation of XLH, and its potential oral health consequences.
- Describe dental treatment considerations when caring for this patient population.
X-linked hypophosphatemia (XLH) is a genetic disorder caused by a mutation in the PHEX gene located on the X chromosome.1 Affecting approximately one in 20,000 births, it is the most common form of hereditary rickets.2 Symptoms range from hypophosphatemia without bone-related manifestations to severe symptoms that may impact activities. Most cases occur early in childhood, while some cases may affect adults. Clinically, XLH is often misdiagnosed or missed altogether.1 In addition to systemic findings, XLH poses risk for oral complications.3–5 All healthcare professionals, including oral health providers, should be aware of its multifaceted characteristics. This paper will describe the nature of this disease and the role of dental professionals in the prevention and treatment of oral complications.
Phosphate is one of the metabolic factors used for cellular energy metabolism and membrane stability. It is the main component of hydroxyapatite in bone. Serum phosphate levels are maintained by hormonal regulation, including calcitriol, parathyroid hormone and fibroblast growth factor 23 (FGF23) through intestinal absorption, renal reabsorption and bone resorption; FGF23 has its principal action in the kidneys, preventing undue elevation of serum phosphate levels.6 In XLH, the PHEX gene, a member of the M13 family of neutral endopeptidases, activates or degrades peptides, and is expressed in bones and teeth. This gene mutates through unclear mechanisms and causes FGF23 excess.1 Elevated concentrations of circulating FGF23 contribute to renal phosphate wasting and hypophosphatemia; it also prevents production of circulating vitamin D [1,25(OH)2D].7–9 Chronic hypophosphatatemia leads to rickets through a lack of endothelial ossification and abnormal bone mineralization.10,11 Further, insufficient levels of inorganic phosphate affect the function of mature osteoblasts because the formation of mature bone involves the precipitation of hydroxyapatite crystals. The mutated PHEX gene in bone could explain why oral phosphate supplements have not always been successful, even when started early.12
Because the PHEX gene is located on the X chromosome, having only one mutated copy of the gene is sufficient to cause the disorder in males and females. A female with XLH has a 50% chance of passing this condition to each of her children, while a male with XLH will pass this disorder to all of his daughters, but none of his sons.13,14 Cases sometimes occur in a family with no history of this condition, likely due to a new mutation in the PHEX gene.13
SIGNS AND SYMPTOMS
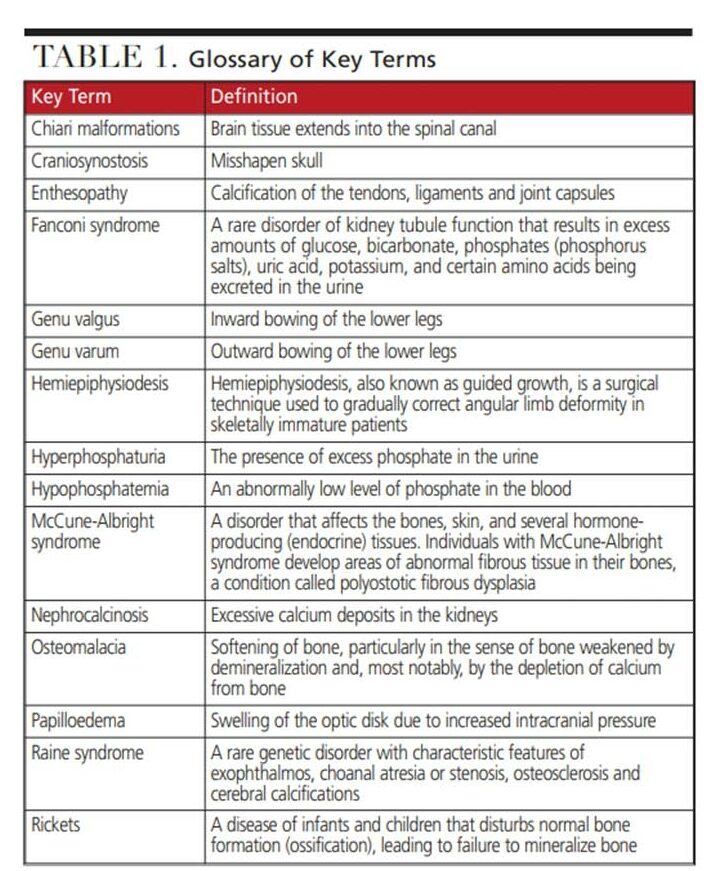
Clinically, symptoms of XLH vary, but the typical presentation becomes apparent within the first 18 months to two years of life, with the onset of weight-bearing activity.13,14 Early signs and symptoms include short stature, slow growth rate, and limb deformity.13–15 Lower extremity bowing may be represented as genu varum or genu valgus (see Table 1 for key terms). Torsion and rotation of the lower extremity may also occur.14 These findings result in a waddling gait. Adults may experience significant joint pain and mobility issues resulting from enthesopathy.13,14 Spinal cord compression, arthritis, and fusion of the sacroiliac joints can lead to back pain and decreased mobility. Pathologic fractures and pseudofractures may occur in adults.6,16 Other skeletal abnormalities include frontal bossing, craniosynostosis and Chiari malformations, and widened wrists and ankles.6,14 Characteristic signs also include osteomalacia and rickets bone disease that does not improve with traditional vitamin D therapy.
Individuals with XLH are susceptible to dental abnormalities. Spontaneous dental abscesses, enamel and dentin defects, oral pain, delayed eruption, enlarged pulp chambers, and taurodontism of permanent molars are all features of this condition.5,13,14,17 Additional signs are sensorineural hearing loss, secondary and tertiary hyperparathyroidism, and cardiovascular and metabolic disorders.14,16 Individuals with XLH can be medically complex. In a study of 59 adults with XLH, Chesher et al15 reported 38 patients presented with nephrocalcinosis; hearing impairment was documented in eight patients; and five patients had neoplastic disease (including melanoma of the parotid gland, breast carcinoma, colorectal cancer, Hodgkins lymphoma, phaeochromocytoma and pituitary macroprolactinoma). In addition, one patient had an asymptomatic papilloedema of the eye accompanied by type 1 Chiari malformation, and, another had stable chronic renal failure with secondary hypertension and hyperparathyroidism.
DIAGNOSIS
The diagnosis of XLH is based on clinical, laboratory or biochemical analysis, radiographic findings and family history. In addition to the clinical features noted above, laboratory/biochemical findings include elevated levels of FGF23 associated with hypophosphatemia and hyperphosphaturia. Calcium and parathyroid hormone levels will be normal, while serum alkaline phosphatase may be normal or increased. Plasma calcidiol concentration will be normal, while serum levels of calcitriol may be normal or low. The phosphate excretion rate may be elevated. Radiographic evidence of XLH in children demonstrates fraying and cupping of metaphyseal regions; in comparison, pseudofractures and enthesopathies are found in adults. Iliac bone biopsies reveal evidence of osteomalacia and hypomineralized periosteocytic lesions.18
Radiographic presentations of XLH may not be pathognomonic for hypophosphatemic rickets; however, a study by Lempicki et al2 used magnetic resonance imaging (MRI) to identify markers of hypophosphatemic rickets activity. In this study, MRI examination of the knees of patients with hypophosphatemic rickets revealed maximum physical widening and transverse degree of widening that correlated with alkaline phosphatase levels.
After completing the examination, molecular genetic testing is used to confirm a diagnosis of XLH. The rachitic skeletal changes of nutritional and hereditary forms of rickets are difficult to distinguish. The differential diagnosis of XLH includes autosomal dominant hypophosphatemic rickets, autosomal recessive hypophosphatemic rickets, tumor-induced osteomalacia, McCune-Albright syndrome, fibrous dysplasia of bone, Fanconi syndrome, hereditary hypophosphatemic rickets with hypercalciuria, vitamin D-dependent rickets (types I and II), vitamin D-deficient rickets, pseudohypoparathyroidism, Raine syndrome, and hypophosphatemia rickets with hyperparathyroidism.12,14,18
TREATMENT AND PROGNOSIS
Treatment focuses on healing rickets, improving leg deformities, maximizing growth potential, alleviating pain, improving muscle function, and managing complications that occur in adulthood. For children, treatment typically begins at the time of diagnosis and continues until growth is completed. For adults, the main goal of treatment is to reduce pain.
Prior to 2018, conventional treatment was daily oral phosphate supplements and vitamin D therapy. Doses varied, depending on disease severity. In 2018, the U.S. Food and Drug Administration approved the use of burosumab, a recombinant human monoclonal IgG1 antibody that targets FGF236,12 and acts to normalize phosphorus levels, improve bone mineralization, manage the leg deformity associated with rickets in children, and help heal fractures in adults.19–25 Other adjuncts include the use of growth hormone in children, MAPK inhibitors, cinacalcet and calcitonin. Limited studies have been conducted with these treatment alternatives, and, due to the lack of available evidence, none of these options can be recommended for routine use in children.6
Surgical care is a consideration for children whose diagnosis was delayed, or for whom initial treatment proved ineffective. Some limb deformities require orthopedic surgery, including osteotomy and fixation, or growth modulation with hemiepiphysiodesis.26,27 For patients who present with craniosynostosis due to the premature fusion of the skull sutures or Chiari 1 malformations, involving a pediatric neurosurgical team is recommended.28,29 Lastly, for patients who progress to tertiary hyperparathyroidism, parathyroidectomy may be indicated.30
GENETIC COUNSELING
Because XLH is an inherited X-linked dominant disorder, genetic testing and counseling are recommended for individuals and family members to clarify genetic status and facilitate informed decisions about genetic risk assessment. The father of a male with XLH will not have the disorder and does not require further testing. If a male is the only family member with XLH, the mother may be heterozygous for the pathogenic variant or the affected male has a de novo pathogenic variant. In this case, the mother should be tested. In a family with more than one affected individual, the mother of an affected male is an obligate heterozygote and may have clinical findings.14
A female proband may have inherited the PHEX pathogenic variant from her mother or father. Another possibility is that the pathogenic variant may be de novo. Therefore, genetic testing is recommended for the parents of a female proband with an apparent de novo pathogenic variant.14 The optimal time for determining genetic risk for XLH is before pregnancy.
ORAL HEALTH CONSIDERATIONS
To provide person-centered care, it is important to understand XLH from an oral health perspective. Research has examined the mineralization effects of XLH on the structure of teeth; case studies have demonstrated dental problems associated with XLH; and a qualitative study revealed the impact XLH may have on daily life. Several studies have provided information on the link between XLH and dentoalveolar defects. Zhang et al3 used Hyp mice, a PHEX mutant, to examine effects of XLH on dental formation and function. Their findings showed that PHEX mRNA was expressed by odontoblasts, osteocytes and cementocytes, enamel volume was reduced, and acellular cementum was thin and showed periodontal ligament detachment. Histologically, dentin defects presented as wide predentin, thin dentin, and extensive interglobular dentin represented as reduced dentin volume and density on micro-computed tomography. Coyac et al31 confirmed the impaired mineral quality changes noted by Zhang et al.3 In their study of dentin using electron microscopy, Coyac and colleagues31 noted major disorganization of the peri- and intertubular structure of the dentin, as well as impaired mineral quality and matrix changes in XLH dentin representing a high level of sensitivity to serum phosphate levels.
In another paper, Coyac et al4 studied XLH dental pulp cell cultures revealing abnormal mineralization — most likely due to an increase in FGF23, and not the PHEX mutation alone. The authors recommended that treatments for XLH should target both local and systemic symptoms. Further, Duplan et al32 examined the periodontal status of adults with XLH and the extent of treatment for their condition. They noted the frequency and severity of patients’ periodontitis varied according to the treatment provided for their hypophosphatemia. Children who received early therapy with vitamin D and phosphate supplementation tended to have less periodontal attachment loss than those who had incomplete treatment or late treatment. This study also examined extracted teeth from patients who had late or incomplete treatment for XLH. The extracted teeth showed acellular cementum hypoplasia. The authors concluded that XLH affects bone, dentin formation and cementum, resulting in periodontal attachment loss.32
Case studies provide further understanding of the oral health problems associated with XLH. Goodman et al5 described 17 children with an established diagnosis of hypophosphatemic vitamin D rickets, noting that abscesses were the presenting feature in 11 cases. Attrition and exposure of the defective dentin was considered the etiology for the abscesses of the primary teeth; however, abscesses of the permanent teeth were unexplained. Enamel defects were found in six patients, and three of these cases occurred in primary dentition. Further, taurodontism was noted on the permanent first molars of males who were severely affected with XLH. Chesher et al15 reported case note review documents of the clinical features of 59 adults with XLH that indicated 63% had at least one form of oral disease, including caries, periodontal disease, missing teeth and failing restorations. More than 40% of the subjects had a history of de novo abscesses, and 49% required at least one extraction. The findings did not appear to be related to age or treatment for XLH. Lee et al33 detailed two cases of patients with XLH, each of whom presented with multiple abscesses over the course of care.
Finally, Lo et al34 conducted a qualitative study of 30 adults with XLH to identify their health-related quality of life, as little information exists on this aspect of the disease. Most XLH individuals reported pain, stiffness, fatigue and mobility as the most common symptoms affecting their lives; however, oral health issues were noted by three-quarters of the sample. While the majority reported negative social experiences (including bullying) resulting in low self-esteem, frustration and depression, others noted having developed mental resilience due to their health condition. A concern for patients was the worry about the future given that XLH is a lifelong, progressive condition.
Given that individuals with XLH have a tendency toward tooth mineralization defects, abscesses and periodontal disease, it is essential they receive regular dental examinations. With the goal of individualized care, oral health professionals should coordinate with the patient’s medical team to ensure comprehensive care is provided. In addition, since XLH may be missed or misdiagnosed, attention to detail during clinical and radiographic assessment is important. Recurring abscesses would be a key identifier of this particular disorder.
Recognizing health-related quality of life issues will help provide assurance during appointments. For example, these patients may benefit from pillows to support their legs and back, or may find they need to change positions in the dental chair if long appointments are necessary. Additionally, patients may require a break during procedures to address stiffness, pain and fatigue.34
Assessing caries risk is an important preventive strategy for this population. Enamel and dentin defects should be evaluated, and fluoride and restorative procedures considered (as indicated) as part of a comprehensive plan to help patients achieve optimum oral health. Likewise, a periodontal program should be considered to mitigate disease occurrence. As case needs dictate, a multidisciplinary team approach between dental hygienists, restorative dentists, orthodontists, endodontists, periodontists and implantologists will help prevent and manage serious dental problems.
Although rare, the genetic disorder XLH affects multiple organs and systems, including oral health. Early diagnosis, regular comprehensive examinations, and utilizing a multidisciplinary team approach will help improve the quality of life of individuals who experience this challenging condition.
REFERENCES
- Carpenter TO, Imel EA, Holm IA, Jan de Beur SM, Insogna KL. A clinician’s guide to X-linked hypophosphatemia. J Bone Miner Res. 2011;26:1381–1388.
- Lempicki M, Rothenbuhler A, Merzoug V, et al. Magnetic resonance imaging features as surrogate markers of X-linked hypophosphatemic rickets activity. Horm Res Paediatr. 2017;87:244–253.
- Zhang H, Chavez MB, Kolli TN, et al. Dentoalveolar defects in the mouse model of X-linked hypophosphatemia. J Dent Res. 2020;99:419–428.
- Coyac BR, Hoac B, Chafey P, et al. Defective mineralization in X-linked hypophosphatemia dental pulp cell cultures. J Dent Res. 2018;97:184–191.
- Goodman JR, Gelbier MJ, Bennett JH, Winter GB. Dental problems associated with hypophosphatemia vitamin D resistant rickets. Int J Paediatr Dent. 1998;8:19–28.
- Saraff V, Nadar R, Högler W. New developments in the treatment of X-linked hypophosphataemia: Implications for clinical management. Pediatr Drugs. 2020;22:113–121.
- Yamazaki Y, Okazaki R, Shibata M, et al. Increased circulatory level of biologically active full-length FGF-23 in patients with hypophosphatemic rickets/osteomalacia. J Clin Endocrinol Metab. 2002;87:4957–4960.
- Santos F, Fuenta R, Mejia N, Mantecon L, Gil-Peña H, Ordoñez FA. Hypophosphatemia and growth. Pediatr Nephrol. 2012;28:595–603.
- Quarles LD. FGF23, PHEX, and MEPE regulation of phosphate homeostasis and skeletal mineralization. Am J Physiol Endocrinol Metab. 2003;285:E1–E9.
- Tiosano D, Hochberg Z. Hypophosphatemia: The common denominator in rickets. J Bone Miner Metab. 2009;27:392–401.
- Penido MG, Alon US. Phosphate homeostasis and its role in bone health. Pediatr Neprhol. 2012;27:2039–2048.
- Chan JC. Hypophosphatemic rickets. Available at: https://emedicine.medscape.com./article/922305-print. Accessed January 7, 2021.
- Genetic and Rare Diseases Information Center. X-linked hypophosphatemia. Available at: https://raredisease.info.nih.gov/diseases/12943/x-linked-hypophosphatemia. Accessed January 7, 2021.
- Ruppe MD. X-linked hypophosphatemia. Available at: https://www.ncbi.nlm.nih.gov/books/NBK83985/. Accessed January 7, 2021.
- Chesher D, Oddy M, Darbar U, et al. Outcome of adult patients with X-linked hypophosphatemia caused by PHEX gene mutations. J Inher Met Dis. 2018;41:865–876.
- Lecoq A-L, Chaumet-Riffaud P, Blanchard A, et al. Hyperparathyroidism in patients with X-linked hypophosphatemia. J Bone Miner Res. 2020;35:1263–1273.
- Connor J, Olear EA, Insogna KL, et al. Conventional therapy in adults with X-linked hypophosphatemia: Effects on enthesopathy and dental disease. J Clin Endocrinol Metab. 2015;100:3625–3632.
- Orphanet. X-linked hypophosphatemia. Available at: https://www.orpha.net/consor/cgi-bin/OC_Exp.php?Ing=En&Expert=89936. Accessed January 7, 2021.
- Brooks M. FDA clears first drug for rare inherited form of rickets. Available at: https://www.medscape.com/viewarticle/895322_print. Accessed January 7, 2021.
- U.S. Food and Drug Administration. FDA approves first therapy for rare inherited form of rickets, X-linked hypophosphatemia. Available at: https://www.fda.gov/news-events/press-announcements/fda-approves-first-therapy-rare-inherited-form-rickets-x-linked-hypophosphatemia. Accessed January 7, 2021.
- Carpenter TO, Whyte MP, Imel EA, et al. Burosumab therapy in children with X-linked hypophosphatemia. N Engl J Med. 2018;378:1987–1998.
- Whyte MP, Carpenter TO, Gottesman GS, et al. Efficacy and safety of burosumab in children aged 1–4 years with X-linked hypophosphatemia: a multicentre, open-label, phase 2 trial. Lancet Diabetes Endocrinol. 2019;7:189–199.
- Thacher TD, Pettifor JM, Tebben PJ, et al. Rickets severity predicts clinical outcomes in children with X-linked hypophosphatemia: Utility of the radiographic rickets severity score. Bone. 2019:122:76–81.
- Imel EA, Glorieux FH, Whyte MP, et al. Burosumab versus conventional therapy in children with X-linked hypophosphataemia: A randomized, active-controlled, open-label, phase 3 trial. Lancet. 2019;393:2416–2427.
- Insogna KL, Briot K, Imel EA, et al. A randomized, double-blind, placebo-controlled, phase 3 trial evaluating the efficacy of burosumab, an anti-FGF23 antibody, in adults with X-linked hypophosphatemia: week 24 primary analysis. J Bone Miner Res. 2018;33:1383–1393.
- Novais E, Stevens PM. Hypophosphatemic rickets: the role of hemiepiphysiodesis. J Pediatr Orthop. 2006;26:238–244.
- Kocaoglu M, Bilen FE, Sen C, Eralp L, Balci HI. Combined technique for the correction of lower-limb deformities resulting from metabolic bone disease. J Bone Joint Surg Br. 2011;93:52–56.
- Currarino G. Sagittal synostosis in X-linked hypophosphatemic rickets and related diseases. Pediatr Radiol. 2007;37:805–812.
- Vega RA, Opalak C, Harshbarger RJ, et al. Hypophosphatemic rickets and craniosynostosis: a multicenter case series. J Neurosurg Pediatr. 2016;17:694–700.
- Savio RM, Gosnell JE, Posen S, Reeve TS, Delbridge LW. Parathyroidectomy for tertiary hyperparathyroidism associated with X-linked dominant hypophosphatemic rickets. Arch Surg. 2004;139:218–222.
- Coyac BR, Falgayrac G, Penel G, et al. Impaired mineral quality in dentin in X-linked hypophosphatemia. Connect Tissue Res. 2018;59(suppl 1):91–96.
- Duplan MB, Coyac BR, Bardet C, et al. Phosphate and vitamin D prevent periodontitis in X-linked hypophosphatemia. J Dent Res. 2017;96:388–395.
- Lee BN, Jung HY, Chang HS, Hwang YC, Oh WM. Dental management of patients with X-linked hypophosphatemia. Restor Dent Endod. 2017;42:146–151.
- Lo SH, Lachmann R, Williams A, Piglowska N, Lloyd AJ. Exploring the burden of X-linked hypophosphatemia: a European multi-country qualitative study. Qual Life Res. 2020;29:1883–1893.
From Decisions in Dentistry. February 2021;7(2):40–43.

