
 GOKHANILGAZ/ISTOCK/GETTY IMAGES PLUS
GOKHANILGAZ/ISTOCK/GETTY IMAGES PLUS
Managing Xerostomia During Cancer Therapy
Implementing protective oral measures can help patients being treated for cancers of the head and neck maintain optimal oral health.
PURCHASE COURSE
This course was published in the August 2021 issue and expires August 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the August 2021 issue and expires August 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the prevalence of cancers of the oral cavity and pharynx.
- Discuss the effects of radiation on salivary gland function and the resulting impact on caries risk.
- Identify strategies for helping this patient population maintain optimal oral health.
Cancers of the oral cavity and pharynx are on the rise, with more than 50,000 cases diagnosed in the United States in 2020.1 While the prevalence of these cancers declined in the 1980s due to a decrease in tobacco and alcohol use, the rate of oral cavity and pharynx cancers began to rise in 1999.2 Between 2007 and 2016, oral and pharyngeal cancers increased by approximately 0.6% annually.2 This increase appears to be due to pharyngeal cancers linked to human papillomavirus (HPV) infections located at the base of the tongue, tonsils, soft palate, uvula or pharyngeal walls. Cancers linked to HPV have been increasing by 2.1% annually, whereas cancers unrelated to HPV have been decreasing by 0.4% annually.3
Cancerous lesions of the oral cavity not associated with HPV are typically located on the lip, floor of the mouth, hard palate or nasopharynx. The majority of these malignancies require intervention with surgery, radiotherapy, chemotherapy, or a combination of these approaches; however, each of these treatments can cause significant morbidity to the oral cavity. Given the increased incidence of oral and pharyngeal cancers, along with the detrimental oral health consequences of cancer therapy — notably xerostomia — dental professionals should be prepared to help these patients maintain their oral health.
Adequate salivary flow is paramount, as saliva’s role in health is multifactorial. It lubricates the mucosal membranes, promotes buffering and remineralization, and provides an antimicrobial effect. Yet patients who undergo head and neck radiotherapy often experience radiation-induced damage to the salivary glands.3,4 This is due to the proximity of the salivary glands to these head and neck tumors. In many cases, the radiation must pass through various salivary glands to effectively treat the tumor — and, in some cases, the tumor exists within the salivary gland itself. Salivary glands are extremely sensitive to even low doses of radiation, resulting in a reduction of salivary flow and alteration in its composition.4 The severity of salivary changes depends on the dose of radiation administered to the gland.5
RADIATION’S EFFECT ON SALIVARY GLAND FUNCTION
During radiation therapy, patients often experience a decrease in salivary production and an increase in viscosity.6 This may be temporary for some, while others may experience a permanent loss of salivary production as a result of radiation therapy. While exploring changes in the salivary gland function of patients with head and neck cancer after radiation therapy, Lin et al7 found a dramatic decrease in salivary flow during the first month following radiotherapy, with some recovery occurring between the third and sixth month posttreatment. However, pretreatment flow levels were not often fully achievable. Salivary flow and dental caries are closely related, as a decrease in flow and an increase in viscosity impair bacterial clearance from tooth surfaces, thus increasing caries susceptibility.8
Radiation therapy also affects the composition of saliva, reducing its buffering capacity. Saliva has a normal pH range of 6.5 to 7.5. Enamel is susceptible to demineralization when the pH of the oral cavity is 5.5 or below.3 With the limited amount of saliva, combined with decreased buffering capacity, the dentin and enamel are more easily demineralized.4 The influence of radiation therapy on the pH of the oral cavity may linger, with the pH beginning to increase back to normal levels approximately 12 months post-radiation therapy.7 Consequently, patients with head and neck cancer are prone to an increase in demineralization after radiotherapy, especially within the first year following treatment.
Reflective of the change in the pH of the oral cavity, acidogenic and cariogenic microorganisms also begin to flourish. From the onset of radiation therapy, more cariogenic bacteria, such as Streptococcus mutans, Lactobacillus and Candida, are identified in the oral cavity.4 The combination of decreased salivary flow, reduced oral pH, and increased cariogenic bacteria significantly impact this population’s caries risk.9

XEROSTOMIA-INDUCED CARIES
Xerostomia is defined as the sensation of dry mouth resulting from reduced or absent salivary flow. This condition can affect speech, taste, and ability to swallow, in addition to increasing the incidence of caries.4,10 Affecting a large percentage of patients previously treated for head and neck cancer, xerostomia negatively impacts quality of life.11–13
The severity of xerostomia depends on the cumulative dose of ionizing radiation to the major salivary glands (Figure 1).14 Reduction in salivary flow can be observed with ionizing radiation doses as low as 30 gray (Gy).5,15,16 Severe salivary dysfunction is observed at doses of 52 Gy or greater.13 Head and neck tumors are typically treated at doses of 60 to 70 Gy, which causes a rapid decline in salivary function. Xerostomia can be experienced as early as the first week of radiotherapy, with a 95% reduction in salivary flow experienced by the fifth week.12,13 As previously noted, salivary dysfunction may be temporary or permanent.11
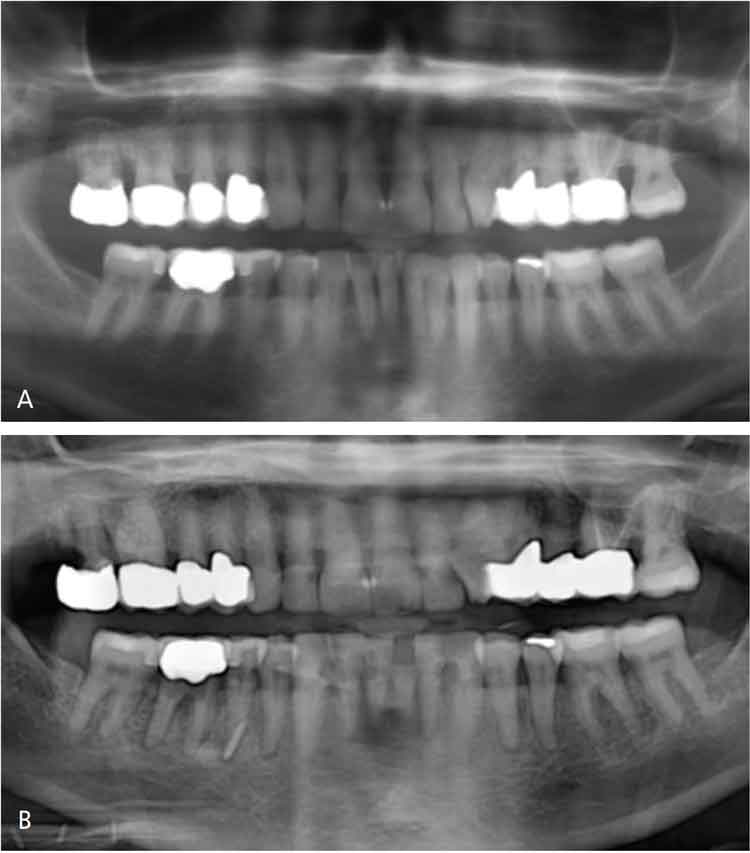
Radiation-induced caries can be extremely destructive and often progresses rapidly (Figures 2A and 2B). Clinically, radiation caries present in three patterns.4 The most common pattern affects the cervical aspect of the teeth, extends into the cementoenamel junction, and creates circumferential decay. The second pattern begins as demineralization of the tooth surface, which quickly progresses. While less common, the third pattern presents as a darkened color on the dentition. Ultimately, the goal of managing post-radiation caries is prevention.
ORAL HEALTH GUIDELINES
Due to the sequelae of head and neck radiation therapy, this patient population is at increased risk for oral complications and should be monitored closely. Given the impacts of radiation therapy, fluoride therapy may be indicated and fabrication of custom fluoride trays may be beneficial (Figure 3). In this case, the patient is instructed to apply prescription-strength (e.g., 5000 ppm) fluoride gel into the trays daily, following the manufacturer’s instructions for use.17
While the impacts from radiation-induced xerostomia can improve over time, these effects rarely resolve completely. As such, patients should continue to use their fluoride trays daily as long as xerostomia persists. In addition, these oral sequelae place this patient population in the high to extreme caries risk level, according to the caries management by risk assessment (i.e., CAMBRA) protocol. Therefore, fluoride varnish should be applied at each dental visit post-radiation therapy.9 In addition, oral health professionals can support patients’ self-care by recommending over-the-counter fluoride toothpaste and/or dentifrice with calcium phosphate in addition to fluoride. Not only does fluoride inhibit demineralization and promote remineralization, in high concentrations it also inhibits accumulation of oral biofilms.18
The extended dental team plays a key role in managing radiation-induced xerostomia, and can mitigate its effects by suggesting preventive strategies to reduce cariogenic activity, and identifying radiation caries or other early changes to tooth structure. Increasing the recall frequency to three months is suggested to monitor caries risk and lesion development.9,18 This interval is recommended until cariogenic activity is stabilized, after which a six-month interval is indicated.19 Depending on the individual’s caries risk assessment, capturing bitewing/periapical radiographs every six to 12 months may be advised.19 Routinely monitoring the oral cavity is an optimal preventive strategy for patients with head and neck cancer.

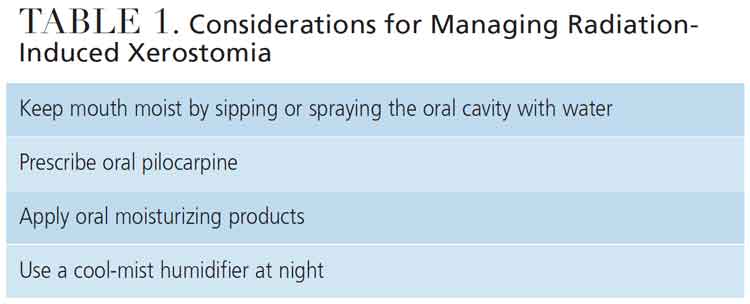
To assist patients in managing radiation-induced xerostomia, sugar-free gum, lozenges, and oral melts containing xylitol are recommended to stimulate salivary production and decrease the oral bacterial load (Table 1).13 Oral mucosal lubricants, sprays and mouthrinses are also available to moisten the oral cavity.6 If dry mouth symptoms cannot be effectively addressed with over-the-counter regimens, a prescription of pilocarpine or other cholinergic agonist may be helpful.6 If extreme xerostomia persists, a referral to a clinician with expertise in the management of salivary dysfunction may be warranted. Due to a reduction in salivary buffering capacity, patients may be advised to rinse with a solution of ½ teaspoon baking soda (and/or ¼ to ½ teaspoon of table salt) in 8 ounces of warm water several times daily.20 Frequent cleaning, lubrication and buffering of the oral cavity will help minimize the effects of radiation-induced xerostomia.
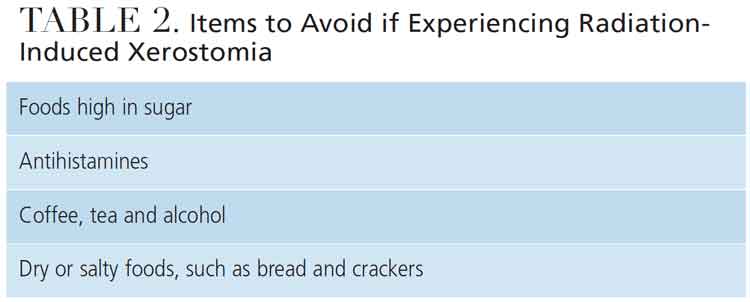
Diet may also influence cariogenic activity in patients with head and neck cancer, as xerostomia affects food preferences, appetite and dietary intake; in addition, xerostomia is a key factor associated with weight loss after radiation therapy.21 Patients are advised to eat small, high-calorie meals multiple times a day and constantly hydrate. Dental team members should suggest preventive strategies to reduce cariogenic activity, such as rinsing with water after eating and avoiding foods with high sugar content. In addition, due to the decrease in salivary function, dry or salty foods should be avoided (Table 2). Properly managing xerostomia may ultimately improve the nutritional status of this patient population.
CONCLUSIONS
In order to maintain optimal oral health in patients being treated for head and neck cancer, a collaborative, multidisciplinary approach is required before, during and after cancer treatment. Radiation therapy leads to changes in salivary quantity and quality, ultimately placing these patients at high risk for xerostomia-induced caries. Routine biofilm control, use of products to stimulate salivary flow or act as a saliva replacement, and daily use of prescription-strength fluoride gel can improve these patients’ overall quality of life.
REFERENCES
- American Cancer Society. Cancer Statistics Center. 2021 Estimates. Available at: cancerstatisticscenter.cancer.org/#!/. Accessed July 7, 2021.
- Ellington TD, Henley SJ, Senkomago V, et al. Trends in incidence of cancers of the oral cavity and pharynx — United States 2007–2016. MMWR Morb Mortal Wkly Rep. 2020;69:433–438.
- Deng J, Jackson L, Epstein JB, Migliorati CA, Murphy BA. Dental demineralization and caries in patients with head and neck cancer. Oral Oncol. 2015;51:824–831.
- Gupta N, Pal M, Rawat S, et al. Radiation-induced dental caries, prevention and treatment: a systematic review. Natl J Maxillofac Surg. 2015;6:160–166.
- Braam PM, Terhaard CH, Roesink JM, Raaijmakers CP. Intensity-modulated radiotherapy significantly reduces xerostomia compared with conventional radiotherapy. Int J Radiat Oncol Biol Phys. 2006;66:975–980.
- Shiboski CH, Hodgson TA, Ship JA, Schiødt M. Management of salivary hypofunction during and after radiotherapy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103(Suppl 66):e61–e79.
- Lin CY, Ju SS, Chia JS, Chang CH, Chang CW, Chen MH. Effects of radiotherapy on salivary gland function in patients with head and neck cancers. J Dent Sci. 2015;10:253–262.
- Dodds MW, Johnson DA, Yeh CK. Health benefits of saliva: a review. J Dent. 2005;33:223–233.
- Rechmann P, Kinsel R, Featherstone JD. Integrating caries management by risk assessment (CAMBRA) and prevention strategies into the contemporary dental practice. Compend Contin Educ Dent. 2018;39:226–233.
- Jawad H, Hodson NA, Nixon PJ. A review of dental treatment of head and neck cancer patients, before, during and after radiotherapy: part 1. Br Dent J. 2015;218:65–68.
- Nyathi M. Ionizing radiation side effects on salivary glands post external beam radiation therapy of head and neck tumors. J Biol Med Res. 2018;2:1–4.
- Cheng SC, Wu VW, Kwong DL, Ying MT. Assessment of post-radiotherapy salivary glands. Br J Radiol. 2011;84:393–402.
- Porter SR, Scully C, Hegarty AM. An update of the etiology and management of xerostomia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;97:28–46.
- Jensen SB, Pedersen AM, Vissink A, et al. A systematic review of salivary gland hypofunction and xerostomia induced by cancer therapies: prevalence, severity and impact on quality of life. Support Care Cancer. 2010;18:1039–1060.
- Pinna R, Campus G, Cumbo E, Mura I, Milia E. Xerostomia induced by radiotherapy: an overview of the physiopathology, clinical evidence, and management of the oral damage. Ther Clin Risk Manag. 2015;11:171–188.
- Wu VW, Leung KY. A review on the assessment of radiation induced salivary gland damage after radiotherapy. Front Oncol. 2019;9:1090.
- Epstein JB, Chin EA, Jacobson JJ, RishiraJ B, Le N. The relationships among fluoride, cariogenic oral flora, and salivary flow rate during radiation therapy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;86:286–292.
- Featherstone JD, Chaffee BW. The evidence for caries management by risk assessment (CAMBRA). Adv Dent Res. 2018;29:9–14.
- Noone J, Barclay C. Head and neck cancer patients — information for the general dental practitioner. Dent Update. 2017;44:209–210,213–215.
- Kawashita Y, Soutome S, Umeda M, Saito T. Oral management strategies for radiotherapy of head and neck cancer. Jpn Dent Sci Rev. 2020;56:62–67.
- Nuchit S, Lam-Ubol A, Paemuang W, et al. Alleviation of dry mouth by saliva substitutes improved swallowing ability and clinical nutritional status of post-radiotherapy head and neck cancer patients: a randomized controlled trial. Support Care Cancer. 2020;28:2817–2828.
From Decisions in Dentistry. August 2021;7(8)36-39.

