

Management of Peg-Shaped Maxillary Lateral Incisors and Congenitally Missing Mandibular Lateral Incisors
This clinical presentation can pose challenges with respect to function and esthetics. Here is an evidence-based approach to treatment.
This clinical presentation can pose challenges with respect to function and esthetics. Here is an evidence-based approach to treatment
The ultimate goal of evidence-based dentistry (EBD) is to provide optimal care by integrating three important aspects of practice: the clinician’s expertise, patient’s needs and preferences, and the best available scientific evidence.1 It is important to realize that EBD is not solely determined by scientific evidence; this must be evenly balanced with the clinician’s experience and preferred clinical approach, and the patient’s preferences. The American Dental Association (ADA) is a proponent of EBD, and published a series of articles that provides an overview of the basic concepts of EBD to assist oral health professionals in using evidence to inform clinical decision-making.1 Although clinicians embrace the concept, the daily use of EBD in treatment decision-making is not without challenges. Kao2 examined potential barriers that clinicians encounter in their attempts to incorporate EBD. The main concern noted in Kao’s paper was the overflow of information that makes it difficult for clinicians to stay up to date with the ever-increasing knowledge base.
This clinical report describes the steps for evidence-based decision-making for treatment of a patient who presented with peg-shaped maxillary lateral incisors and congenitally missing mandibular lateral incisors. Special emphasis is placed on how to perform a quick and efficient search of the literature in order to support EBD. When seeking filtered information about a clinical question, systematic reviews are preferred and offer a quick way to evaluate the evidence. Searching for best evidence can be facilitated by formulating a sound question that can be answered through a literature search. PICO is often used to describe the four elements of a good clinical question; in this acronym, P stands for population, I for intervention, C for comparison, and O for outcome.


CASE REPORT
Patient JW was a healthy 21-year-old female. She presented to the operative dentistry clinic with a chief complaint that “I don’t like my small top teeth and the spaces in my bottom teeth.” She was referred from the orthodontic clinic after spacing closure between teeth #21/#22 and #27/#28. During orthodontic planning and treatment, she was informed about the need for additional restorative treatment after debanding. The final alignment of the two peg-shaped maxillary lateral incisors was finalized so unnecessary tooth reduction could be prevented. The patient had high esthetic expectations with regard to the final appearance of her smile. JW’s medical history was unnoteworthy and the dental history included general dental prophylaxis, a few restorations on anterior teeth, and completion of orthodontic treatment with clear retainers. The consulting prosthodontist did not recommend placing implants due to limited spaces on the patient’s lower missing teeth. Preoperative frontal and occlusal views are shown in Figures 1 through Figure 4.


PHASE I: DIAGNOSIS AND TREATMENT PLANNING
During the initial visit, preparations were made to provide detailed information about various treatment options. The diagnostic phase included:
- A comprehensive examination and caries risk assessment
- Anterior periapicals, bite-wing films
- Extraoral and intraoral photographs
- Upper and lower arch alginate impressions
- Digital smile analysis
- Diagnostic wax-up on a study cast based on the digital smile analysis
- Mock-up restorations to present the proposed final restoration and obtain the patient’s consent to continue to the treatment phase
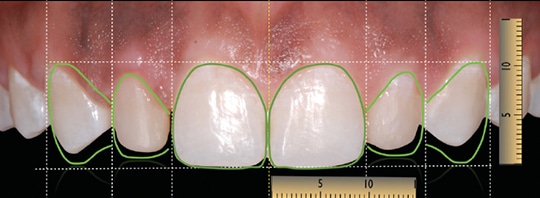

The prevalence of peg-shaped maxillary permanent lateral incisors has been reported to be 1.8% to 2.3%, while the prevalence of missing permanent mandibular lateral incisors is less frequent (0.1%).3,4 However, if they occur together, they can pose challenges in clinical dentistry with respect to function and esthetics. During the consultation visit, the smile analysis, diagnostic wax-ups and mock-up restoration were utilized to help JW visualize the final outcome (Figure 5 and Figure 6). The following treatment options, as well as the advantages of a conservative treatment approach, were explained:
- Tooth whitening
- Direct resin composite versus porcelain laminate veneers on peg-shaped laterals
- Resin-bonded fixed dental prostheses (RBFDPs), using either one or two retainers
- Implants, fixed dental prostheses and removable prostheses
The use of direct resin-based composites and indirect porcelain laminate veneers are well-established procedures for the treatment of peg-shaped and discolored teeth. However, the treatment team was unsure whether the longevity would be the same for these two treatment options. Thus, a search was planned for the best evidence on the comparative longevity of these therapies. Regarding the treatment of the lower space, the prosthodontist had already ruled out the placement of implants. Therefore, the team recommended the use of RBFDPs, which is a conservative alternative to implants in cases of insufficient bone or other anatomical, medical or economical limitations.5 Optimal design is an important factor in the success of RBFDPs, so the team wished to explore whether the number of retainers would influence the longevity of the restoration. To address these questions, two PICO queries were formulated.
PICO 1. In a young adult patient, what is the longevity of direct resin-based composites compared to porcelain laminate veneers?
PICO 2. When restoring lower mandibular anterior teeth, what is the longevity of a one retainer, fixed bonded cantilever bridge compared to a two retainer bonded restoration?
A quick and easy place to find the latest evidence is the ADA Center for Evidence-Based Dentistry website,6 which provides clinical practice guidelines, critical summaries, plain language summaries and systematic reviews. The treatment team searched within the ADA Center for Evidence-Based Dentistry website under the topic index of esthetic dentistry and found one systematic review evaluating the longevity of direct versus indirect veneer restorations for intrinsic dental stains. Based on the review by Wakiaga et al,7 there was no reliable evidence to show the benefit of one type of veneer restoration (direct or indirect) over the other with regard to longevity.
A search on the second PICO question did not yield any relevant information on the ADA website, therefore, the PubMed database was used. Many times, database searches can be frustrating in that there are too many publications, and narrowing it down to a few articles is time consuming. The use of Boolean operators can help maximize search efficiency. On PubMed, the search was limited to “review articles,” with the following search terms: “resin-bonded fixed dental prostheses AND design AND anterior AND two retainer.” The use of AND combines only sets that contain both terms and effectively reduces the number of search results. NOT excludes sets that contain the term and is often used to narrow the search. The team’s search yielded a systematic review and meta-analysis on the “Clinical performance of anterior resin-bonded fixed dental prostheses with different framework designs,” by Wei et al.8 Within the limitations of the review, the authors concluded that cantilever RBFDPs demonstrate lower clinical failure than two-retainer RBFDPs in the anterior region.8
Based on the description of the scientific evidence and visual aids, including the diagnostic wax-up and mock-up, JW chose to start the treatment with at-home whitening to lighten her teeth, and proceed with direct resin composites on her peg-laterals and two fixed bonded cantilever restorations on her lower teeth.
PHASE II: TREATMENT STAGE
Tooth Whitening: Over a three-week period, a professionally dispensed, patient administered at-home whitening kit with custom fabricated trays and 10% carbamide peroxide whitening agent was used to whiten the teeth from a baseline shade of A1 to a final shade of B1. The incorporation of tooth whitening to anterior composite or ceramic restorations is essential in maximizing the esthetic outcome of a the final smile. The use of 10% carbamide peroxide has been reported to be a safe and effective treatment by the ADA Council of Scientific Affairs.9 However, it is important to pace the next treatment to allow sufficient time (generally two to six weeks) for the color to stabilize and prevent inadvertent reductions in bond strength.10,11
Direct Resin-Based Composite Restorations: Preservation of healthy tooth structure is the main advantage of the use of direct resin-based composites for the treatment of peg-shaped teeth.12 The diagnostic wax-up was used to fabricate a lingual matrix from polyvinyl siloxane. This matrix facilitated the polychromatic layering technique with nanofilled, resin-based composite to mimic the natural tooth’s characteristics.
All-Ceramic, Resin-Bonded Fixed Dental Prostheses: The acid-etch technique introduced in 1955 opened the door for minimally invasive dentistry, and RBFDPs based on this technique were first proposed in the early 1970s. The preparation design and framework type have evolved thanks to improvements in restorative materials and adhesive systems. In the 1990s, all-ceramic RBFDPs were introduced and these delivered superior and more predictable bonding to the tooth structure for the anterior esthetic region.13 The systematic review published by Wei et al,8 as well as other investigators, documented that the two-retainer all-ceramic RBFDPs presented a higher incidence of unilateral framework failure due to fracture than the cantilevered RBFDPs.13,14 Survival of RBFDPs was mainly determined by abutment tooth preparation design, mechanical properties of the restoration material, and the quality of the adhesive bond.8


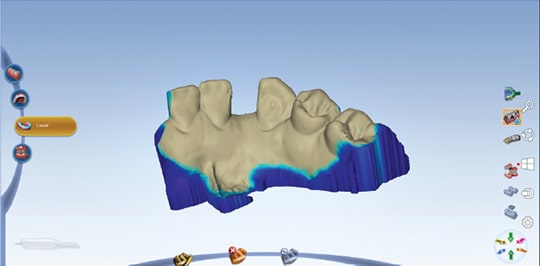
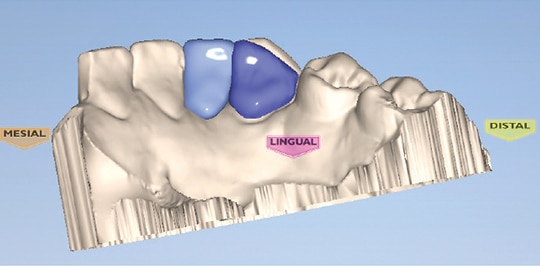
In light of these findings, the patient’s final preparation of tooth abutments (#23 and #26) followed a unilateral cantilevered concept. The margin consisted of a 0.5 mm light chamfer finish line in the enamel. Additionally, a flat area on the mesial surface of the abutment teeth was created with tapered, cylindrical diamond bur to establish a path of insertion and stabilize the prostheses during try-in and bonding. An intraoral scanner was utilized for digital impressions. Digital equipment and tools in the digital design center created the digital wax-up of the proposed restorations. A lithium disilicate glass ceramic block was used in the milling machine (Figure 7 through Figure 10). After try-in, further adjustments were made, and the prostheses in blue phase were stained to mimic the tooth characteristics. Final cementation was performed with rubber dam isolation with an adhesive resin cement.


PHASE III: MAINTENANCE
The patient was satisfied with the treatment outcome and motivated to maintain her new smile (Figure 11 through Figure 14). She received new orthodontic retainers and newly fabricated whitening trays for touch-up whitening, if needed. Optimal maintenance of oral hygiene and restorations was confirmed at the 6-month and 1-year recall examinations.


CONCLUSION
The process of searching for best evidence can be enhanced by formulating a PICO question that can be answered through a literature search. The compilation and interpretation of the resulting evidence aids clinical treatment decision-making, and could justify the use of contemporary adhesive techniques and cantilever RBFDPs involving computer aided design and computer aided manufacturing, as demonstrated by the case management process outlined here.
As noted at the outset, the goal of EBD is to provide optimal patient care, and, toward this end, becoming faster and more proficient in literature searches will not only aid clinical efficiency, it also promises to help improve long-term outcomes.
KEY TAKEAWAYS
- This clinical report describes the steps for evidence-based decision-making when treating a patient who presented with peg-shaped maxillary lateral incisors and congenitally missing mandibular lateral incisors.
- Evidence-based dentistry is not solely determined by scientific evidence; it must be evenly balanced with the clinician’s experience and preferred clinical approach, as well as patient preferences.
- The overflow of information makes it difficult for clinicians to stay up to date with the ever-increasing knowledge base.
- Searching for best evidence can be facilitated by formulating a sound PICO question (see text) that can be answered through a literature search.
- The use of Boolean operators can also help maximize search efficiency.
- The use of direct resin-based composites and indirect porcelain laminate veneers are well-established procedures for the treatment of peg-shaped and discolored teeth. However, the treatment team was unsure whether the longevity would be the same for these two treatment options.
- Consequently, a search was planned for the best evidence on the comparative longevity of these options.
- Becoming faster and more proficient in literature searches will not only aid clinical efficiency, it also promises to help improve long-term outcomes.
REFERENCES
- Brignardello-Petersen R, Carrasco-Labra A, Glick M, Guyatt GH, Azarpazhooh A. A practical approach to evidence-based dentistry: understanding and applying the principles of EBD. J Am Dent Assoc. 2014;145:1105–1107.
- Kao RT. The challenges of transferring evidence-based dentistry into practice. J Evid Based Dent Pract. 2006;6:125–128.
- Hua F, He H, Ngan P, Bouzid W. Prevalence of peg-shaped maxillary permanent lateral incisors: A meta-analysis. Am J Orthod Dentofacial Orthop. 2013;144:97–109.
- Rakhshan V. Meta-analysis of observational studies on the most commonly missing permanent dentition (excluding the third molars) in non-syndromic dental patients or randomly-selected subjects, and the factors affecting the observed rates. J Clin Pediatr Dent. 2015;39:199–207.
- Kern M, Sasse M. Ten-year survival of anterior all-ceramic resin-bonded fixed dental prostheses. J Adhes Dent. 2011;13:407–410.
- American Dental Association Center for Evidence-Based Dentistry. About EBD. Available at: ebd.ada.org/en/about. Accessed September 15, 2017.
- Wakiaga J, Brunton P, Silikas N, Glenny AM. Direct versus indirect veneer restorations for intrinsic dental stains. Cochrane Database Syst Rev. 2004;1:CD004347.
- Wei YR, Wang XD, Zhang Q, et al. Clinical performance of anterior resin-bonded fixed dental prostheses with different framework designs: A systematic review and meta-analysis. J Dent. 2016;47:1–7.
- American Dental Association Council of Scientific Affairs. Tooth Whitening/Bleaching: Treatment Considerations for Dentists and Their Patients. Available at: ada.org/~/media/ ADA/About%20the%20ADA/Files/ada_house_of_delegates_whitening_report.ashx. Accessed September 15, 2017.
- Haywood VB. Tooth Whitening: Indications and Outcomes of Nightguard Vital Bleaching. Hanover Park, Ill: Quintessence Publishing Co; 2007.
- Al Shethri S, Matis BA, Cochran MA, Zekonis R, Stropes M. A clinical evaluation of two in-office bleaching products. Oper Dent. 2003;28:488–495.
- Ferracane JL. Resin composite — state of the art. Dent Mater. 2011;27:29–38.
- Piemjai M, Ozcan M, Garcia-Godoy F, Nakabayashi N. A 10-year clinical evaluation of resin-bonded fixed dental prostheses on non-prepared teeth. Eur J Prosthodont Restor Dent. 2016;24:63–70.
- Stylianou A, Liu PR, O’Neal SJ, Essig ME. Restoring congenitally missing maxillary lateral incisors using zirconia-based resin bonded prostheses. J Esthet Restor Dent. 2016;28:8–17.
The authors have no commercial conflicts of interest to disclose.
Featured image by LORADO/E+/GETTY IMAGES PLUS
From Decisions in Dentistry. October 2017;3(10):26–30.
