

Navigating Post-Frenectomy Wound Care
This systematic review explores recommendations for infant post-frenectomy wound care and suggestions for future research
PURCHASE COURSE
This course was published in the October 2023 issue and expires October 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the October 2023 issue and expires October 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 430
Educational Objectives
After reading this course, the participant should be able to:
- Discuss the prevalence and impact of ankyloglossia in infants and its relevance to breastfeeding and overall health.
- Explore the current state of post-frenectomy wound management, including varying approaches and the need for standardized protocols.
- Identify the complex variables involved in post-frenectomy care, including oral wound healing physiology, individual patient factors, and functional considerations.
Frenectomy is an effective treatment when ankyloglossia causes infant feeding difficulties. However, there is substantial variability in provider recommendations regarding wound management post-frenectomy for infants. A systematic approach to understanding, defining, and further researching best practice options for infant post-frenectomy wound care is needed. As such, we reviewed the literature on identifying clinical practices regarding infant post-frenectomy wound care, post-procedure recommendations, and oral wound healing physiology with the goal of noting variables that impact future research for post-frenectomy protocols.
Ankyloglossia, commonly known as tongue-tie, occurs when there is incomplete apoptosis of the lingual frenulum during embryogenesis. Ankyloglossia impacts 4% to 16% of infants born around the globe.1,2 Tongue-tie can negatively impact infant feeding and other health conditions.3–5
Throughout the literature, frenectomy is noted as beneficial when warranted, particularly regarding optimizing infant feeding, and the procedure is very low risk.6,7 Clinicians worldwide have varying approaches to wound management post-frenectomy. Many parents and clinicians have concerns around the potential for reattachment, adhesion formation, trauma, and stress post-procedure. Experience with post-frenectomy healing variables has led some clinicians to focus on healing by secondary intention.8 There is no commonly agreed upon post-frenectomy aftercare that is currently considered best-practice.
A systematic review was conducted to search for articles that examined the wound in patients undergoing lingual frenectomy or frenotomy for ankyloglossia. The inclusion criteria for articles included in this review were: discussed wound healing management in patients undergoing frenectomy/frenotomy for ankyloglossia; specified recommendations for the frequency, and/or duration, and/or type of active wound healing management in frenectomy/frenotomy patients; and limited treatment and post-operative care to 0 to 12 months of age.
The exclusion criteria were: articles that did not discuss post-frenectomy/frenotomy care for ages 0-12 months; nonscientific papers, guidelines, or conference proceedings; articles that focused on post-frenectomy/frenotomy care for those older than 12 months; and articles involving suturing post-frenectomy, lingual frenuloplasty.
Both MeSH terms and non-MeSH keywords were searched . MeSH terms allowed retrieval of articles containing word variants subsumed under that particular MeSH heading. MeSH subheadings of rehabilitation, surgery, therapy, and therapeutic use were employed as needed to aid in focusing searches. We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses method of reporting items for systematic reviews.9 Cochrane Library (n = 1), PubMed/Medline Database (n = 180), CINAHL (n = 118), Google (n = 83), and Up-To-Date (n = 1) databases were searched retrieving 383 records. Two additional records were obtained following a manual review of retrieved Medline article bibliographies. This produced 385 retrieved records, of which 299 were removed because they were duplicates, written in a language other than English, or were not relevant based on their titles. Of those left, 86 records remained for initial screening. Reviewing article abstracts removed 60 of these records as topically irrelevant, leaving 26 records that were screened against the eligibility criteria; 19 records failed to meet the eligibility criteria. A total of 79 records were eliminated as either irreverent or because the study did not meet eligibility criteria. This left seven studies that were analyzed in this article.
Data Collection
A systematic review was performed between 2017 and 2020. Our searches provided articles from 1977 to 2019, with a targeted focus on aftercare activities for infants undergoing lingual frenotomies/frenectomies. While searches were limited to humans and articles published in English, they were not restricted by study design. Article abstracts were then examined, and relevant articles were retrieved in full text. Bibliographies from retrieved articles were manually searched to locate additional articles not obtained in the initial search; we then retrieved those in full text.
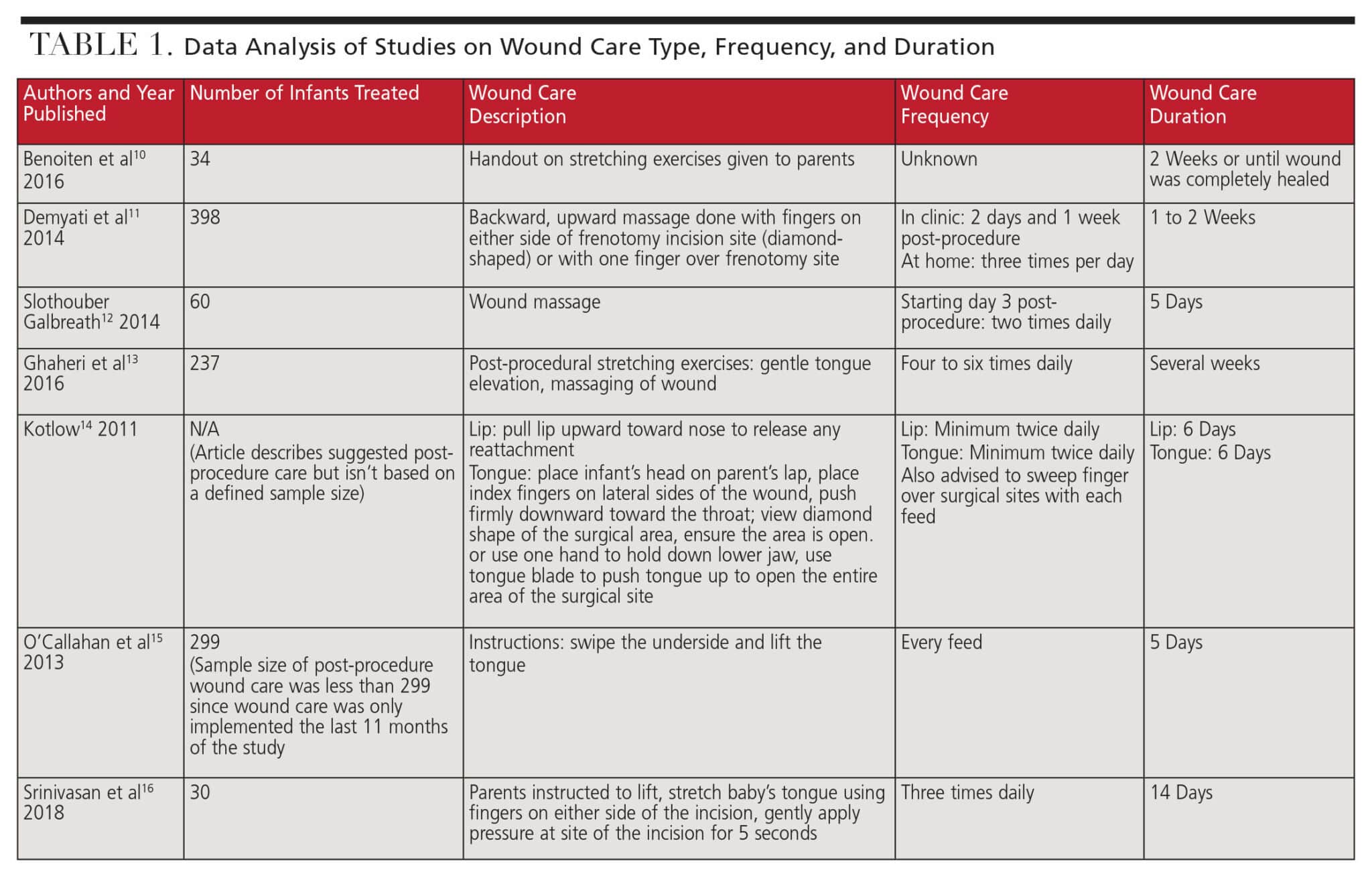
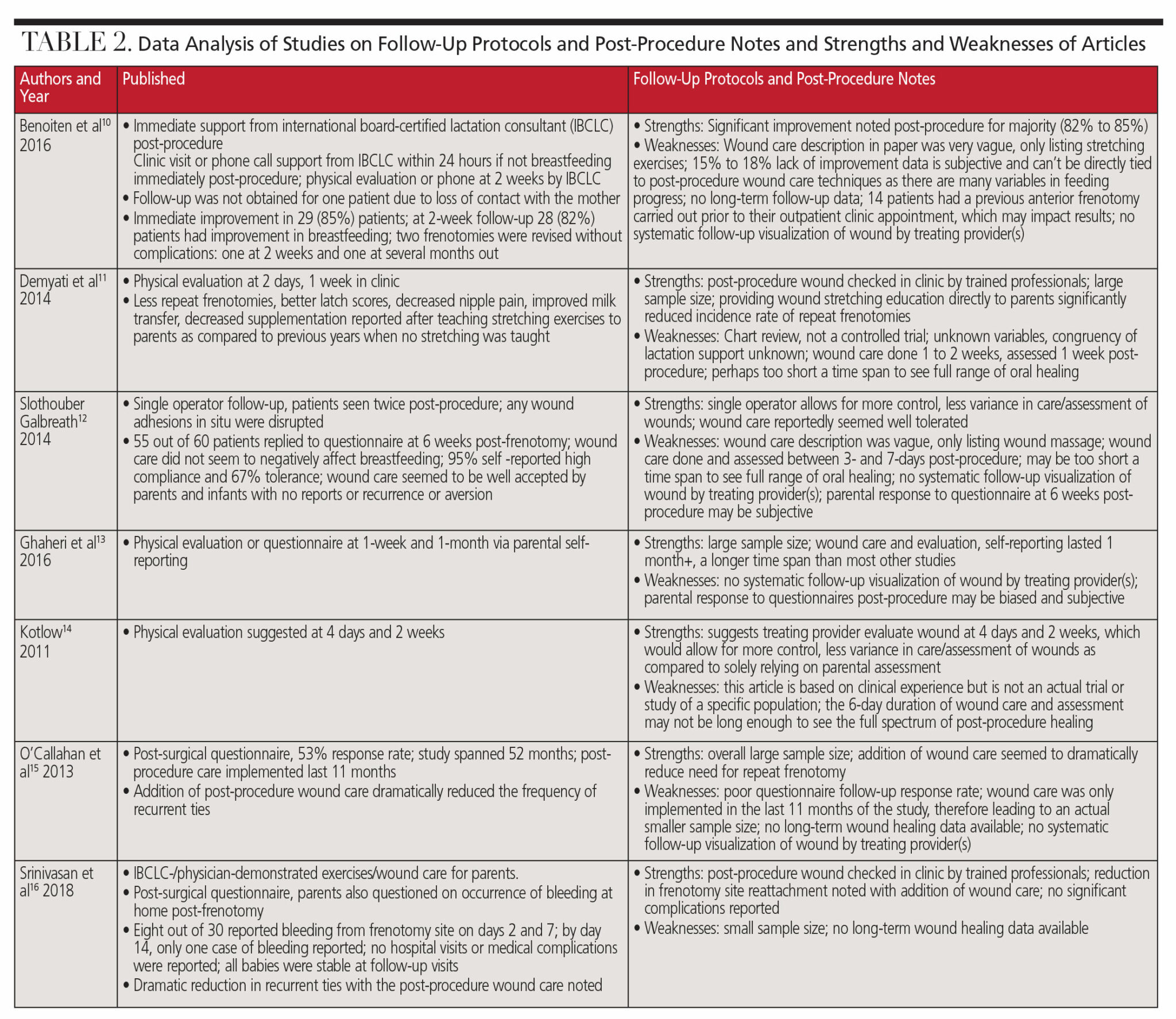
All three authors independently reviewed all full text articles, extracted data, and analyzed the information collected. Included papers were reviewed to assess the details regarding wound care prescribed for infants post-lingual frenectomy. Tables 1 and 2 detail the data analyses.10–16
![]()
![]() Clinical Relevance and Implications
Clinical Relevance and Implications
At the time we conducted our review, there were no high-level studies done solely on infant post-frenectomy wound care. In reviewing the available literature, we hope to gain a better understanding of the types of care being prescribed and assess the effectiveness of such care. In addition, we aim to integrate post-procedure recommendations with oral wound healing physiology and set the stage for further research considerations.
The literature has long pointed to the benefit of surgical release of the frenulum when ankyloglossia is impacting infant feeding and lactation.3,4,6,7,17,18 This review highlights the fact that post-procedural adhesions and reattachment are significant concerns for clinicians and parents. We acknowledge that there are few studies that include post-procedural wound care in their methodology.
All seven articles in our review found some benefit in implementing follow-up protocols, particularly reduced reattachment rates and frequency of repeat procedures. Our review revealed significant differences in wound care frequency, duration, technique, and follow up.
Several studies noted that wound care was well tolerated and without complications. This is clinically relevant because clinicians from multiple disciplines have noted concern around “regression leading to a repeat frenotomy due to a restrictive scar.”15,18
Post-frenectomy oral healing is unique because the goal is healing by secondary, not primary intention. The goal of healing by secondary intention is to not have the sides of the wound approximate and fuse together again, but rather have the wound heal from the base up, allowing for the site to maintain maximum surface space and prevent closure of the wound margins. Due to the placement of the post-frenectomy wound, the rapid nature of oral healing, and the goal of optimizing lingual range of motion and function, healing by secondary intention for this procedure appears to aid in the reduction of reattachment and repeat procedures.19
Abstract
Background:
Frenectomy is recognized as an effective treatment when ankyloglossia causes infant feeding difficulties. However, there is substantial variability in provider recommendations regarding wound management post-frenectomy for infants. There is a need for a systematic approach to understanding, defining and further researching best practice options for infant post-frenectomy wound care.
Research aim:
- To review the literature identifying clinical practices regarding infant post-frenectomy wound care.
- Integrate post-procedure recommendations and oral wound healing physiology.
- Identify variables that impact future research for post-frenectomy protocol development.
Methods:
Cochrane Library, PubMed/Medline Database and CINAHL, Web of Science, and bibliographic backtracking were searched for articles that discussed wound management for patients ages 0-12 months undergoing lingual frenectomy or frenotomy for ankyloglossia (n=7). Articles that did not meet our inclusion criteria were excluded (n=79).
Results:
At the end of our literature review process, seven studies were eligible for inclusion. Included papers described great variability regarding post-frenectomy wound care frequency, duration, and description of wound management. Two papers reported decreased rates of repeat procedures after post frenectomy wound care protocols were implemented. One paper reported wound management did not negatively affect infant feeding. However, clear wound management protocols were only sometimes included and were not the direct focus of any of the included papers.
While we can’t directly compare oral wound healing to dermal wound healing, other types of surgeries also carry the risk of “web-creep”and reattachment, particularly in the syndactyly literature.20,21 Since recurrence of webbing and contracture along incision lines happens with other procedures and anatomical sites, there may be potential value in exploring information from other surgical fields. The implication of the reviewed papers demonstrates potential benefit of some type of wound management post-frenectomy to optimize healing, but there is still much to be learned.
Beyond healing of the wound, other variables should be considered when it comes to post-frenectomy care for infants. There is great individual variability of the lingual frenulum itself including microanatomical structure, histological composition, collagen types, thickness, and more.22 Lingual nerve branches are superficially located on the ventral tongue surface, beneath a fascial layer. These nerves may impact sensation and movement patterns. Given the vast diversity of frenula, individualized post-operative care may be best. Pre- and post-procedural neonatal oral motor skills, lingual function, feeding patterns, pain, sensitivity, oral somatosensory awareness, and healthy attachment in the caregiver all must be taken into account, as well.23-31
When contemplating future research methodology, the fact that the wound itself always is attached to a baby who has unique needs, functional abilities, and sensitivities must be remembered. While exploring wound care, we must also consider the experience of the infant and family, and functional and phenomenological implications.
Limitations
One limitation of this review is the quality and focus of the retrieved studies. While all included papers discussed post-frentomy/frenectomy care, this was not the primary focus for most. In addition, several studies described their wound care in detail. However other studies were more vague.
While all studies seem to point to a benefit of some type of wound care, the development of best practices cannot be clearly defined from the papers reviewed. At present, no universally accepted protocols for assessing for ankyloglossia have been determined, let alone standards for surgical techniques or quantifying healing results.32 We recognize that further studies around this topic will require carefully designed methodology due to the personalized nature and many variables involved in wound healing, oral function, infant feeding, and oral somatosensory awareness.
Conclusion
Studies on post-frenectomy wound management are not robust enough to draw specific conclusions about what constitutes best practice. However, this review does point to evidence around the need to proactively support wound healing by secondary intention post-frenectomy. We propose that future research consider ways to quantify and qualify oral functional improvements post-procedure. We also hope researchers will consider evaluating options that prevent oral wound adhesions while optimizing oral function. Robust evidence demonstrates the importance of breastfeeding.33,34 Frenectomy to resolve infant ankyloglossia optimizes feeding and lactation issues on many levels.35 As global communities continue to work on supporting the initiation and duration of breastfeeding, researching related issues and care options that could help improve these rates is important.33
References
- Ngerncham S, Laohapensang M, Wongvisutdhi T, et al. Lingual frenulum and effect on breastfeeding in Thai newborn infants. Paediatric Interntional Child Health. 2013;33:86-90.
- Segal LM, Stephenson R, Dawes M, Feldman P. Prevalence, diagnosis, and treatment of ankyloglossia: methodologic review. Canadian Family Physician. 2007;53(6):1027-1033.
- Francis DO, Chinnadurai S, Morad A, et al. Treatments for ankyloglossia and ankyloglossia with concomitant lip-tie. In: Treatments for Ankyloglossia and Ankyloglossia With Concomitant Lip-Tie. Rockville, Maryland: Agency for Healthcare Research and Quality (US); 2015 May. Report No:15-EHC011-EF.
- Lalakea ML, Messner AH. Ankyloglossia: does it matter? Pediatr Clin North Am. 2003;50:381-397.
- Zaghi S, Valcu-Pinkerton S, Jabara M, et al. Lingual frenuloplasty with myofunctional therapy: Exploring safety and efficacy in 348 cases. Laryngoscope Investig Otolaryngol. 2019;4:489-496.
- Edmunds J, Miles SC, Fulbrook P. Tongue-tie and breastfeeding: a review of the literature. Breastfeed Rev. 2011;19:19-26.
- O’Shea JE, Foster JP, O’Donnell CP, et al. Frenotomy for tongue-tie in newborn infants. Cochrane Database Syst Rev. 2017;3:CD011065.
- Bernstein G. Healing by secondary intention. Dermatol Clin. 1989;7:645-660.
- Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA Statement. Open Medicine. 2009;3:e123-130.
- Benoiton L, Morgan M, Baguley K. Management of posterior ankyloglossia and upper lip ties in a tertiary otolaryngology outpatient clinic. Int J Pediatr Otorhinolaryngol. 2016;88:13-16.
- Demyati E, Stern M, Goldfarb L, Srinivasan A, Mitnick H, Dobrich C. Ankyloglossia in breastfeeding infants: stretching exercises post-frenotomy and the efficacy of the procedure. J Hum Lact. 2014;ILCA Abstracts.
- Slothouber Galbreath J, Fisher K, Patel S. Does postoperative wound massage improve outcome of frenulotomy for breastfeeding .difficulties in infants? J Hum Lact. 2014;30:501.
- Ghaheri BA, Cole M, Fausel SC, Chuop M, Mace JC. Breastfeeding improvement following tongue-tie and lip-tie release: a prospective cohort study. Laryngoscope. 2017;127:1217-1223.
- Kotlow L. Diagnosis and treatment of ankyloglossia and tied maxillary fraenum in infants using Er:YAG and 1064 diode lasers. Eur Arch Paediatr Dent. 2011;12:106-112.
- O’Callahan C, Macary S, Clemente S. The effects of office-based frenotomy for anterior and posterior ankyloglossia on breastfeeding. Int J Pediatr Otorhinolaryngol. 2013;77:827-832.
- Srinivasan A, Al Khoury A, Puzhko S, et al. Frenotomy in infants with tongue-tie and breastfeeding problems. J Hum Lact. 2018:890334418816973.
- Frenectomy for the Correction of Ankyloglossia: A Review of Clinical Effectiveness and Guidelines. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health: June 15, 2016.
- Klockars T, Pitkaranta A. Pediatric tongue-tie division: indications, techniques and patient satisfaction. Int J Pediatr Otorhinolaryngol. 2009;73:1399-1401.
- Larjava H. Oral Wound Healing: Cell Biology and Clinical Management. Chichester, West Sussex, UK: Wiley-Blackwell; 2012.
- Chopra K, Tadisina KK, Patel KR, Singh DP. Syndactyly repair. Eplasty. 2013;13:ic51.
- Dao KD, Shin AY, Billings A, Oberg KC, Wood VE. Surgical treatment of congenital syndactyly of the hand. J Am Acad Orthop Surg. 2004;12:39-48.
- Mills N, Geddes DT, Amirapu S, Mirjalili SA. Understanding the lingual frenulum: histological structure, tissue composition, and implications for tongue tie surgery. Int J Otolaryngol. 2020;2020:1820978.
- Haggard P, de Boer L. Oral somatosensory awareness. Neurosci Biobehav Rev. 2014;47:469-484.
- Witt N, Coynor S, Edwards C, Bradshaw H. A guide to pain assessment and management in the neonate. Curr Emerg Hosp Med Rep. 2016;4:1-10.
- Meek J, Huertas A. Cochrane review: Non-nutritive sucking, kangaroo care and swaddling/facilitated tucking are observed to reduce procedural pain in infants and young children. Evid Based Nurs. 2012;15:84-85.
- Larsson BA. [Pain and pain relief during the neonatal period. Early pain experiences can result in negative late-effects]. Lakartidningen. 2001;98:1656-1662.
- Schwaller F, Fitzgerald M. The consequences of pain in early life: injury-induced plasticity in developing pain pathways. Eur J Neurosci. 2014;39:344-352.
- Grunau RE. Neonatal pain in very preterm infants: long-term effects on brain, neurodevelopment and pain reactivity. Rambam Maimonides Med J. 2013;4:e0025
- Bovey A, Noble R, Noble M. Orofacial exercises for babies with breastfeeding problems? Breastfeed Rev. 1999;7:23-28.
- Greene Z, O’Donnell CP, Walshe M. Oral stimulation for promoting oral feeding in preterm infants. Cochrane Database Syst Rev. 2016;9:CD009720.
- Younesian S, Yadegari F, Soleimani F. Impact of oral sensory motor stimulation on feeding performance, length of hospital stay, and weight gain of preterm infants in NICU. Iran Red Crescent Med J. 2015;17:e13515.
- Walsh J, Links A, Boss E, Tunkel D. Ankyloglossia and lingual frenotomy: national trends in inpatient diagnosis and management in the United States, 1997-2012. Otolaryngol Head Neck Surg. 2017;156:735-740.
- Kramer MS, Kakuma R. Optimal duration of exclusive breastfeeding. Cochrane Database Syst Rev. 2012;2012(8):CD003517.
- Brownell EA, Hagadorn JI, Lussier MM, et al. Optimal periods of exclusive breastfeeding associated with any breastfeeding duration through one year. J Pediatr. 2015;166:566-570.
- Francis DO, Krishnaswami S, McPheeters M. Treatment of ankyloglossia and breastfeeding outcomes: a systematic review. Pediatrics. 2015;135:e1458-1466.
From Decisions of Dentistry. October 2023; 9(9):28-31

