

Medication Use and Gingival Enlargement
Understanding the etiology, risk factors and treatment options for drug-related gingival overgrowth.
Understanding the etiology, risk factors and treatment options for drug-related gingival overgrowth
This course was published in the March 2016 issue and expires 03/31/19. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the different types of drugs that may cause gingival enlargement.
- Identify the clinical features of gingival enlargement.
- Explain the etiology and risk factors of drug-induced gingival
enlargement. - List the available options for treating this condition.
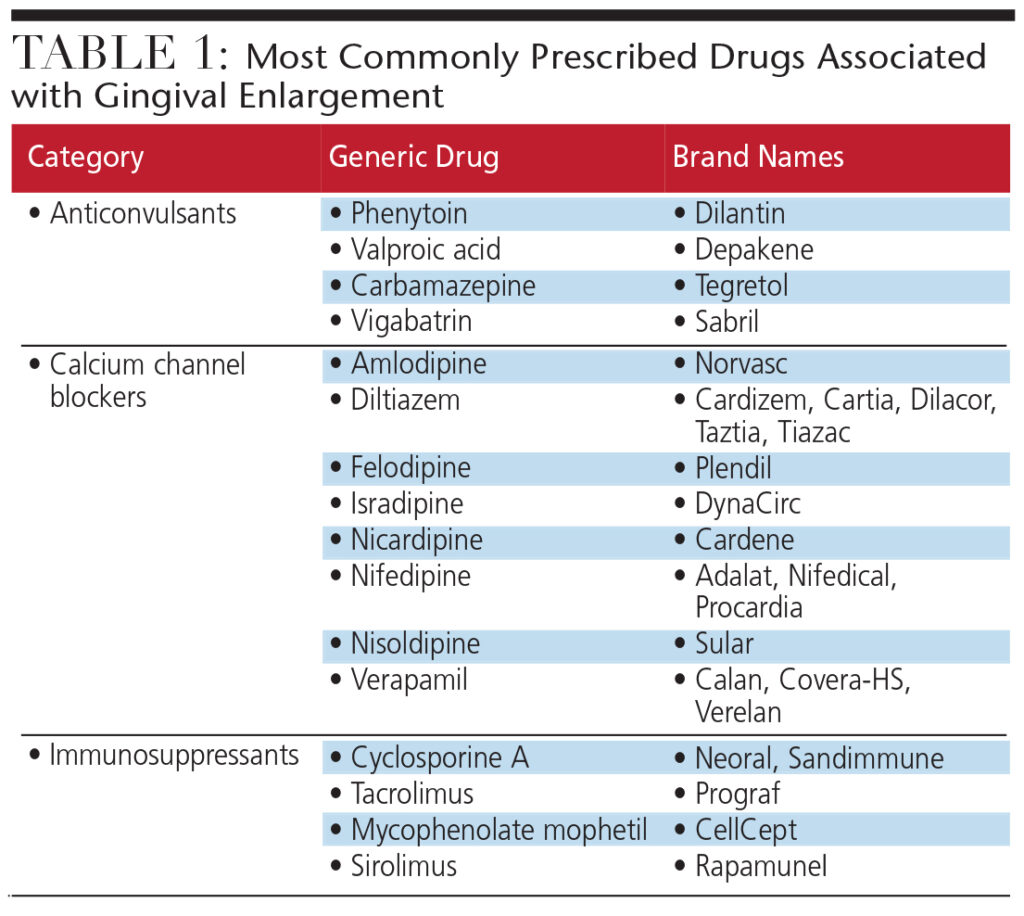
Bacteria, viruses, neoplasms and certain drugs can negatively affect gingival health. Gingival enlargement raises the risk of infection, caries and periodontal disease, and negatively affects smile esthetics. Initiated by both systemic and inflammatory factors, gingival enlargement is often caused by common prescription medications. These drugs — anticonvulsants, calcium channel blockers (CCBs) and immunosuppressants — promote changes in fibroblast function, which lead to an increase in the extracellular matrix of the gingival connective tissue (Table 1). In order to restore normal fibroblast function and gingival health, another drug may need to be substituted for the offending medication. When substitution is not feasible, surgical excision of gingival tissue may provide temporary relief to patients affected by drug-induced gingival enlargement.
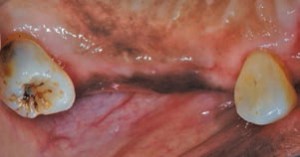
The discovery of phenytoin in 1938 by Merritt and Putnam provided a major breakthrough in the management of patients with epilepsy.1 Shortly after its introduction, however, reports linking phenytoin to gingival overgrowth began to surface.2 Susceptibility to this drug is not universal, as the prevalence of benign enlargement varies among population subsets. Gingival enlargement induced by anticonvulsants is significantly higher among children and institutionalized patients. For noninstitutionalized patients, the prevalence of gingival overgrowth caused by phenytoin is approximately 50%, and the condition most often affects the maxillary anterior teeth (Figure 1).3 Gingival enlargement typically appears two months to three months after the first dose of phenytoin is taken, reaching its maximum severity approximately 12 months to 18 months later.
Since 1938, several anticonvulsant agents have been introduced — including valproic acid, carbamazepine, phenobarbital and vigabatrin — in an attempt to overcome the adverse effects of phenytoin. Cases of gingival enlargement have been noted with these agents as well, but such reports are rare and poorly documented.
Due to its effectiveness in controlling convulsive seizure disorders, as well as its low cost and wide availability, phenytoin is still the drug of choice for treating epilepsy — particularly for grand mal, temporal lobe and psychomotor seizures. Many patients are reluctant to substitute it with a new class of anticonvulsants, making it imperative that oral health professionals recognize the increased risk and are prepared to address phenytoin-induced gingival enlargement in these patient populations.



CALCIUM CHANNEL BLOCKERS
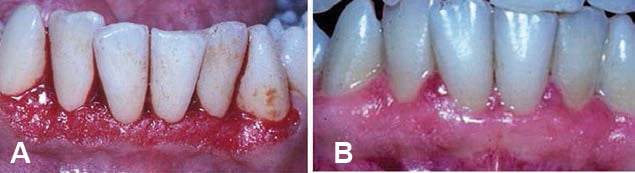
This class of drugs is widely used for managing hypertension, angina and supraventricular cardiac arrhythmias. These drugs derive their main therapeutic effects by preventing calcium ion influx through cell membranes. Not all CCBs affect the gingiva in the same way, however. Nifedipine is the most frequently implicated CCB in drug-induced gingival overgrowth (Figure 2 through Figure 4).4 Lederman et al were first to report its negative oral effects in 1984, and subsequent studies showed the prevalence of adverse effects varied from 14% to 83%.5–7
The prevalence of negative gingival effects is significantly lower with verapamil and amlodipine (4.2% and 3.3%, respectively).8,9 Numerous reports have also associated gingival enlargement with the new generation of CCBs, such as felodipine, nicardipine, manidipine and diltiazem.
IMMUNOSUPPRESSANTS
Immunosuppressants reduce the incidence and severity of allograft rejection following transplants of major organs (e.g., the liver, pancreas, heart or lung), as well as for managing autoimmune conditions, such as rheumatoid arthritis.
Since its discovery by Borel et al in 1977, cyclosporine A has become the most commonly prescribed drug for preventing organ rejection.10 It can exert serious side effects, unfortunately, including nephrotoxicity, induction of a diabetic state, chronic headaches and disfiguring gingival enlargement (Figure 5). The first publication of gingival overgrowth was reported in kidney transplant patients four weeks to six weeks following the initial dose.11 The enlargement was more pronounced on the labial aspect of the gingiva, and was associated with significant bleeding. When teeth were surgically extracted, however, the enlargement was permanently eliminated. The prevalence of cyclosporine A-associated gingival enlargement ranges from 8% to 81%, with children and adolescents at greatest risk.12,13
New immunosuppressant drugs, such as tacrolimus, mycophenolate mophetil and sirolimus, have provided alternative options for managing organ transplant patients without the risk of gingival overgrowth.14


CLINICAL FEATURES
While the oral manifestation of each type of drug-induced gingival enlargement is similar, it is not a diagnostic factor. Keeping a detailed patient medical history will help dental professionals achieve an accurate diagnosis. In their initial stages, lesions may appear as firm nodular enlargement of the interdental papillae, and may present throughout the oral cavity. Gingival overgrowth more commonly affects the anterior region, with greater pronouncement on facial/buccal surfaces than palatal/lingual surfaces.15 The enlargement can range from a mild increase of the interproximal gingival papillae to severe enlargement of both marginal and papillary tissues. In severe cases, the entire papillae and surrounding tissues are enlarged, giving the gingival tissues a lobulated appearance (Figure 6).
The enlargement may extend coronally and interfere with mastication and speech; in addition, in cases involving anterior teeth it can lead to esthetic issues. Overgrown tissue creates pockets that can harbor pathogenic microbes beyond the reach of a toothbrush or dental floss.
Though these drugs do not directly affect the underlying alveolar bone, the gingival enlargement may become superimposed among patients with preexisting periodontitis, or patients may acquire it concomitantly. Gingival enlargement can present with different forms, ranging from noninflamed, firm and fibrous gingiva to gingival tissue dominated by edema, erythema and bleeding.
DIFFERENTIAL DIAGNOSIS
Drug-induced gingival overgrowth lacks a distinctive clinical marker to aid oral health professionals in reaching an accurate diagnosis. These lesions mimic several pathologic conditions that manifest similarly. The enlargement may be localized or generalized. A localized gingival overgrowth may be caused by a periodontal abscess, fibroma or a pyogenic granuloma (tissue overgrowth caused by irritation, trauma or hormonal fluctuations, such as experienced during pregnancy). The local nature of these lesions — along with the clinical signs and symptoms, and patient medical and dental history — help to differentiate them from gingival enlargement caused by medication use.
Generalized gingival enlargement poses a difficult diagnostic challenge in some patients. The most common factor involved in the majority of gingival enlargement is oral biofilm, which should be treated as plaque-induced gingival overgrowth with scaling and root planing, coupled with good self-care. If the lesions persist three weeks to four weeks post-treatment, the patient should be referred to a medical provider to rule out systemic disease as a causative factor. Undiagnosed or poorly controlled diabetes is a major culprit, causing generalized inflammatory gingival enlargement and significant periodontal destruction.
Other systemic diseases that may cause gingival enlargement include acute leukemia, Wegener’s granulomatosis and scurvy. Rapid gingival overgrowth accompanied by bleeding may indicate the presence of acute myeoblastic leukemia, chronic myeloid leukemia, acute lymphocytic leukemia or chronic lymphocytic leukemia. Among patients diagnosed with acute myeloblastic leukemia, 5% experience gingival enlargement as the first complication.16,17 Leukemia is a malignant disease, and its successful resolution depends on early diagnosis and treatment. Oral health professionals should refer patients to a medical professional when rapid progression of overgrowth is noted.16,17
In Wegener’s granulomatosis, the gingiva appears swollen and bright red, with a granular surface described as “strawberry gums.” Differential diagnosis is suspected through this characteristic clinical manifestation, but it must be confirmed by biopsy. Scurvy, the result of vitamin C deficiency, is quite rare, but patients affected by this condition may experience severe gingival swelling and bleeding, accompanied by mobile teeth. Clinicians may rely on a high dosage of vitamin C and nonsurgical periodontal therapy to resolve gingival enlargement in this patient group.
In addition, generalized overgrowth may be due to a rare genetic condition called hereditary gingival fibromatosis, which is characterized by a progressive enlargement of the gingiva. These cases usually require surgical intervention to remove the excess fibrotic gingival tissue, but lesion recurrence is unpredictable. The fibrotic nature of these lesions, along with the patient’s medical and family history, can differentiate them from drug-induced gingival overgrowth.
ETIOLOGY AND RISK FACTORS
The pathogenesis of drug-induced gingival enlargement is not fully understood. It could be due to a reduction of collagen degradation by collagenase, or the outcome of overproduction of extracellular ground substance.18,19 Other possible pathways are the presence of a subset of gingival fibroblasts genetically susceptible to these medications.20 Johnson et al have reported the synergistic effect of proinflammatory cytokines (IL-1b and IL-6) in enhancement of collagen synthesis by human gingival fibroblasts as another possible factor involved in this enlargement.21
Biofilm is a common risk factor for all forms of inflammatory periodontal disease, and its presence exacerbates drug-induced gingival enlargement. Other risk factors may include gender, as men are three times more likely to develop gingival overgrowth than women.22 Age is inversely correlated with phenytoin- and cyclosporine A-induced gingival enlargement, as children and teenagers have a higher prevalence of these lesions than adults.23 In regard to dosage, there are conflicting reports of an association between the severity of enlargement and the daily intake of any of these drug classes. The majority of reports have failed to detect a significant relationship between drug dosage and the severity of gingival enlargement.18
TREATMENT
The most effective treatment for drug-induced gingival enlargement is withdrawing the offending drug. Medical providers may replace CCBs with beta blockers, diuretics or angiotensin-converting enzyme inhibitors, for example — none of which affect the oral tissues. Phenytoin may be replaced by carbamazepine, ethosuximide or sodium valproate.24 Cyclosporine A can be substituted with tacrolimus. Despite these options, physicians and patients are often reluctant to switch to a different regimen, especially when the disease is well controlled or other options have already been explored. If changing medications is not an option, some lesions may be managed nonsurgically. Mild lesions of CCB-induced gingival enlargement respond favorably to scaling and root planing and antimicrobial mouthrinses.
Good oral hygiene is pivotal in preventing further inflammation and maintaining positive results achieved with professional care, including periodic nonsurgical periodontal therapy. As for phenytoin-induced enlargement, the gingival response to scaling and root planing is not as favorable due to the high content of collagen in the lesions, which prevents significant tissue shrinkage.
Surgical excisions of the enlarged tissue by gingivectomy can eliminate the pseudo-pockets, restoring tissue architecture, appearance and function. This procedure is performed with blades, surgical knives, electrosurgical units or lasers (Figure 7). The recurrence of drug-induced gingival enlargement has been reported in cases treated with either surgical or nonsurgical methods — especially if cessation of the offending drug was only temporary or not an option in the first place. Recurrence can occur as early as three to six months following the intervention, and affects as many as 40% of patients.25 Recurrence is more common among those with poor oral hygiene or who lack access to professional care (Figure 8).
Drug-induced gingival enlargement is a common condition that can be caused by a variety of medications. These lesions lack distinguishable clinical markers from plaque-associated lesions, and may be difficult to diagnose. A detailed medical history will help guide clinicians regarding the etiology, diagnosis and treatment options for patients presenting with drug-induced gingival enlargement.
References
- Merritt HH, Putnam TJ. Landmark article Sept 17, 1938: Sodium diphenyl hydantoinate in the treatment of convulsive disorders. JAMA. 1984;251:1062–1067.
- Kimball OP. The treatment of epilepsy with sodium diphenylhydantoinate. JAMA. 1939;112:1244–1245.
- Casetta I, Granieri E, Desidera M, et al. Phenytoin-induced gingival overgrowth: A community-based cross-sectional study in Ferrara, Italy. Neuroepidemiology. 1997;16:296–303.
- Butler RT, Kalkwarf KL, Kaldahl WB. Drug-induced gingival hyperplasia: phenytoin, cyclosporin, and nifedipine. J Am Dent Assoc. 1987;114:56–60.
- Lederman D, Lumerman H, Reuben S, Freedman PD. Gingival hyperplasia associated with nifedipine therapy. Report of a case. Oral Surg Oral Med Oral Pathol. 1984;57:620–622.
- Barak S, Engelberg IS, Hiss J. Gingival hyperplasia caused by nifedipine. Histopathologic findings. J Periodontol. 1987;58:639–642.
- Fattore L, Stablein M, Bredfeldt G, Semla T, Moran M, Doherty-Greenberg JM. Gingival hyperplasia: a side effect of nifedipine and diltiazem. Spec Care Dentist. 1991;11:107–109.
- Miller CS, Damm DD. Incidence of verapamil-induced gingival hyperplasia in a dental population. J Periodontol. 1992;63:453–456.
- Jorgensen MG. Prevalence of amlodipine-related gingival hyperplasia. J Periodontol. 1997;68:676–678.
- Borel JF, Feurer C, Magnée C, Stähelin H. Effects of the new anti-lymphocytic peptide cyclosporin A in animals. Immunology. 1977;32:1017–1025.
- Rateitschak-Plüss EM, Hefti A, Lörtscher R, Thiel G. Initial observation that cyclosporin-A induces gingival enlargement in man. J Clin Periodontol. 1983;10:237–246.
- Friskopp J, Klintmalm G. Gingival enlargement. A comparison between cyclosporine and azathioprine treated renal allograft recipients. Swed Dent J. 1986;10:85–96.
- Pernu HE, Pernu LM, Huttunen KR, Nieminen PA, Knuuttila ML. Gingival overgrowth among renal transplant recipients related to immunosuppressive medication and possible local background factors. J Periodontol. 1992;63:548–553.
- Keown PA. New immunosuppressive strategies. Curr Opin Nephrol Hypertens. 1998;7:659–663.
- Marshall RI, Bartold PM. A clinical review of drug-induced gingival overgrowth. Aust Dent J. 1999;44:219–232.
- Demirer S, Ozdemir H, Sencan M, Marakoglu I. Gingival hyperplasia as an early diagnostic oral manifestation in acute monocytic leukemia: a case report. Eur J Dent. 2007;1:111–114.
- Wu J, Fantasia JE, Kaplan R. Oral manifestations of acute myelomonocytic leukemia: a case report and review of the classification of leukemias. J Periodontol. 2002;73:664–668.
- Barclay S, Thomason JM, Idle JR, Seymour RA. The incidence and severity of nifedipine-induced gingival overgrowth. J Clin Periodontol. 1992;19:311–314.
- Lucas RM, Howell LP, Wall BA. Nifedipine-induced gingival hyperplasia. A histochemical and ultrastructural study. J Periodontol. 1985;56:211–215.
- Pernu HE, Knuuttila MLE, Huttenen KRH, Tiilikainen ASK. Drug-induced gingival overgrowth and class I1 major histocompatibility antigens. Transplantation. 1994;57:1811–1813.
- Johnson RB, Zebrowski EJ, Dai X. Synergistic enhancement of collagenous protein synthesis by human gingival fibroblasts exposed to nifedipine and interleukin-1-beta in vitro. J Oral Pathol Med. 2000;29:8–12.
- Ellis JS, Seymour RA, Steele JG, Robertson P, Butler TJ, Thomason JM. Prevalence of gingival overgrowth induced by calcium channel blockers: a community based study. J Periodontol. 1999;70:63–67.
- Daley TD, Wysocki GP, Day C. Clinical and pharmacologic correlations in cyclosporine-induced gingival hyperplasia. Oral Surg Oral Med Oral Pathol. 1986;62:417–421.
- Seymour RA, Smith DG, Turnbull DN. The effect of phenytoin and sodium valproate on the periodontal health of adult epileptic patients. J Clin Periodontol. 1985;12:413–419.
- Ilgenli T, Atilla G, Baylas H. Effectiveness of periodontal therapy in patients with drug-induced gingival overgrowth. Long-term results. J Periodontol. 1999;70:967–972.

