

Optimal Management of Tooth Decay in Children
Implementing an evidence-based fluoride approach to treating this common chronic childhood disease is a prudent approach to improving patient outcomes.
PURCHASE COURSE
This course was published in the October/November 2025 issue and expires November 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the October/November 2025 issue and expires November 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 430
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
-
Identify the sources of fluoride available for use in the dental office and out-of-office settings.
-
Discuss how to create a child-centered fluoride strategy.
-
Explain ways to facilitate effective patient communication.
Introduction
Managing childhood caries is particularly complex and challenging. The disease itself is multifaceted, and when caries appears at an early age, it is further complicated by psychological and developmental factors that may impact the ability of oral health professionals to deliver effective care.
Considering the high prevalence, incidence, and burden that dental caries represents, every preventive measure and agent at our disposal should be considered in order to protect our patients — especially children and other vulnerable populations. Our goal as oral health professionals is to ensure patients remain healthy and smiling for a long time.
This article reviews key preventive measures for childhood caries, highlighting their benefits, roles in prevention, and how to apply them effectively to achieve the best outcomes for patients.
— Martin Pendola, PhD Scientific Affairs Manager Colgate Oral Pharmaceuticals, Inc.
Strategies for Addressing Childhood Caries
Tooth decay is the most common disease in children worldwide.1 Nearly one in two United States children are affected by tooth decay.2 Restorative treatment is costly, invasive, and increases a child’s risk of experiencing treatment-related morbidity and mortality.3,4 Furthermore, when left untreated, tooth decay can lead to problems with eating, sleeping, and learning.5-9 Dental caries in childhood is the strongest predictor of tooth decay in adulthood, which can negatively impact employment opportunities, compromise oral health-related quality of life, and exacerbate systemic diseases.10,11
Fluoride is one of the only evidence-based strategies available to prevent tooth decay.13 It helps maintain the balance between demineralization and remineralization during pH changes in the mouth caused by the intake of added sugars from foods and beverages.14-16 The main sources of fluoride include over-the-counter fluoride toothpastes and mouthrinses; professionally applied fluoride (varnishes); dentist-prescribed fluorides (tablets, drops, high-concentration toothpastes); and community water fluoridation (CWF).15,17-20 One potential side effect of excess fluoride is dental fluorosis, which occurs when too much fluoride is ingested during specific periods of tooth development.21 Other concerns, including links to lower IQ and systemic diseases such as cancer, are not supported by reliable scientific evidence.22
Although fluorides are considered safe when used as recommended, fluoride hesitancy among caregivers is a growing clinical and public health challenge.23 Defined as “a delay in acceptance, thoughts of refusal, or refusal despite availability,” about 42.3% of dentists report fluoride hesitancy as a growing problem and 81.3% of parents/caregivers are hesitant about dentist-applied topical fluorides such as varnish.23,24 Parallel concerns are present at the community level regarding CWF.25 Anti-fluoride sentiments are likely to intensify in the coming years given the statements about fluoride made by US Department of Health and Human Services Secretary Robert F. Kennedy, Jr., which have already prompted at least two states – Utah and Florida – to pass legislation banning CWF.26,27
Given the various forms of fluoride available to children and increasing levels of fluoride-related concerns among caregivers, dentists must tailor preventive care to ensure that all children have an opportunity to receive optimal exposure to fluoride commensurate with the child’s caries risk.
Determining a Child-Centered Fluoride Strategy
Following are steps used to determine an individualized, evidence-based fluoride strategy based on a combination of clinical practice guidelines and recent scientific data:28-30
- Conduct a Caries Risk Assessment
Various caries risk assessment tools are available, including “caries management by risk assessment” (CAMBRA) and the American Academy of Pediatric Dentistry’s caries risk assessment tool.28,31-34 While these tools use different approaches in helping clinicians to determine caries risk, they share features, including data collection in four ways: chart review, caregiver interview, clinical assessment, and radiograph assessment.
As part of the chart review, past dental disease and treatments should be examined, as well as determining the patient’s socioeconomic status, which can be assessed through proxies such as the child’s insurance type, annual household income, and the highest level of education attained by the caregiver.35,36 During the parent/caregiver interview, the dentist should take time to address any concerns he or she has, including questions about cavities. Dentists should also ask about the two most important factors in assessing caries risk: the child’s dietary behaviors, such as preferred foods and beverages, and oral hygiene routines, including toothbrushing frequency, use of fluoride toothpaste, and primary water source.37,38
The dentist will then perform an intraoral clinical assessment, which includes assessing plaque levels, examining the gums for gingival health, and checking for signs of both noncavitated and cavitated caries lesions. Radiographs may be indicated to identify interproximal tooth decay.
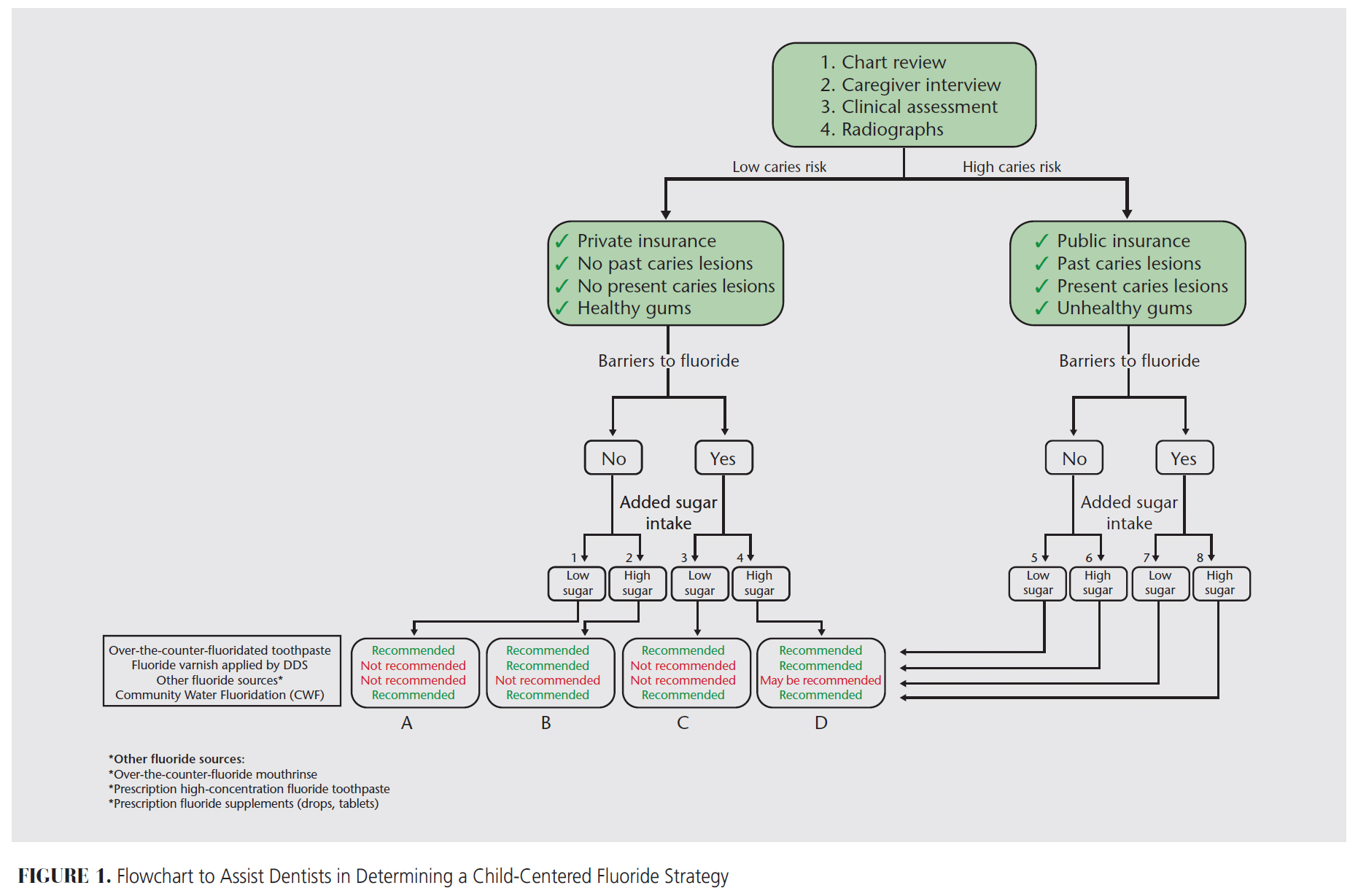
The information gleaned from these four sources of information (chart review, caregiver interview, clinical assessment, and radiographic assessment) will allow a dentist to classify each child as either low-risk or high-risk. While there are always exceptions, an assessment of four key factors can be used as a shorthand to assess caries risk: dental insurance type (private/public or uninsured), past caries history (no/yes), current caries (no/yes), and gingival health (healthy/unhealthy gums) (Figure 1).
- Identify Barriers to Fluoride
After classifying the child as low or high-risk for caries, the next step is to identify any barriers to fluoride (Figure 1). Given the growing prevalence of fluoride hesitancy, this evaluation is increasingly important. While fluoride hesitancy is associated with fluoride opposition, not all hesitant parents are opposed to all sources of fluoride. For instance, a parent/caregiver who is hesitant about topical fluoride is four times as likely to be receptive to fluoride toothpaste than fluoridated water.39
Consider whether the child is exposed to fluoride at home (eg, toothpaste), whether the family avoids drinking or using fluoridated water, and whether parents/caregivers are hesitant or opposed to any or all sources of fluoride. Another barrier to fluoride is living in an area without CWF. Up to 30% of the US population lives in an area without CWF. The goal is to understand the parent’s/caregiver’s beliefs about fluoride and identify which forms the child is currently exposed.
There are several ways to collect information on barriers to fluoride. One possibility is to include an item on a health history form that is updated at each child’s visit asking if the parent/ caregiver avoids fluoride by using nonfluoride toothpaste, bottled water, or a water filter that removes fluoride (eg, reverse osmosis). Dental offices may also consider using more extensive tools like the fluoride hesitancy identification tool, a validated 20-item Likert scale instrument that assesses a parent’s/caregiver’s level of fluoride hesitancy and identifies the underlying reasons for the hesitancy.40
- Assess Added Sugar Intake
The next step is assessing added sugar intake. The goal is to evaluate the presence, quantity, and frequency of foods and beverages consumed by the child that contain added sugars. Based on this evaluation, sugar consumption is categorized as low or high, serving as the final step before determining the appropriate fluoride recommendation (Figure 1).
To generate this information, a thorough dietary evaluation is ideal. This can be done by asking parents caregivers to recall the child’s typical weekday meals or by using a food diary.41 However, this is not always a practical chairside activity. Thus, we recommend a brief assessment of sugar-sweetened beverage consumption, as these are the leading source of added sugars in US children.37,42 Ask parents/caregivers about their child’s intake of sugar-sweetened beverage — whether the child consumes them daily, how many times per day, or if it is only on certain days like special occasions.
Child-Tailored Fluoride Strategy
Figure 1 illustrates eight pathways (1 to 8) that lead to four fluoride strategies (A, B, C, and D) based on a child’s caries risk, barriers to fluoride, and added sugar intake. Two common fluoride sources are part of all four fluoride strategies: over-the-counter toothpaste and CWF. These sources provide oral health benefits to all children, regardless of caries risk.17,20 Fluoride toothpastes should be used only after the first tooth has started to erupt into a child’s mouth at around age 6 months.
A nuance exists between fluoride varnish from a dentist and other fluoride sources (over-the-counter mouthrinses and prescription fluoride toothpaste, tablets, and drops).15,17-19 Fluoride varnish is recommended for all children with high sugar intake, as outlined in fluoride strategies B and D (pathways 2, 4, 6, and 8), and for high-risk children with low sugar intake (pathways 5 and 7). In contrast, fluoride varnish is not recommended for low-risk children with low sugar intake, as indicated in strategies A and C (pathways 1 and 3). This is based on clinical recommendations that varnish is indicated for children at high risk for caries.28 Similarly, other fluoride sources are not recommended in strategies A and C (pathways 1 and 3), with over-the-counter fluoride toothpaste and CWF providing sufficient protection against caries development.
Other sources of fluoride may be recommended for children with a low caries risk profile but with barriers to fluoride and high sugar intake, as indicated in fluoride strategy D (pathway 4). These include recommending prescription fluoride tablets or drops for a child who lives in an area without CWF. Other fluoride sources may also be recommended for children with a high caries risk profile regardless of their sugar intake, as indicated in strategy D (pathways 5, 6, 7, and 8). These could include the use of an over-the-counter fluoride mouthrinse for children who are able to spit (usually age 6 and older) or replacing over-the-counter toothpaste with a prescription high-concentration fluoride toothpaste for teenagers.
Parent Communication
Once an appropriate fluoride strategy is identified, clinical recommendations should be communicated to the child’s parent/caregiver, which can be a challenge when speaking to those who are opposed to fluoride.
Some parents/caregivers will follow all fluoride-related recommendations, while others may push back on some sources or share that they are opposed to all sources of fluoride. When communicating fluoride-related recommendations to a hesitant or opposed parent/caregiver, the goal is not to coax or convince a caregiver to accept fluoride. Pressuring caregivers violates the principle of preserving caregiver autonomy. It can also lead to a phenomenon known as reactance, in which a hesitant parent/caregiver becomes more strongly hesitant in response to perceived pressure from a healthcare provider to make a particular decision for his or her child (whether the pressure is intentional or inadvertent).43
Building trust with the parent/caregiver and using engaged and tailored communication techniques are important.44,45 Examples include the following:
- Using open-ended questions to understand why a parent/caregiver is hesitant about or opposed to fluoride
- Evaluating whether the parent/caregiver understands his or her child’s caries risk and how risk is tied to the recommended fluoride strategy
- Discussing sources of fluoride that are acceptable
- Identifying other prevention strategies such as ways to reduce caries risk by decreasing added sugar intake.
Conclusion
Fluoride is a safe and effective strategy in preventing pediatric tooth decay, a disease that continues to pose a significant public health challenge. To support dentists in selecting an appropriate fluoride prevention strategy for each child, we propose three main steps: conducting a caries risk assessment, identifying barriers to fluoride, and evaluating the child’s added sugar intake.
While there is no one-size-fits-all fluoride approach, the proposed clinical flowchart provides a more simplified way to derive fluoride-related recommendations that are tailored to a child’s specific caries risk and need for various forms of fluoride. The most difficult challenge may be in communicating a fluoride strategy to parents/caregivers and assessing the degree to which recommendations may need to be modified to account for concerns regarding specific forms of fluoride.
References
- GBD 2021 Oral Disorders Collaborators. Trends in the global, regional, and national burden of oral conditions from 1990 to 2021. Lancet. 2025;405:897–910.
- Stierman B, Afful J, Carroll MD, et al. National Health and Nutrition Examination Survey 2017–March 2020 prepandemic data files: development of files and prevalence estimates for selected health outcomes. Natl Health Stat Report. 2021:10.15620/cdc:106273.
- Coté CJ, Notterman DA, Karl HW, Weinberg JA, McCloskey C. Adverse sedation events in pediatrics: a critical incident analysis of contributing factors. Pediatrics. 2000;105(4 Pt 1):805–814.
- Kamat PP, McCracken CE, Simon HK, et al. Trends in outpatient procedural sedation: 2007–2018. Pediatrics. 2020;145:e20193977.
- Casamassimo PS, Thikkurissy S, Edelstein BL, Maiorini E. Beyond the dmft: the human and economic cost of early childhood caries. J Am Dent Assoc. 2009;140:650–657.
- Kastenbom L, Falsen A, Larsson P, Sunnegårdh-Grönberg K, Davidson T. Costs and health-related quality of life in relation to caries. BMC Oral Health. 2019;19:187.
- Quadros LN, Rebelo MAB, de Queiroz AC, Pereira JV, Vettore MV, Rebelo Vieira JM. Clinical consequences of untreated dental caries and school performance in low-income adolescents. Int J Paediatr Dent. 2021;31:619–626.
- Dunleavy G, Verma N, Raghupathy R, et al. Inequalities in oral health: estimating the longitudinal economic burden of dental caries by deprivation status in six countries. BMC Public Health. 2024;24:3239. doi:10.1186/s12889-024-17991-0
- Quadri MFA, Ahmad B. The mediation pathway linking dental caries and academic performance in children. Caries Res. 2024;58:1–10.
- Glied S, Neidell M. The economic value of teeth. J Hum Resour. 2010;45:468–496.
- Halasa-Rappel YA, Tschampl CA, Foley M, Dellapenna M, Shepard DS. Broken smiles: the impact of untreated dental caries and missing anterior teeth on employment. J Public Health Dent. 2019;79:231–237.
- Peres MA, Macpherson LMD, Weyant RJ, Daly B, et al. Oral diseases: a global public health challenge. Lancet. 2019;394:249–260.
- Whelton HP, Spencer AJ, Do LG, Rugg-Gunn AJ. Fluoride revolution and dental caries: evolution of policies for global use. J Dent Res. 2019;98:837–846.
- Kusano SC, Tenuta LMA, Del Bel Cury AA, Cury JA. Timing of fluoride toothpaste use and enamel-dentin demineralization. Braz Oral Res. 2011;25:383–387.
- Marinho VC, Worthington HV, Walsh T, Clarkson JE. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2013;7:CD002279.
- Zhang Q, Guan L, Guo J, et al. Application of fluoride disturbs plaque microecology and promotes remineralization of enamel initial caries. J Oral Microbiol. 2022;14:2105022.
- Walsh T, Worthington HV, Glenny AM, Marinho VC, Jeroncic A. Fluoride toothpastes of different concentrations for preventing dental caries. Cochrane Database Syst Rev. 2019;3:CD007868.
- Marinho VC, Chong LY, Worthington HV, Walsh T. Fluoride mouthrinses for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2016;7:CD002284.
- Tubert-Jeannin S, Auclair C, et al. Fluoride supplements (tablets, drops, lozenges or chewing gums) for preventing dental caries in children. Cochrane Database Syst Rev. 2011;12:CD007592.
- Iheozor-Ejiofor Z, Walsh T, Lewis SR, et al. Water fluoridation for the prevention of dental caries. Cochrane Database Syst Rev. 2024;10:CD010856.
- Wong MCM, Zhang R, Luo BW, Glenny AM, Worthington HV, Lo ECM. Topical fluoride as a cause of dental fluorosis in children. Cochrane Database Syst Rev. 2024;6:CD007693.
- Thorp H. Convergence and consensus. Science. 2025;388:339.
- Chi DL, Basson AA. Surveying dentists’ perceptions of caregiver refusal of topical fluoride. JDR Clin Trans Res. 2018;3:314–320.
- Lim J, Carle A, Carpiano R, Chi D. Topical fluoride hesitancy is significantly associated with topical fluoride opposition. J Dent Res. 2024;103(Spec Iss A):2721.
- Chi DL, Guinn S, Shands ME, Nemawarkar D, et al. Socioeconomic vulnerability and access to community water fluoridation in Washington. J Am Dent Assoc. 2024;155:747–754.
- Anderson O. RFK Jr. to tell CDC to change fluoride guidelines. ADA News. Available at adanews.ada.org/ada-news/2025/april/rfk-jr-to-tell-cdc-to-change-fluoride-guidelines. Accessed June 23, 2025.
- Cochrane E. Florida just banned fluoride from public water. Here’s what to know. New York Times. Available at nytimes.com/2025/05/15/ us/politics/florida-fluoride-water-ban.html. Accessed June 23, 2025.
- American Academy of Pediatric Dentistry. Caries-risk assessment and management for infants, children, and adolescents. In: The Reference Manual of Pediatric Dentistry. Chicago: American Academy of Pediatric Dentistry; 2024:306–312.
- Chi DL. Parent refusal of topical fluoride for their children: clinical strategies and future research priorities to improve evidence-based pediatric dental practice. Dent Clin North Am. 2017;61:607–617.
- Chi DL, Scott JM. Added sugar and dental caries in children: a scientific update and future steps. Dent Clin North Am. 2019;63:17–33.
- Featherstone JD, Chaffee BW. The evidence for caries management by risk assessment (CAMBRA®). Adv Dent Res. 2018;29:9–14.
- Christian B, Armstrong R, Calache H, Carpenter L, Gibbs L, Gussy M. A systematic review to assess the methodological quality of studies on measurement properties for caries risk assessment tools for young children. Int J Paediatr Dent. 2019;29:106–116.
- American Academy of Pediatrics. Oral health risk assessment tool. Available at https://downloads.aap.org/AAP/PDF/oralhealth_RiskAssessmentTool.pdf. Accessed June 23, 2025.
- Featherstone JD, Crystal YO, Alston P, Chaffee BW, Doméjean S, Rechmann P, et al. A comparison of four caries risk assessment methods. Front Oral Health. 2021;2:656558.
- Ortiz AS, Tomazoni F, Knorst JK, Ardenghi TM. Influence of socioeconomic inequalities on levels of dental caries in adolescents: a cohort study. Int J Paediatr Dent. 2020;30:42–49.
- Al-Rashdan O, AlZoubi Z, Ibrahimi M, Al-Khraisha A, Almajali N. Mother’s characteristics and socioeconomic status as possible risk factors for children’s caries in Jordan. Int J Dent. 2022;2022:2006088.
- Valenzuela MJ, Waterhouse B, Aggarwal VR, et al. Effect of sugar-sweetened beverages on oral health: a systematic review and meta-analysis. Eur J Public Health. 2021;31:122–129.
- Ha DH, Spencer AJ, Moynihan P, Thomson WM, Do LG. Excess risk of dental caries from higher free sugars intake combined with low exposure to water fluoridation. J Dent Res. 2021;100:1243–1250.
- Ko A, Chi DL. Fluoride hesitancy: a mixed methods study on decision-making about forms of fluoride. Community Dent Oral Epidemiol. 2023;51:997–1008.
- Carle AC, Pallotto I, Edwards TC, Carpiano R, Kerr DC, Chi DL. Psychometric properties of the Fluoride Hesitancy Identification Tool (FHIT). PLoS One. 2024;19:e0297188.
- Angelopoulou MV, Seremidi K, Benetou V, Agouropoulos A, Rahiotis C, Gizani S. Cariogenic diet assessment and analysis tools in children and adolescents: a systematic review. Oral Health Prev Dent. 2024;22:93-106.
- United States Centers for Disease Control and Prevention. Get the Facts: Sugar-Sweetened Beverages and Consumption. Available at cdc.gov/nutrition/php/data-research/sugar-sweetened-beverages.html. Accessed June 23, 2025.
- Adame BJ, Corman SR, Von Feldt PA, Meneses CM, O’Rourke HP, Tahir A. Reactance as a cause of COVID-19 vaccination hesitancy. Vaccine. 2025;57:127209.
- Cruz S, Kerr D, Chi DL. A qualitative assessment of factors influencing fluoride-hesitant parents’ trust of dentists. Pediatr Dent. 2023;45:133–141.
- Cruz S, Ko A, Chi DL. A qualitative study on dentists’ communication approaches in managing fluoride-hesitant caregivers. J Dent Res Clin Transl Res. 2023:23800844231203673.
From Decisions in Dentistry. October/November 2025;11(5):28-31.

