
 PEOPLEIMAGES / ISTOCK / GETTY IMAGES PLUS
PEOPLEIMAGES / ISTOCK / GETTY IMAGES PLUS
Managing Dental Anxiety With Advanced Behavioral Techniques
Using the principles of applied behavior analysis and functional behavior assessment can help allay patients’ dental anxiety, fear and dentophobia.
PURCHASE COURSE
This course was published in the May 2023 issue and expires May 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the May 2023 issue and expires May 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 153
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Explain the impacts of dental anxiety, fear and dentophobia, and the prevalence of these emotions in the U.S. patient population.
- Discuss behavioral tools for managing anxious dental patients, including applied behavior analysis, the modified dental anxiety scale, ABC contingencies, and functional behavior assessment.
- Describe how adopting behavior management techniques can create a comforting and patient-centered care environment.
Dental anxiety, fear and dentophobia (or odontophobia) can negatively impact the overall health of patients and prevent them from seeking and receiving dental treatment. The use of applied behavior analysis (ABA) principles in the dental setting can help create a comforting and patient-centered environment for care.1
The following educational and hypothetical vignette was developed from the experiences of various oral health professionals, including general dentists, providers specializing in geriatric dentistry, dental public health specialists, and public health-endorsed dental hygienists. This is intended as an example and provides a collection of learned experiences that reflect a common scenario.
Ann is a 55-year-old female with a history of dentophobia stemming from traumatic dental experiences when she was young. Ann contacted the dental office for an initial appointment with the complaint of “my teeth have been hurting for a while and I cannot sleep because of the horrible pain.” She also stated, “I cannot remember the last time I went to the dentist. I do not like going to the dentist and I am only here because I cannot get any sleep.” Upon clinical and radiographic examination, it was apparent that her chronic pain was due to multiple caries which have resulted in irreversible pulpitis and presence of an infection on her mandibular posterior molars. Ann did present with additional caries, but there was no evidence of an abscess or infection associated with these other lesions. When asked to rate her level of pain from one to 10, Ann said it was a nine or 10.
During the medical history review, the patient’s history of dental trauma was discussed. The next step was to find out what the possible triggers were for her fear and anxiety. After much discussion, it was determined that she was fearful of the local anesthetic; specifically, the site of the syringe and needle. Now that the trigger had been identified, the appropriate and corresponding technique for fear reduction could be discussed to help reduce her fear and anxiety. By addressing Ann’s concerns and comfort level before conducting the procedure, the clinician was able to build trust. More specifically, the dentist discussed the delivery of the anesthetic and how the procedures that would be used (administration technique and listening to her favorite music using headphones) would help create a more comforting treatment environment.
Ann did not want to proceed with treatment during the initial appointment, so a follow-up visit was scheduled early the next morning. Due to her overwhelming fear of the pending procedure, she was prescribed alprazolam (0.25 mg) to be taken in the office one hour prior to treatment so she could be monitored. As an added precaution, she was also asked to arrange for a ride home. Prior to the delivery of anesthetic, Ann was given a topical mouthrinse (dyclonine) and topical gel. The patient was encouraged to use her headphones to listen to music. After 10 minutes, she announced, “I am comfortable with you as my dentist, and I am ready to proceed.” The dentist waited another 15 minutes for profound anesthesia before initiating therapy. Ann tolerated the procedure well and scheduled her follow-up appointments.
BEHAVIORAL PRINCIPLES
In this vignette, the dental provider used some behavioral principles in the delivery of care, but without necessarily understanding the principles were founded in the science of ABA.1 For example, although it may be common practice, the distraction technique used during the administration of anesthesia and using headphones are examples of behavior strategies that involve changing the environment to make it more comfortable for the patient to receive treatment.1 Rescheduling the patient for a follow-up visit to initiate the dental treatment is an example of a pre-visit or desensitization technique. Desensitization is a step-by-step process to expose someone to something new or frightening until they become more comfortable in that situation. In ABA, this is sometimes referred to as a graduated exposure to stimuli.1
Asking the patient about triggers during the medical history interview is an example used in ABA to help identify any antecedents or precursors to the problem behavior — in this case, the fear of visiting the dentist. The one aspect in the vignette that could have been modified even more is the prescribing of alprazolam to reduce her anxiety. The implementation of behavior principles to reduce her fear could have been used as an alternative to prescribing medication. If medication is the only option, alternatives to alprazolam could be considered, depending on age and history. Such alternatives could include 0.5 mg lorazepam or a low dose of quetiapine (25 mg), as both can be effective in reducing anxiety. The dosing schedule was developed by shared experiences of the authors and dental colleagues. Once the patient is out of pain/discomfort, further integration of ABA principles can be used as part of a behavior plan to increase her cooperation in receiving treatment — and without the need for pharmaceuticals.
DISTINGUISHING BETWEEN DENTOPHOBIA AND FEAR OR ANXIETY
The educational vignette reveals that Ann has a history of dentophobia. While fear or anxiety of going to the dentist and dentophobia are terms that are used interchangeably at times, fear and phobia have distinctly different meanings and presentations in dental settings. People with anxiety or fear feel anxious when they think about going to the dentist. In comparison, dentophobia is an extreme fear that is out of proportion to the situation.2 Individuals with dentophobia avoid seeing the dentist, even when they are in pain.2 Past negative experiences, family history, traumatic history, or feeling a loss of control or embarrassment can lead to dentophobia.2 Possible triggers in a dental setting can include sound, smell, pressure, fear of anesthetic, shame, embarrassment, blood, noise, choking, feeling pain, and needles. Findings suggest that nearly 3% of men and almost 5% of women have dentophobia.2 This phobia is important to address because, similar to Ann’s case, a patient could delay treatment for an oral health condition that needs attention.
Severe fear or anxiety of dental treatment involves feelings of distress, but these feelings are not as extreme as dentophobia.2 Patients with dental anxiety worry about pain or stress at the dentist, but will likely still visit the office for treatment — unlike those with dentophobia.2 About 36% of the U.S. population has a fear of dental treatment, with 12% having an extreme fear.3 Dental anxiety has also been shown to negatively impact quality of life. Low oral health-related quality of life has been associated with high dental anxiety.4,5
According to a recent poll by the American Dental Association’s Health Policy Institute, more than 70% of dentists surveyed reported an increase in the prevalence of patients experiencing teeth grinding and clenching (i.e, bruxism), conditions often associated with stress — up from just under 60% in 2020.6 In addition, the survey revealed that 63% of dentists noted an increase in chipped and/or cracked teeth, while 62% of respondents saw a rise in temporomandibular disorder symptoms, which include headaches and jaw pain.6 These poll findings highlight the added stress and anxiety brought on by the COVID-19 pandemic and other stressors.
Dental anxiety and dentophobia can further impact a patient’s overall health, as the anxiety and fear become deterrents to receiving the necessary care; this hesitancy can eventually affect their social environment, as well as their work and school performance. Delaying or avoiding dental care can also lead to more costly treatment later due to the extent of disease. Patients with dentophobia or dental anxiety may be more likely to present with problem behaviors that can include crying, screaming, running away, not opening their mouth, or even vocalizing their fear to the dental team. The problem behavior(s) may arise when the patient is directly exposed to the fear of the dental office itself or a possible trigger within the dental environment. One of the central tenets of the ABA approach to dental anxiety is the opportunity to modify the environment as the first step in changing behavior.7
The literature supports the description of a “vicious cycle” of dental fear, dental anxiety and avoidance of treatment.8,9 The possible confounding of oral health and fear level is one manifestation of the cycle that has a higher risk of neglected health concerns, wherein neglect leads to increased health concerns that render avoidance more likely.10 The concept of a vicious cycle of dental anxiety was proposed by Berggren8 in 1984; it suggests that dental fear and dental anxiety lead to avoidance of oral healthcare — and a subsequent neglect of oral health.
TOOLS TO MANAGE DENTAL ANXIETY
In the vignette, the patient was hesitant about receiving dental treatment because of her dentophobia. The extreme pain that kept Ann up at night was the trigger or antecedent to have her schedule a dental appointment.
The modified dental anxiety scale (MDAS) is an example of implementing an indirect measure in a dental setting. The findings from patients with high MDAS scores can assist providers in determining the best course of action to help the individual reduce his or her fear and anxiety.11,12 The dentist in the vignette used questions from the MDAS to assess the patient’s current state of well-being. The MDAS consists of five questions and uses a Likert scale, with possible responses including: not anxious, slightly anxious, fairly anxious, very anxious, and extremely anxious. A response of “not anxious” receives a score of 1, “slightly anxious” is noted as 2, “fairly anxious” is rated as 3, “very anxious” earns a 4, and “extremely anxious” receives a 5.11,12
The total score for the MDAS is a sum of all five questions, ranging from 5 to 25. A cutoff of 19 or above indicates high dental anxiety and a score of 11 to 18 indicates moderate-to-high anxiety.11,12 According to Humphris et al,11,12 the MDAS has an empirically devised cutoff point where scores above a certain level indicate the possibility of dentophobia, rather than dental anxiety, as follows: 5 to 9 = not dentally anxious, 10 to 18 = fairly dentally anxious, and 19 to 25 = very dentally anxious/dentally phobic.
According to White et al,13 anxiety assessments, such as the MDAS, are an easy and reliable way to assess dental anxiety so that care can be more effective and patient-centered. Being aware of the MDAS and the patient’s anxiety level may help the dental team establish a trusting rapport, and thus encourage routine care that will help the individual achieve and maintain optimal oral health.13 An effective approach to conducting the assessment in a systematic manner is to embed the MDAS within an electronic health record. When the assessment yields a score indicating the patient is afraid or anxious, the dental team can begin to look at less aversive approaches to care that will alleviate these concerns.
CONCEPT OF APPLIED BEHAVIOR ANALYSIS
In clinical use, ABA is a scientific approach to understanding and improving behavior through manipulations to environmental contingencies. A contingency is something that immediately follows a behavior.14 Indirect data (similar to the MDAS) are collected to better understand the behaviors; however, direct observations are relied upon to make more confident changes to the contingencies. These contingencies are sometimes referred to as the ABCs.14 These contingencies of the environment investigate the behavior (which is the B) in context of the antecedents (A: what happens before the behavior) and the consequences (C: what happens immediately after the behavior).14 The contingencies are then controlled through the ABA principles of reinforcement, punishment and extinction.
According to Cooper et al,14 reinforcement is defined as a response-consequence relationship in which a response (e.g., the correct answer) is followed immediately by a consequence (e.g., verbal praise). This immediate consequence will result in similar responses occurring more often.14 In the dental setting, this refers to offering a reinforcer (e.g., verbal praise or a break from treatment) to increase the likelihood the positive behavior will occur in the future. It is important to note that a reinforcer or reinforcement needs to occur immediately after the desired or appropriate behavior.14 If this is not possible, then a verbal reason for receiving the reinforcer should be provided.
For example, if a patient gets to choose a prize out of the reward chest, he or she would be told this is because the patient sat still and opened wide when requested. Punishment is defined as a response-consequence relationship in which a response (e.g., the patient is talking) is followed immediately by a consequence (e.g., tap on the chin to open the mouth) that decreases future occurrences of that behavior.14
Similar to punishment, extinction can also be used to limit patient behavior. Before using extinction, it is important to know what the reinforcement might be. An example in the dental setting would be a patient who continues to whine or cry. It appears the crying and whining behaviors are due to the provider constantly reinforcing the behavior by paying some type of attention. In this case, the reinforcement is increasing an unwanted behavior. So, when systematically using extinction, the provider would ignore the behavior until the crying eventually subsides. Extinction occurs when a response no longer produces access to a reinforcement.14
Examining behavior within the context of these three contingencies — and further generalized by the ABA principles presented by Fisher et al1 and Cooper et al14 — can help providers better understand the patients’ behavior and how the behavior is impacted by the dental environment. The goal of ABA therapy is to decrease the occurrence of a behavior that may potentially be harmful or perhaps interfere with treatment.1,14 In the dental profession, research provides sufficient evidence that a behavioral approach to resistance to dental treatment can be effective in reducing the patient’s physical resistance during care, thus allowing therapy to be completed.7
CREATE A COMFORTABLE ENVIRONMENT
In combination with desensitization techniques, a behavioral approach can be used to create a more comfortable environment for the patient, which, in turn, increases the likelihood of cooperation during future treatment.7 The implementation of pre-visits to a dental office (without any treatment) can help patients better understand what to expect from the first dental visit.1 In addition, sharing pamphlets, brochures or videos that describe the dental office, supplies and procedures can help create a more comforting environment for the patient. Applying behavior principles within a dental setting may be an extra step in the daily routine, but it could save time during future appointments if patients are more cooperative and can receive the scheduled care. These behavior process tools can strengthen the patient-provider relationship and develop the foundations of a patient-centered environment.
A systematic and consistent approach to applying ABA principles in the dental setting involves conducting a functional behavior assessment (FBA). The FBA is a systematic method of obtaining information about the purpose or function of a problem behavior.14 The indirect and direct findings from the FBA help providers structure an intervention to mitigate the problem behavior and encourage more appropriate or cooperative behavior. By conducting an FBA, clinicians can develop objective, patient-centered goals to improve health outcomes using accepted behavior principles, such as reinforcement, punishment or extinction.
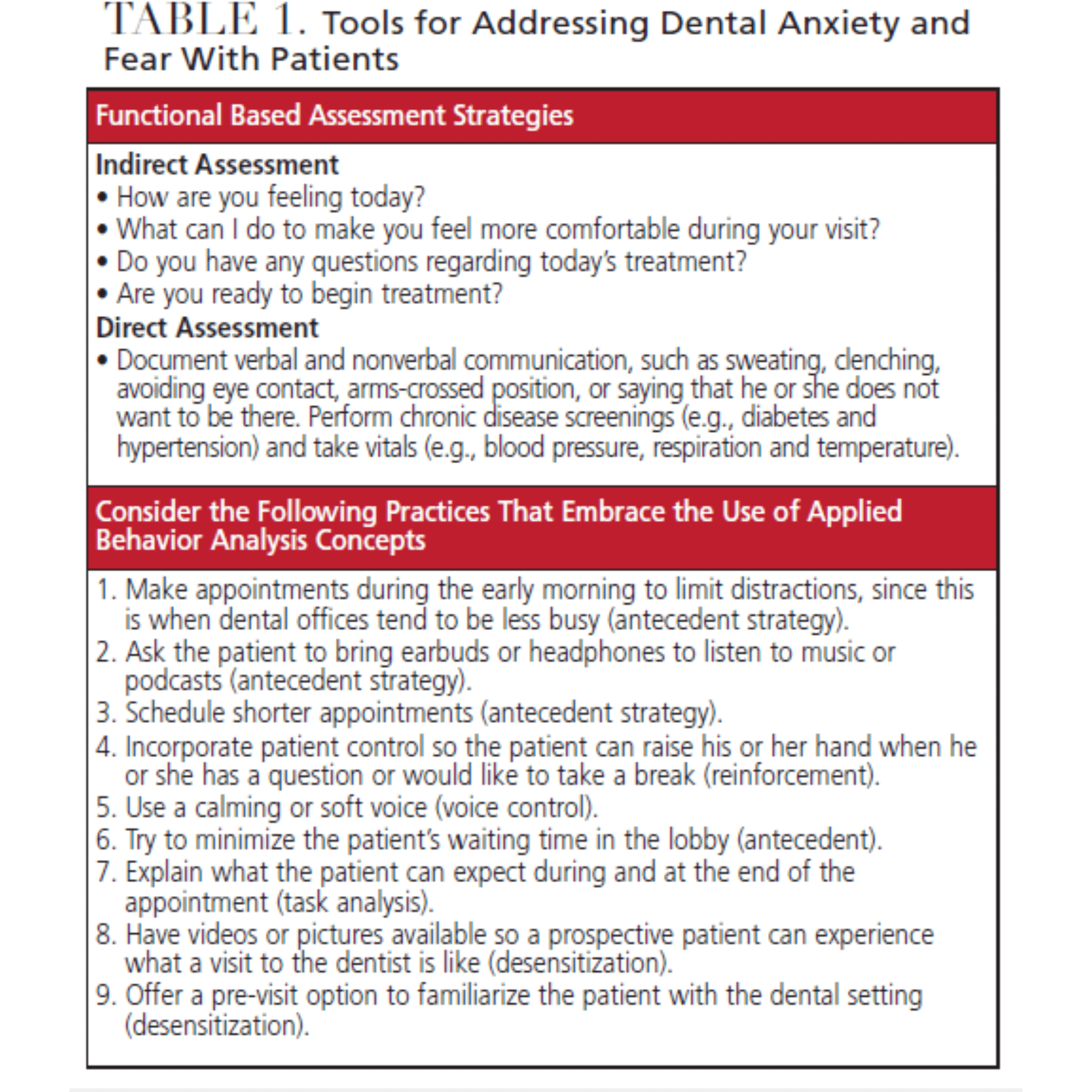
As evidenced by the educational vignette, the use of ABA principles or behavior strategies can be incorporated in a dental setting with just a few tips, as outlined in Table 1. These suggestions were drafted based on the shared experiences of the authors and adapted from Cooper et al.14
CONCLUSION
Dental anxiety, fear and dentophobia can negatively impact a patient’s overall health and create a barrier to accessing dental care, which can further exacerbate the patient’s oral health status. By applying ABA principles and thinking in terms of the ABC contingencies, providers can create a comforting, empathetic, and patient-centered environment for individuals who display some level of fear or anxiety. Similar strategies can also be used to create a welcoming environment for children and adults with special healthcare needs, as well as patients in general who wish to establish a dental home with a trusting team. Adopting a systematic and consistent approach to assessment using FBA and related strategies can help create patient-centered goals that support improved health outcomes.
REFERENCES
- Fisher WW, Piazza CC, Roane HS. Handbook of Applied Behavior Analysis. 2nd ed. New York: The Guilford Press; 2021.
- Cleveland Clinic. Dentophobia (Fear of Dentists). Available here. Accessed April 14, 2023.
- Hill KB, Chadwick B, Freeman R, O’Sullivan I, Murray JJ. Adult Dental Health Survey 2009: relationships between dental attendance patterns, oral health behaviour and the current barriers to dental care. Br Dent J. 2013;214:25–32.
- McGrath C, Bedi R. Measuring the impact of oral health on quality of life in Britain: using OHQoL-UK(W). J Public Health Dent. 2003;63:73–77.
- McGrath C, Bedi R. The association between dental anxiety and oral health-related quality of life in Britain. Community Dent Oral Epidemiol. 2004;32:67–72.
- American Dental Association. Health Policy Institute poll: Dentists see increased prevalence of stress-related oral health conditions. Available at: https://www.ada.org/publications/ada-news/떕/march/hpi-poll-dentists-see-increased-prevalence-of-stress-related-oral-health-conditions. Accessed April 14, 2023.
- Kemp F. Alternatives: A review of non-pharmacologic approaches to increasing the cooperation of patients with special needs to inherently unpleasant dental procedures. Behav Anal Today. 2005;6:88–108.
- Berggren U. Dental fear and avoidance: a study of etiology, consequences and treatment. Thesis. Goteborg, Sweden: Goteborg University; 1984.
- DeJongh A, Schutjes M, Aartman IHA: A test of Berggren’s model of dental fear and anxiety. Eur J Oral Sci. 2011;119:361–365.
- Klepac RK, Dowling J, Hauge G. Characteristics of clients seeking therapy for the reduction of dental avoidance: reactions to pain. J Behav Ther Exp Psychiatry. 1982;13:293–300.
- Humphris GM, Dyer TA, Robinson PG. The modified dental anxiety scale: UK general public population norms in 2008 with further psychometrics and effects of age. BMC Oral Health. 2009;9:20.
- Humphris G, Crawford JR, Hill K, Gilbert A, Freeman R. UK population norms for the modified dental anxiety scale with percentile calculator: adult dental health survey 2009 results. BMC Oral Health. 2013;13:29.
- White AM, Giblin L, Boyd LD. The prevalence of dental anxiety in dental practice settings. J Dent Hyg. 2017;91:30–34.
- Cooper JO, Heron TE, Heward WL. Applied Behavior Analysis. 3rd ed. Upper Saddle River, NJ: Pearson Education, Inc; 2020.
From Decisions in Dentistry. May 2023;9(5):26-29.

