

Minimizing Aerosols in Dental Practice
Use of silver diamine fluoride and the atraumatic restorative technique can help minimize aerosols during dental procedures.
In early 2020, the COVID-19 pandemic negatively impacted dental care worldwide. Globally, dental offices were initially forced to close, allowing for emergency treatment only. Supply and demand chains were woefully unprepared to deal with the pandemic, further complicating the delivery of oral health care. With the introduction of vaccines for SARS-CoV-2,1 the virus responsible for COVID-19, the United States’ economy is slowly recovering and dental practices are seeing patient visits return to pre-pandemic levels. As a result of ongoing disease, however, an emphasis on reducing viral transmission continues.
Understanding of COVID-19 transmission is evolving. The primary known mode of transmission for COVID-19 is through respiratory droplets.2 According to the U.S. Centers for Disease Control and Prevention, COVID-19 can be detected in saliva, but whether aerosolized saliva can infect a susceptible host is yet to be determined.3 As the pandemic continues, clinicians have sought alternate ways to minimize the risk of COVID-19 transmission in oral health care settings, including minimization of dental aerosols. The Occupational Safety and Health Administration states, “In dentistry, using dental turbines, micro-motor handpieces, ultrasonic scalers, and air-water syringes are examples of tasks that can generate aerosols.”4
Oral health professionals are already familiar with some of the techniques used to eliminate or limit dental aerosol production, particularly those who engage in community service or mission work. Examples include use of silver diamine fluoride (SDF) or the atraumatic restorative technique (ART), which both help reduce exposure. Among other methods of minimizing or limiting aerosols is the use of high-volume evacuators and air management systems, such as air purifiers.
Clinicians who treat patients with special needs, older adults, and other vulnerable populations commonly employ treatment modalities that limit aerosol production. Minimizing or limiting aerosols is vital because medically vulnerable individuals may have other chronic conditions leading to a weak respiratory system, making them at higher risk for respiratory infections, such as aspiration pneumonia.5 This is a condition that can be fatal in individuals with compromised respiratory issues, such as chronic obstructive pulmonary disorder, asthma, chronic bronchitis, emphysema and lung cancer. Therefore, as a preventive dental measure, use of SDF and ART may be beneficial for the broader population during the pandemic.
![FIGURE 1. Application of silver diamine fluoride.]() SILVER DIAMINE FLUORIDE
SILVER DIAMINE FLUORIDE

With an action similar to fluoride varnish, SDF was approved as a desensitizing agent by the U.S. Food and Drug Administration (FDA) in August 2014. However, this material has been used in other parts of the world — including Japan, New Zealand, Australia and Argentina — for decades with minimal adverse reactions.6 In the United States, SDF was awarded breakthrough therapy status by the FDA in 2016 for treatment of dental caries.7,8
A 2016 systematic review revealed that application of 38% SDF in children arrested 65% of active lesions when applied at least once a year (Figure 1).9 If applied twice a year, SDF has been shown to arrest more than 90% of caries.7 As such, SDF is now used in the United States as a desensitizing agent, preventive agent, and a caries arresting agent, either alone or in conjunction with a restoration (Table 1). While fluoride varnish is most effective in remineralization of the enamel, SDF is most effective at arresting caries of the dentin and root surfaces.10 This material is noninvasive, easy to apply, cost effective, and is safe for most patients;11 in fact, among some geriatric, pediatric and public health dentists, SDF is referred to as the “silver bullet.”12
While the majority of studies on SDF effectiveness have been done with pediatric, geriatric and other vulnerable populations, the potential benefits of using SDF more broadly outweigh the adverse effects, namely, staining — which is a concern, especially with anterior teeth.13 The major shortcoming of SDF is that it will stain caries and plaque a dark brown-to-black color. Newer products have added potassium iodide to reduce staining issues.14 Because it is taken up by saliva, the stain may affect caries and plaque in areas that were not originally intended for treatment.15 There are no specific postoperative instructions. If reapplication is needed depending on the original diagnosis, treatment plan and prognosis, application is recommended twice per year for caries arrest and prevention.
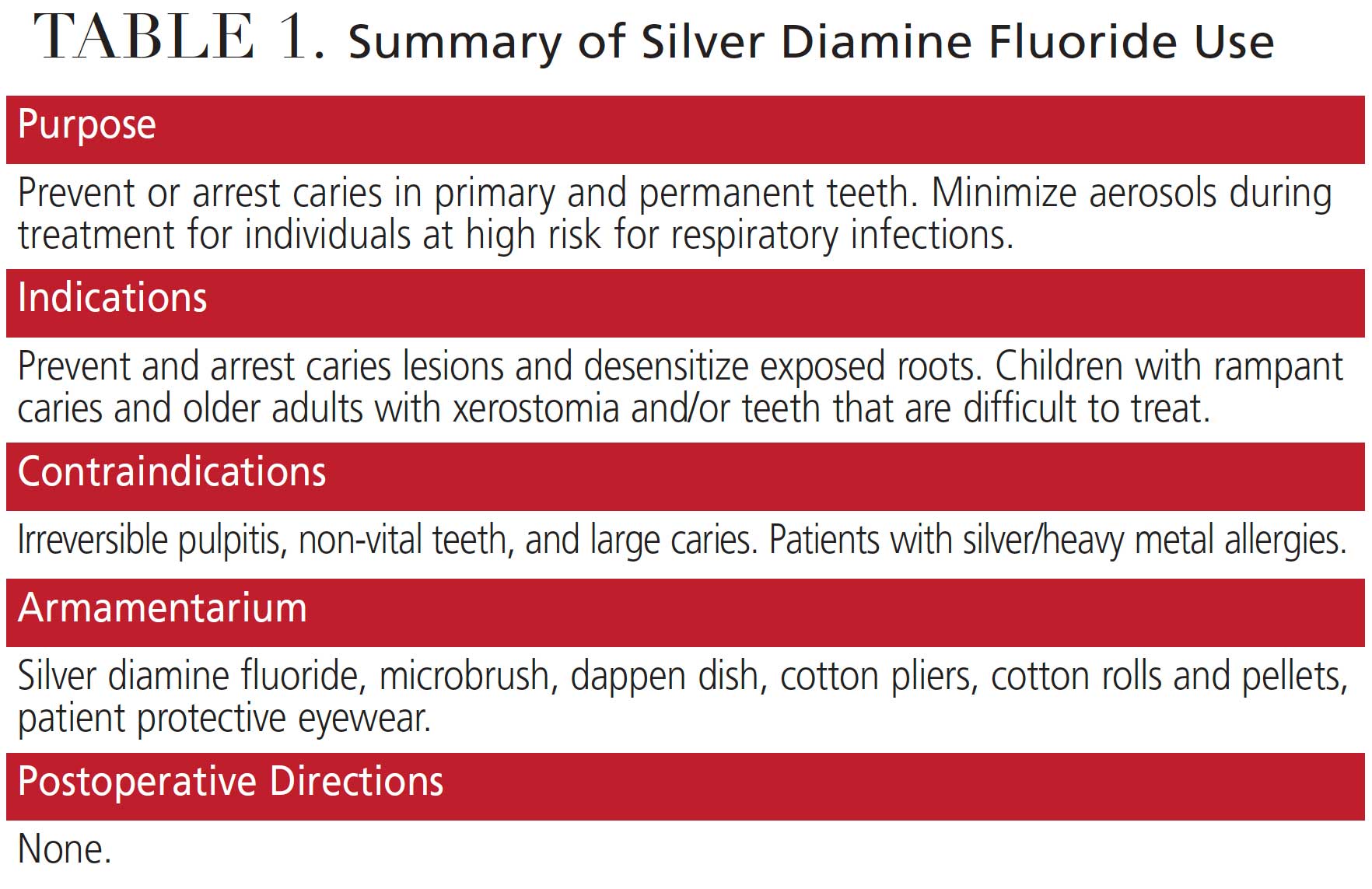
For example, SDF can be used to desensitize teeth/roots and prevent or arrest caries in primary and permanent teeth, whether due to early childhood caries or xerostomia.11,16,17 It is also an effective treatment option for other vulnerable patients with behavioral or medical management concerns. Use of this material allows the provider to treat more lesions in one visit, which limits access-to-care barriers for patients who have difficulties visiting a dental office.12
There are contraindications to SDF administration, including:
- Patients with an allergy to silver or other heavy metals may experience adverse effects with SDF.
- This medicament should not be used on teeth with pulpal involvement, and it is not recommended for use on teeth with large caries or exposed pulp18 — although it is indicated for remineralization of tooth structure to prevent pulpal exposure.19 Similarly, it is not recommended for teeth with diagnosis of irreversible pulpitis, necrotic pulp or periapical disease.20
While there are no reported health complications for suitable patients, a reaction to the silver ingredient may be a possibility. As a standard of clinical care, the use of protective eyewear is recommended for the application of SDF.21 Lastly, because SDF can stain operatory surfaces, proper handling and disposal is important.
The American Dental Association’s Code on Dental Procedures and Nomenclature (CDT) lists codes that can be used to bill insurance companies for SDF application:
- D1208: Topical application of fluoride for prevention
- D9910: Topical application of desensitizing medicament for sensitivity
- D1354: Interim caries arresting medicament of fluoride varnish for treating caries/per tooth application
![FIGURES 2A and 2B. Application of the atraumatic restorative technique (A, B).]() ATRAUMATIC RESTORATIVE TECHNIQUE
ATRAUMATIC RESTORATIVE TECHNIQUE

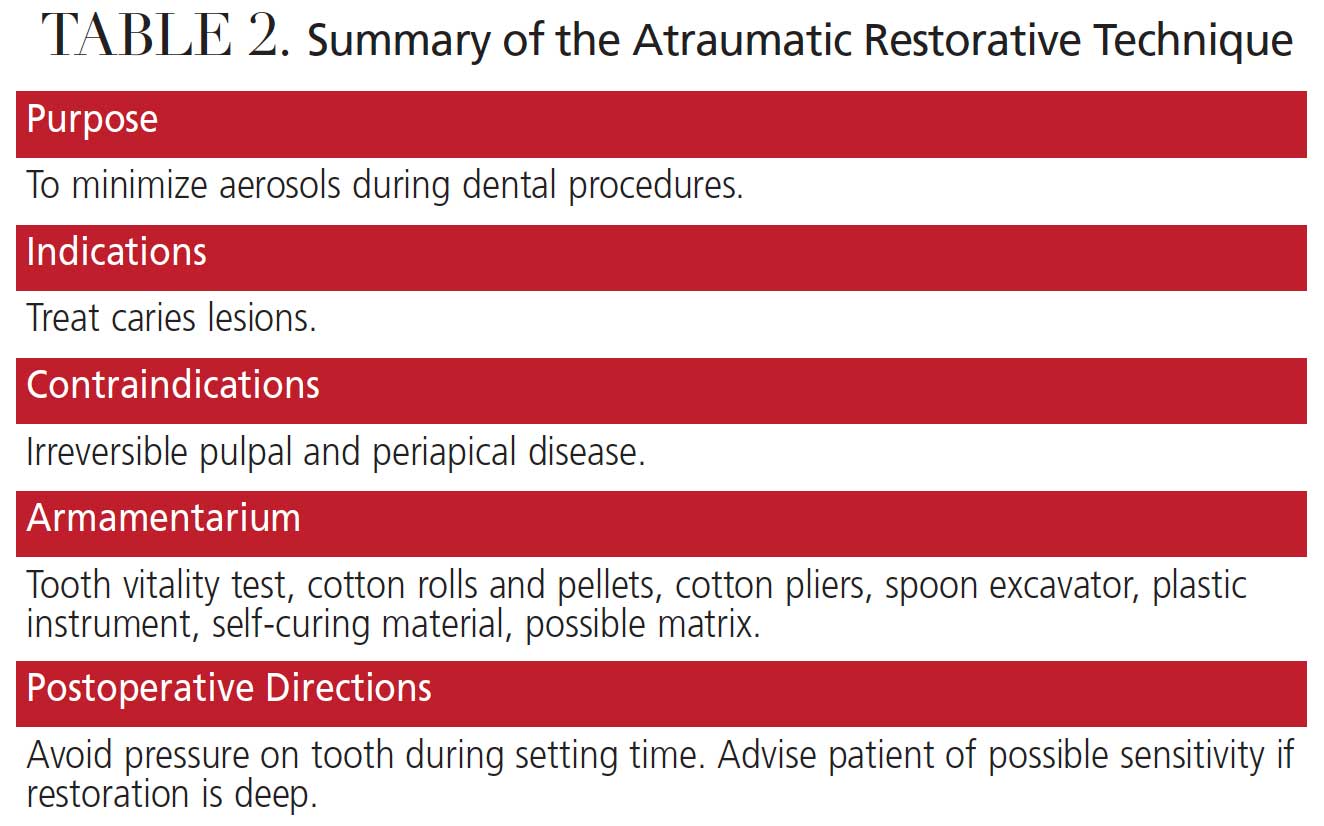
Another approach to minimize aerosol generation is using hand instruments instead of a handpiece for restorative procedures. This delivery, known as ART, has long been employed in the public health sector and is another alternative for treating caries lesions (Figures 2A and 2B). The ART approach includes preventive, minimally invasive care that prevents further development of caries, particularly in medically and socioeconomically vulnerable patients.22 In some cases, ART restorations are considered definitive restorations, while in other instances they are considered interim. The latter are often referred to as interim therapeutic restorations (ITR).
A 25-year comprehensive overview describes the ART restorative approach as precisely creating sufficient tooth or root surface access for the removal of only the soft, demineralized (decomposed) dentin with hand instrumentation.22 Caries removal is followed by restoration with an adhesive dental material;23 for example, glass ionomer is generally used in pediatric dentistry and for root caries in geriatric patients. When using SDF, cavity conditioner plays an important role.24 Simultaneously, the provider seals any remaining pits and fissures that remain at risk.25 If the lesion is excavated with rotating instruments, it is not considered ART or modified ART. This approach has spread globally; in many countries, in fact, ART is part of the dental curriculum due to conducive clinical outcomes in young children and older adults.26
Research has found that partial caries removal was associated with a significant reduction in pulp exposure in asymptomatic teeth with deep caries.27 The intentional retention of caries within a restorative preparation is a significant paradigm in caries management, and the level and quality of evidence is compelling. Partial caries removal with ART minimizes trauma to the tooth. This technique typically does not involve the use local anesthetic or a handpiece, and there is minimal chance of unintended pulpal exposure.28 There are no medical contraindications to the ART approach or partial caries removal techniques, although patients with an allergy to the dental materials used for the restoration should be excluded (Table 2). Postoperatively, patients should be advised to avoid putting pressure on the restored tooth for the duration of the final setting time. If the restoration was deep and postoperative sensitivity is anticipated, advise the patient accordingly. This approach is not recommended for use on teeth with a diagnosis of irreversible pulpitis, necrotic pulp or periapical disease. Also, patients with cognitive decline or management issues may not be suitable for this technique.
The CDT code used for billing will depend on the diagnosis and rationale for use of ART or ITR:
- D2941: Interim therapeutic restoration: primary dentition
- D2940: Protective restoration
- Codes for definitive resin restorations of primary or permanent teeth
CONCLUSION
The COVID-19 pandemic forced oral healthcare providers to pursue alternative methods to ensure patient and operator safety. Minimizing dental aerosols which may contain SARS-CoV-2 is a strategy that is easily implemented by using SDF and ART. The ART approach helps minimize aerosol production, while application of SDF minimizes the need to use a dental handpiece. Oral health professionals may offer a great service to patients at elevated risk of developing caries due to other conditions or medications by providing care utilizing alternative, aerosol-reducing clinical techniques.
The authors have no commercial conflicts of interest to disclose.
KEY TAKEAWAYS
- In light of the COVID-19 pandemic, oral health professionals have sought alternative practices to minimize the risk of COVID-19 transmission during care, including techniques to reduce dental aerosols.
- Approaches to minimize aerosols include the use of silver diamine fluoride (SDF) and the atraumatic restorative technique (ART).
- The use of SDF has been approved by the U.S. Food and Drug Administration as a desensitizing agent, and it was awarded breakthrough therapy status in 2016 for treatment of dental caries.7,8
- As such, SDF is now used in the United States as a desensitizing agent, preventive agent, and a caries arresting agent, either alone or in conjunction with a restoration.
- The major shortcoming of SDF is that it will stain caries and plaque a dark brown-to-black color.
- Care delivery via ART minimizes concerns with dental aerosols because caries preparation is done with hand instrumentation, rather than rotary instruments.
- In some cases, ART restorations are considered definitive restorations, while in other instances they are considered interim. The latter are often referred to as interim therapeutic restorations.
- Where indicated, treatment utilizing SDF and ART can effectively reduce or eliminate dental aerosols, thus reducing the risk of SARS-CoV-2 transmission in dental settings.
REFERENCES
- U.S. Food and Drug Administration. COVID-19 Vaccines. Available at: http/://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/covid-19-vaccines. Accessed May 12, 2021.
- World Health Organization. Modes of transmission of virus causing COVID-19: implications for IPC precaution recommendations. Available at: https://www.who.int/news-room/commentaries/detail/modes-of-transmission-of-virus-causing-covid-19-implications-for-ipc-precaution-recommendations. Accessed May 12, 2021.
- Santosh TS, Parmar R, Anand H, Srikanth K, Saritha M. A review of salivary diagnostics and its potential implication in detection of COVID-19. Cureus. 2020:12:e7708.
- U.S. Department of Labor Occupational Safety and Health Administration. Dentistry Workers and Employers. Available at: https://www.osha.gov/SLTC/covid-19/dentistry.html. Accessed May 12, 2021.
- Mandell LA, Niederman MS. Aspiration pneumonia. N Eng J Med. 2019;380:651–663.
- Möhler JS, Sim W, Blaskovich MA, Cooper MA, Ziora ZM. Silver bullets: a new lustre on an old antimicrobial agent. Biotechnol Adv. 2018;36:1391–1411.
- Horst JA. Silver fluoride as a treatment for dental caries. Adv Dent Res. 2018;29:135–140.
- U.S. Food and Drug Administration. Breakthrough Therapy. Available at: https://www.fda.gov/patients/fast-track-breakthrough-therapy-accelerated-approval-priority-review/breakthrough-therapy. Accessed May 12, 2021.
- Crystal YO, Niederman R. Silver diamine fluoride treatment considerations in children’s caries management. Pediatr Dent. 2016;38:466–471.
- Gao SS, Zhang S, Mei ML, Lo EC, Chu CH. Caries remineralisation and arresting effect in children by professionally applied fluoride treatment — a systematic review. BMC Oral Health. 2016;16:12.
- Horst JA, Ellenikiotis H, UCSF Silver Caries Arrest Committee, Milgrom PL. UCSF protocol for caries arrest using silver diamine fluoride: rationale, indications and consent. J Calif Dent Assoc. 2016;44:16–28.
- 12. Rosenblatt A, Stamford TC, Niederman R. Silver diamine fluoride: a caries “silver-fluoride bullet.” J Dent Res. 2019;88:116–125.
- 13. Crystal YO, Kreider B, Raveis VH. Parental expressed concerns about silver diamine fluoride (SDF) treatment. J Clin Pediatr Dent. 2019;43:155–160.
- Patel J, Anthonappa RP, King NM. Evaluation of the staining potential of silver diamine fluoride: in vitro. Int J Paediatr Dent. July 4, 2018. Online ahead of print.
- Hosoya Y, Watanabe E, Tadokoro K, Inoue T, Miyazaki M, Tay FR. Effects of ammonium hexafluorosilicate application on demineralized enamel and dentin of primary teeth. J Oral Science. 2012;54:267–272.
- Gold J. Silver diamine fluoride arrests caries in primary teeth. J Evid Based Dent Pract. 2018;18:88–90.
- Chu CH, Lee AH, Zheng L, Mei ML, Chan GC. Arresting rampant dental caries with silver diamine fluoride in a young teenager suffering from chronic oral graft versus host disease post-bone marrow transplantation: a case report. BMC Res Notes. 2014;7:3.
- Hu S, Meyer B, Duggal M. A silver renaissance in dentistry. Eur Arch Paediatr Dent. 2018;19:221–227.
- Zhi QH, Lo EC, Lin HC. Randomized clinical trial on effectiveness of silver diamine fluoride and glass ionomer in arresting dentine caries in preschool children. J Dent. 2012;40:962–967.
- Felemban OM, Dabroom WA, Alsharif MT, et al. The effect of silver diamine fluoride in preventing secondary caries in primary teeth: in-vitro study. EC Dental Science. 2018;17:1564–1569.
- Allred A, Moulding LR, Stewart PW. Dental patients’ perceptions and understandings towards the use of protective eyewear during dental procedures. Doctoral dissertation. Weber State University. 2016.
- Frencken JE, Leal SC, Navarro MF. Twenty-five-year atraumatic restorative treatment (ART) approach: a comprehensive overview. Clin Oral Investig. 2012;16:1337–1346.
- Perdigão J. Current perspectives on dental adhesion: (1) Dentin adhesion — not there yet. Jpn Dent Sci Rev. 2020;56:190–207.
- Mazaheri R, Pishevar L, Shichani AV, Geravandi S. Effect of different cavity conditioners on microleakage of glass ionomer cement with a high viscosity in primary teeth. Dent Res J (Isfahan). 2015;12:337–341.
- Borsatto MC, Thomaz MY, Contente MM, et al. Bonding agent underneath sealant: shear bond strength to oil-contaminated. Braz Dent J. 2010;21:50–54.
- da Mata C, Allen PF, Cronin M, O’Mahony D, McKenna G, Woods N. Cost-effectiveness of ART restorations in elderly adults: a randomized clinical trial. Community Dent Oral Epidemiol. 2014;42:79–87.
- Frencken JE. Atraumatic restorative treatment and minimal intervention dentistry. Br Dent J. 2017;223:183–189.
- Karim A, Mascarenhas AK, Dharamsi S. A global oral health course: isn’t it time? J Dent Ed. 2008;72:1238–1246.
From Decisions in Dentistry. June 2021;7(6)16-18,21.
