

Improving Access to Care for Patients With Autism Spectrum Disorder
This patient population needs support in receiving much-needed dental care that requires a multifactorial approach.
PURCHASE COURSE
This course was published in the March 2024 issue and expires March 2027. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
Characterized by the Diagnostic and Statistical Manual of Mental Disorders, 5th ed (DSM-V), as the presence of impairments with communication, social interactions, and restricted and repetitive interests, autism spectrum disorder (ASD) is a lifelong neurodevelopment disorder. 1–9
This course was published in the March 2024 issue and expires March 2027. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 750
Educational Objectives
After reading this course, the participant should be able to:
- Define autism spectrum disorder (ASD).
- Identify perceived barriers to dental care for those with autism, their caregivers, and their dental team.
- Discuss ways to overcome barriers to care for the ASD population.
According to a 2019 study, one in 59 individuals is diagnosed with ASD, with males diagnosed four times more frequently than females.2,3 There is no known etiology, though various research has indicated a relationship to genetics, the environment, or a combination of both.3,9
Diagnostic criteria
The diagnostic criteria for ASD use gradation of severity and, therefore, the diagnosis may present differently in each individual. The DSM-V outlines the gradation of severity in three levels:8,9
- Level 1: requires support
- Level 2: requires substantial support
- Level 3: requires very substantial support
This article will focus on individuals at level 2
Profile of Patients With Autism Spectrum Disorder
Individuals on the autism spectrum share many characteristics that make professional oral care a higher priority compared to their neurotypical counterparts. Habits, such as teeth grinding, cheek biting, and gingival pricking (fingernail scraping of the gingiva), are common self-injurious behaviors among individuals with ASD.1
Individuals with ASD also experience generalized impairment of fine motor skills. Research shows that many children on the autism spectrum also experience a dyspraxia, a developmental coordination disorder. Dyspraxia decreases the ability to manipulate tools, such as floss and/or a toothbrush, which significantly impacts the effectiveness of an oral hygiene regimen.11
Many medications used to treat the symptoms of ASD cause side effects such as xerostomia, dysgeusia, gingivitis, hyperplasia, stomatitis, dysphagia, and bruxism.10 These conditions, combined with poor manual dexterity and behaviors typical of individuals with ASD, may increase this population’s susceptibility to oral diseases.
Patients with ASD find comfort in consistency and repetition of routine; even a slight disruption to their routine may cause disorientation and distress. Often these disruptions are followed by what others perceive as challenging and uncooperative behaviors.7
To ensure the success of dental appointments among patients with ASD, oral health professionals need to understand the underlying cause of their distress in order to prevent further escalation.
Standard dental clinics are frequently overstimulating to those on the autism spectrum. Sensory triggers, such as strong odors, bright lights, loud noises, and close proximity to others, may lead to a reaction that is perceived as challenging or negative by dental staff and families. The reactions may include screaming, crying, pushing, and/or biting themselves or others.1,3-5,7 Among individuals with ASD, 50% are nonverbal, and these extreme responses may be their way of expressing fear, stress, and anxiety in an environment in which they feel they have little to no control.1
Accommodating Sensory Deficits
While some individuals with ASD experience hypersensitivity to certain stimuli, others may experience hyposensitivity. Hyposensitive individuals may be less aware of internal experiences of discomfort or pain.12 As such, they may not be aware of the presence of a carious lesion or an oral infection.
This may be due to differences in pain receptors and/or perception of their experiences. Some studies challenge the idea that those on the autism spectrum may have a higher threshold for pain.12 Those in the hyposensitive category do, in fact, feel pain, however their expression of it differs from that of neurotypical individuals.12 Indeed, self-injurious behaviors could be a direct manifestation of a pain response.
To accommodate sensory deficits, the dental team and caregivers should communicate about the patient’s sensory preferences and aversions prior to the appointment. Visual pedagogy is an effective tool used to familiarize patients with dental tools and materials prior to their appointment.13 Viewing photos or videos of a dental setting in advance may help to ease feelings of anxiety and uncertainty.
During the appointment, the use of a weighted blanket/lead apron, noise cancelling headphones, and/or dimming the lights may also aid in making the patient feel calmer and more comfortable.5,13
The use of a papoose board is a sensory adaptation technique that may be used in some dental facilities. A protective stabilization device, a papoose board is used to immobilize patients with special needs as a way to prevent injury to themselves and/or healthcare providers during dental procedures. While controversial, papoose boards may provide deep-touch pressure, which has been shown to induce a sense of calm and comfort during an otherwise stressful event.14
Finding the Right Dental Team
Among the special healthcare needs populations, unmet dental needs ranked the highest compared to other healthcare categories.15–17 Moreover, children on the autism spectrum were shown to be two times less likely to have their healthcare needs met than typical children.6
Despite the demand for affordable and adequate dental care, many parents/caregivers of individuals on the autism spectrum experience difficulty finding a dental facility that will treat their children.3,4,6,7,16 At the same time, healthcare workers report a lack of training and feelings of unpreparedness in treating and communicating with patients on the spectrum.5,16,17
Dental facilities often lack the necessary training, time, staff, and environment needed to treat patients with ASD. A review of the literature shows a general lack of training within dental programs in regards to treating this population.18
Lai et al17 found that 50.8% of dental students had no experience in caring for special-needs populations and 60% did not have the confidence needed to treat patients with ASD. Additionally, in a survey of dental programs across the United States, researchers discovered 50% of dental students received less than 5 hours of instruction on how to care for patients with special needs.18,19
To minimize these barriers, dental programs may consider revising their curricula to include courses on how to care for and treat various special-needs populations. These courses should require a certain amount of clinic and rotation hours spent treating patients who are differently abled. This would afford dental and dental hygiene students the opportunity to develop a deeper understanding of the needs of patients with ASD, while enhancing the confidence required to treat them effectively. Private practices may consider holding monthly training and continuing education courses for staff.
Within both the dental school and private practice setting, the implementation of stimulus fading may be an effective solution for patients averse to dental settings. Stimulus fading involves the gradual exposure of an individual to a stimulus that causes a fear response.20
When individuals exhibit a positive response, they are rewarded. Stimulus fading may include exposing the individual to dental materials and/or tools in increments. Increased exposure, proximity, and duration to a stimulus over time has been shown to garner positive responses in patients with autism.20
Finally, the addition of one or two treatment rooms dedicated to the care of those with sensory integration difficulties may also help create a less overstimulating environment and facilitate a more positive experience.
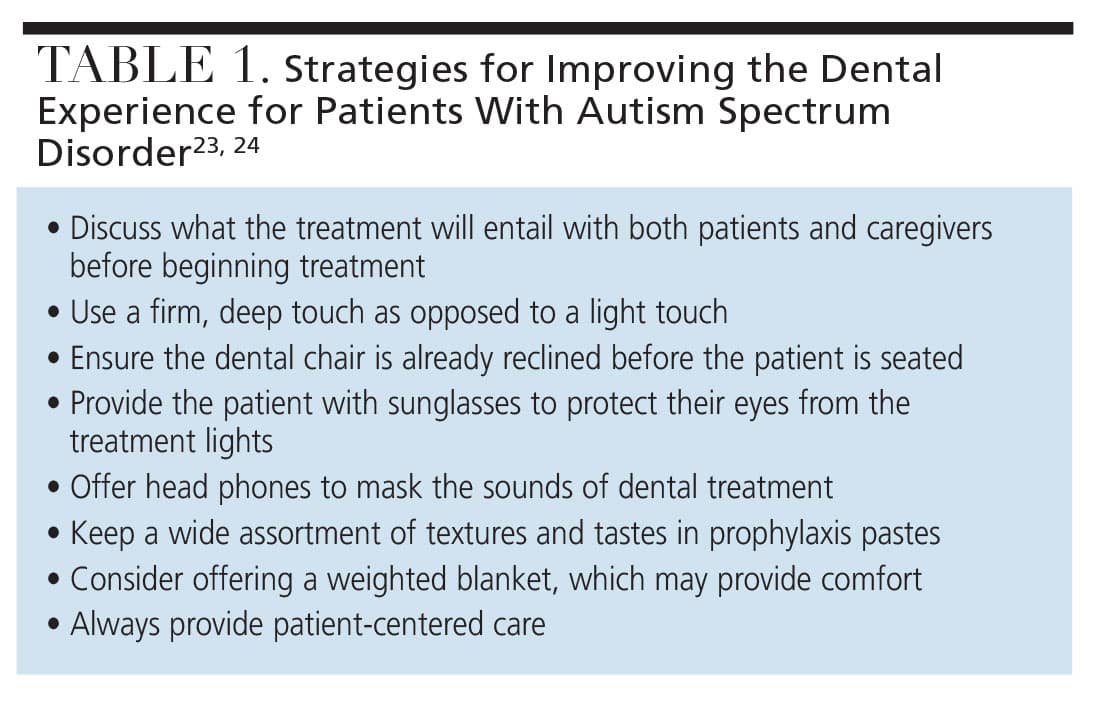 Sensory adapted dental environments, such as the Snoezelan environment, have a calming effect on not only the patient, but also on the caregiver and the dental provider.21 The Snoezelan environment uses dim lighting, sound, and deep-pressure touch to elicit a calm response. Studies have shown a marked decrease in maladaptive behaviors and dental anxiety when using these techniques in a sensory adapted environment.21,22 Table 1 includes additional strategies to ensure successful dental experiences.23,24
Sensory adapted dental environments, such as the Snoezelan environment, have a calming effect on not only the patient, but also on the caregiver and the dental provider.21 The Snoezelan environment uses dim lighting, sound, and deep-pressure touch to elicit a calm response. Studies have shown a marked decrease in maladaptive behaviors and dental anxiety when using these techniques in a sensory adapted environment.21,22 Table 1 includes additional strategies to ensure successful dental experiences.23,24
Importance of Caregivers
Raising and caring for persons with ASD can be an overwhelming experience for parents/caregivers and family members. This is often exacerbated by the high cost of medical care and contradicting information concerning therapeutic treatments for people on the autism spectrum. This is also true when it comes to dental treatment.
Many parents/caregivers have expressed concerns about perceived toxins thought to be found in dental materials such as fluoride, mercury, and gluten.2 Despite a lack of scientific evidence, some parents/caregivers insist certain dental materials adversely affect their child with ASD.10
These concerns often derive from information exchanged through social media forums and parental support groups. Because of this, the use of complementary and alternative medicine (CAM) has become more prominent, though its efficacy has not been well documented.10 Most CAM treatments include supplements, such as vitamins, omega 3, and probiotics, intended to help manage ASD symptoms.
With so much misinformation, it has become a challenge for parents/caregivers to identify which treatments are beneficial for the child with ASD from those that may be harmful. This can hinder the dental professional’s ability to administer quality preventive care.
If a parent/caregiver has questions or concerns regarding dental treatments or therapies used, oral health professionals need to approach these encounters with empathy and without judgment. Additionally, dental providers should listen to parent/caregiver concerns and offer evidence-based responses.
To increase knowledge of safe dental practice for patients with ASD, dental clinics or local dental schools should consider hosting educational sessions where parents and caregivers are presented with the most current research regarding the care of individuals with ASD. These session could also be held virtually, so those with limited access to transportation are still able to attend.
Parents/caregivers frequently object to the use of preventive dental materials and may request the use of alternative treatments. In the event a parent/caregiver declines the use of fluoride, the oral health professional may consider recommending more frequent preventive visits.10 This provides the opportunity to continuously evaluate the patient’s progress with self-care. It will also allow the patient to become more familiar with the dental setting and may prevent challenging behaviors in the future.
Dental facilities may consider offering fluoride-free dentifrices, such as those with hydroxyapatite, to parents/caregivers who still refuse fluoride after education. By offering fluoride-free options, oral health professionals continue to build rapport with parents/caregivers and demonstrate that the care of their child is a priority.
Conclusion
ASD is a multifaceted condition that requires a multifaceted approach to care. With no known etiology and a rapidly changing understanding of ASD, it can be difficult for dental providers and parents/caregivers to provide the best care. Autism is not a one-size-fits-all condition.
Oral health professionals need to have an in-depth knowledge of their patient with ASD in order to provide comfortable treatment and optimize care.1 This can be achieved in part through detailed documentation at each visit, as well as continuous and clear communication between the parent/caregiver and dental provider.
The barriers to care experienced by those with ASD are not separate entities, but rather a small fraction of intertwining obstacles that fall under the larger umbrella of “access to care.”
When brainstorming for solutions, dental providers should consider other barriers faced by individuals with ASD and their parents/caregivers, such as financial capabilities, access to transportation, and social support. Oral healthcare should not be a privilege for select populations, but rather a right for every individual, regardless of the differences and disadvantages he or she may face.
References
- Chandrashekhar SS, Bommangoudar J. Management of autistic patients in dental office: a clinical update. InJ J Clin Pediatr Dent. 2018;11:219–227.
- Trudeau MS, Madden RF, Parnell JA, Gibbard WB, Shearer J. Dietary and supplement-based complementary and alternative medicine use in pediatric autism spectrum disorder. Nutrients. 2019;11:1783.
- Alshihri AA, Al-Askar MH, Aldossary MS. Barriers to professional dental care among children with autism spectrum disorder. J Autism Dev Disord. 2021;51:2988–2994.
- AlHumaid J, Gaffar B, AlYousef Y, Alshuraim F, Alhareky M, El Tantawi M. Oral health of children with autism: the influence of parental attitudes and willingness in providing care. ScientificWorldJournal. 2020;2020:8329426.
- Bultas MW, McMillin SE, Zand DH. Reducing barriers to care in the office-based health care setting for children with autism. J Pediatr Health Care. 2016;30:5–14.
- Taneja N, Litt MD. Caregivers’ barriers to dental care for children with autism spectrum disorder. J Dent Child (Chic). 2020;87:98–102.
- Loo CY, Graham RM, Hughes CV. Behaviour guidance in dental treatment of patients with autism spectrum disorder. Int J Paediatr Dent. 2009;19:390–398.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, Virginia: American Psychiatric Publishing; 2013:947.
- Masi A, DeMayo MM, Glozier N, Guastella AJ. An overview of autism spectrum disorder, heterogeneity and treatment options. Neurosci Bull. 2017;33:183–193.
- Rada RE. Controversial issues in treating the dental patient with autism. J Am Dent Assoc. 2010;141:947–953.
- Kaur M, M Srinivasan S, N Bhat A. Comparing motor performance, praxis, coordination, and interpersonal synchrony between children with and without autism spectrum disorder (ASD). Res Dev Disabil. 2018;72:79–95.
- Ko HG, Oh SB, Zhuo M, Kaang BK. Reduced acute nociception and chronic pain in Shank/-/- mice. Mol Pain. 2016;12:1744806916647056.
- Balian A, Cirio S, Salerno C, Wolf TG, Campus G, Cagetti MG. Is visual pedagogy effective in improving cooperation towards oral hygiene and dental care in children with autism spectrum disorder? A systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18:789.
- Ismail N, Isa KAM, Wan Mokhtar I. A randomised crossover trial of behaviour guidance techniques on children with special health care needs during dental treatment: the physiological variations. Children (Basel). 2022;9:1526.
- Waldman HB, Perlman SP, Rader R. Hardships of raising children with special health care needs (a commentary). Soc Work Health Care. 2010;49:618–629.
- Nelson LP, Getzin A, Graham D, et al. Unmet dental needs and barriers to care for children with significant special health care needs. Pediatr Dent. 2011;33:29–36.
- Lai B, Milano M, Roberts MW, Hooper SR. Unmet dental needs and barriers to dental care among children with autism spectrum disorders. J Autism Dev Disord. 2012;42:1294–1303.
- Ocanto R, Levi-Minzi MA, Chung J, Sheehan T, Padilla O, Brimlow D. The development and implementation of a training program for pediatric dentistry residents working with patients diagnosed with ASD in a special needs dental clinic. J Dent Educ. 2020;84:397–408.
- Romer M, Dougherty N, Amores-Lafleur E. Predoctoral education in special care dentistry: paving the way to better access? ASDC J Dent Child. 1999;66:132–185.
- Shabani DB, Fisher WW. Stimulus fading and differential reinforcement for the treatment of needle phobia in a youth with autism. J Appl Behav Anal. 2006;39:449–452.
- Shapiro M, Melmed RN, Sgan-Cohen HD, Eli I, Parush S. Behavioural and physiological effect of dental environment sensory adaptation on children’s dental anxiety. Eur J Oral Sci. 2007;115:479–483.
- Cermak SA, Stein Duker LI, Williams ME, Dawson ME, Lane CJ, Polido JC. Sensory adapted dental environments to enhance oral care for children with autism spectrum disorders: a randomized controlled pilot study. J Autism Dev Disord. 2015;45:2876–2888.
- Laurence SS, Melvin L, Bruhn AM. Improve the oral health of patients with autism spectrum disorder. Dimensions of Dental Hygiene. 2022;20(2):35-38.
- Burgette JM, Rezaie A. Association between autism spectrum disorder and caregiver reported dental caries in children. JDR Clin Trans Res. 2020;5:254–261.
From Decisions in Dentistry. March 2024; 10(2):42-45

