

Effective and Efficient Asepsis Protocols
Every practice should follow a stringent infection prevention plan to minimize risk of transmission among patients and providers.
Every practice should follow a stringent infection prevention plan to minimize risk of transmission among patients and providers
Following best practices in infection prevention reduces the risk of transmission of pathogenic microorganisms and is integral to maintaining patient and clinician health and safety. While rare, incidents of bloodborne pathogen (BBP) exposure and/or transmission have been reported in dental settings, such as portable clinics and oral surgery and dental offices.1–3 In addition, the transmission of Legionella pneumophila via contaminated dental unit waterlines (DUWL) led to the death of an octogenarian from Legionnaire’s disease.4 More recently, Mycobacterium abscessus — a fast-growing pathogen present in water, soil and dust — was transmitted to children undergoing pulpotomies in dental clinics in California and Georgia.5 In these cases, contaminated DUWLs were the source. Typically, transmission occurs through the use of contaminated equipment during invasive procedures or inoculations involving contaminated products.6 The exposure resulted in children contracting soft and hard tissue infections that required invasive surgery and intravenous antibiotic therapy.5 The growing global threat posed by antibiotic resistance further emphasizes the importance of disease prevention. Antibiotic resistance has been observed in many microorganisms found in the dental setting, such as M. abscessus, Pseudomonas aeruginosa and Staphylococcus aureus.7–10 In addition, of the three most concerning BBPs in the dental setting — hepatitis B (HBV), hepatitis C and human immunodeficiency virus (HIV) — only HBV can be prevented through inoculation. Furthermore, 10% of patients newly diagnosed with HIV are infected with an antiretroviral-resistant strain.11
Best practices for the dental setting are detailed in the U.S. Centers for Disease Control and Prevention’s (CDC) Guidelines for Infection Control in Dental Health-Care Settings — 2003.12 The CDC also offers a plain-language synopsis of best practices and checklists in its Summary of Infection Prevention Practices in Dental Settings: Basic Expectations for Safe Care.13 In addition, the Occupational Safety and Health Administration (OSHA) established mandatory standards to help promote worker health and safety. The BBP Standard is particularly relevant to infection prevention in the dental setting, while the Hazard Communication Standard is relevant when using chemical agents as infection control products.14 Twenty-six states and two territories have their own OSHA-approved plans, which must be at least as stringent as OSHA requirements.
STRATEGIES FOR COMPLIANCE
Investigations have found that infection control breaches were caused by a failure to properly reprocess instruments; lack of awareness, education and training; and unsafe injection practices. These findings resulted in recommendations to improve awareness and use of standard precautions. Other causes of infection control breaches may include human error, complacency, and, rarely, a disregard for safety. Recommended strategies to promote compliance include education and training, designating an office infection control coordinator, using engineering and work controls, and keeping team member’s immunizations up to date.12,13,15,16 Under OSHA’s BBP Standard, employers must offer the HBV vaccination at no cost to individuals at risk of BBP exposure within 10 days of hire. In one study, however, 15% of offices did not offer HBV vaccination.17 For individuals who decline the HBV immunization, a signed and dated declination form must be retained in the personnel records.14 Offices and other dental facilities should have a written immunization policy.12 The increased availability of single-use devices, streamlined processes and digital technology also helps dental professionals and staff meet requirements.
EDUCATION AND TRAINING
Compliance with asepsis guidelines improves when training is provided. In one study, taking more than six hours of continuing education (CE) on infection prevention significantly improved compliance.18 Additionally, a higher percentage of participating oral health professionals reported compliance with surveyed practices when working in states with mandated infection prevention requirements and when they had recently completed CE classes on the topic.19 Multimodal education has been found to be more effective than more limited methods.16
The CDC guidelines recommend designating an infection control coordinator, and by 2012, approximately 80% of offices responding to a national survey reported complying with this recommendation.16 Coordinators must have the appropriate knowledge base and training. They are responsible for reviewing policies and procedures; developing written policies; managing the exposure control plan; monitoring compliance; identifying unsafe practices; noting areas for improvement; arranging or providing training; fostering a culture of safety; maintaining all relevant documents; and ensuring that disposables, equipment and devices required for infection prevention are available.20,21
ENGINEERING AND WORK CONTROLS
Engineering controls must be employed, and prospective options reviewed at least annually.14 Examples include needle recapping devices, disposable single-use syringes, computerized injection systems, and self-sheathing anesthetic needles.22 In addition, the use of sharps containers in each operatory/work area eliminates the need to transport used sharps to instrument reprocessing areas.
Using instrument cassettes, ultrasonic cleaning units, instrument washers and washer/disinfectors also reduces the risk of injury. Perforated, closed cassettes eliminate the need to handle contaminated instruments during cleaning. Inspection after cleaning is still necessary, however, and if instruments are visibly contaminated, further cleaning is warranted. Compared with manual cleaning, automated cleaning is safer and more effective.12 Instrument washers use detergents, while instrument washer/disinfectors (Figure 1) substantially reduce the bacterial load through thermal disinfection and the use of proprietary formulations containing detergents and chemical additives.

Work practice controls may also reduce the risk of sharps exposure. Examples include using cheek retractors instead of fingers, avoiding transferring a syringe with the needle unsheathed or pointing toward another individual, and avoiding reaching over sharp objects.
CHECKLISTS AND OBSERVATIONS
The CDC summary document contains policy and practice checklists that can be used to evaluate compliance, thus allowing corrective action, if needed.13 The observational checklists are particularly useful when assessing compliance with repeatable infection prevention protocols and to determine areas and methods for improvement. Observations include performance of individual tasks, such as hand hygiene (Table 1), donning and wearing personal protective equipment (PPE), and treatment of environmental surfaces.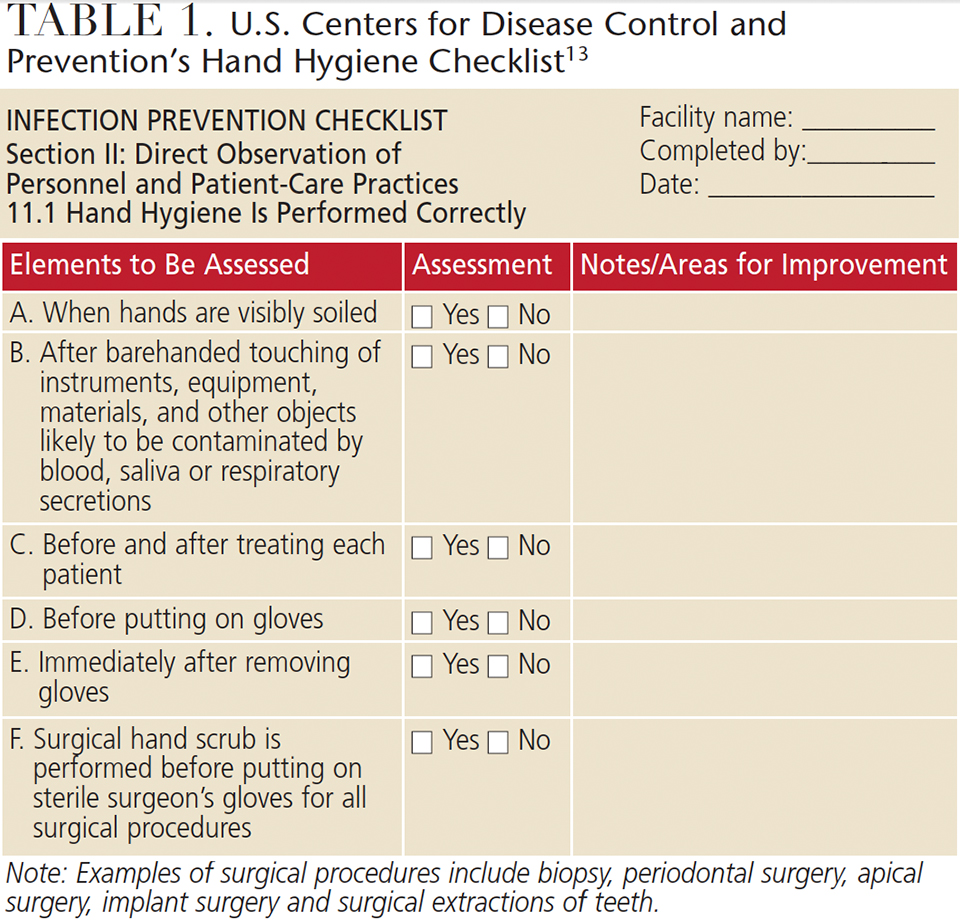
Other observations can be made that may indicate further assessment is needed. For instance, if soap is lasting substantially longer than anticipated, this may mean that handrubs are being used more often, but it may also indicate that compliance with hand washing is poor. Checklists also function as reminders of critical steps and as tools for task verification. Printed and digital versions of the checklists are available at cdc.gov/oralhealth/infectioncontrol/index.html. The CDC DentalCheck app is designed to help dental practices maintain compliance with infection prevention guidelines.23,24 Practices may consider conducting a self-audit (with or without the assistance of a consultant) to identify areas that do not meet accepted guidelines.
Offices can simplify their asepsis efforts by reducing clutter and employing single-use disposables and barrier protection for computers, tablets and, where permissible, complex devices. Cleaning and disinfection of clinical contact surfaces can also be simplified by using a hospital-level cleaner/disinfectant that both cleans and disinfects. This reduces inventory requirements and potentially reduces the risk of error. From an efficiency perspective, selecting produces with a fast kill time for microorganisms can decrease operatory turnaround time. In instrument reprocessing, a workflow from the zone receiving contaminated instruments to the clean zone with sterile instrument packs also simplifies infection prevention, especially if these zones are visually indicated, such as by using red to signify the contaminated zone and blue to identify the clean zone (Figure 2).

A further consideration for effective asepsis includes the selection of instruments and devices. After cleaning, and in accordance with the Spaulding Classification (i.e., the classification of instruments by their risk of transmitting microorganisms and disease), critical instruments and devices — as well as semicritical heat-resistant instruments, devices and handpieces — are to be heat sterilized.12 In contrast, semicritical heat-sensitive instruments or devices (except handpieces) are reprocessed by immersion in a high-level disinfectant/sterilant. Noncritical items are treated using U.S. Environmental Protection Agency (EPA)-registered disinfectants. An intermediate-level disinfectant must be used if visible blood is present, but if no visible blood is present, a low-level disinfectant may be utilized.12 When determining which instrument or device to purchase, consider the reprocessing instructions and whether it is compatible with the reprocessing requirements based on the Spaulding Classification. Another consideration is the complexity of a device (e.g., whether it must be disassembled prior to reprocessing, and if individual parts need to be reprocessed differently).
Products regulated by the U.S. Food and Drug Administration (FDA) include high-level disinfectant/sterilants and sterilization pouches, ultrasonic cleaners, instrument washers, washer/disinfectors and autoclaves.25 These medical devices have undergone review by the FDA, as have the manufacturers’ instructions for use (unlike products that are similar but not bona fide medical devices). For example, a dishwasher has not been assessed for safety and efficacy for use as infection control equipment in the dental setting. Using a dishwasher does not represent the standard of care, and has been shown to be ineffective for instrument cleaning.26 Instrument washer/disinfectors, in contrast, are highly effective.27 Similarly, the EPA regulates hospital-level (low- and intermediate-level) disinfectants.
Infection prevention products must be readily available and accessible, and team members’ personal preferences should be considered. One potential issue is frequent hand washing, which can irritate hands — particularly if they are not dried properly — thus affecting compliance. When hands are not visibly soiled, using 60% to 95% alcohol-based handrubs for routine hand hygiene may aid compliance, as they are less drying on hands than soap and water.28 In addition, soaps and alcohol-based handrubs containing emollients can increase hand hygiene compliance by helping to maintain epidermal water content and improve skin health.29 Barrier creams may also be helpful.
Staff compliance may be an issue with PPE, which includes clinical attire, surgical face masks (or respirator for transmission-based precautions),30 protective eyewear, single-use medical or sterile surgical gloves for patient care, and utility gloves for operatory cleanup and instrument reprocessing. The American Society for Testing and Materials (ASTM) has standards for rating masks based on bacterial and particulate filtration efficacy, fluid resistance, breathability and flame resistance. Using an ASTM-rated mask ensures the wearer knows its level of protection, which is not the case with unrated masks. While ASTM 3-rated surgical face masks provide the highest level of protection, these masks are also typically thicker and less breathable than ASTM 1- or ASTM 2-rated masks; thus, they are generally used in situations in which greater protection is needed. Compliance may improve if the mask is comfortable, soft and breathable. Research on wearing N95 respirators shows that discomfort, heat buildup and low breathability negatively impact compliance.31
Glove fit and comfort affect compliance, and gloves should be available in several sizes. Right- and left-handed gloves may be more comfortable than ambidextrous gloves. In addition, OSHA requires that an employer ensure that hypoallergenic gloves or glove liners (or something similar) are available for workers. This encourages glove use by individuals with allergies or sensitivity to glove materials.
In light of the fact that PPE is worn throughout the day, comfort and preference are important considerations. Displaying a chart with images of the recommended sequence of donning and doffing PPE in the operatory and instrument reprocessing area will remind team members of the proper protocol and thereby aid compliance.
ENSURING COMPLIANCE
In addition to the CDC checklists and DentalCheck app, a variety of digital tools is available to aid compliance. These include (but are not limited to) phone and tablet apps, interactive website support from product manufacturers, prescheduled collection of regulated waste and inventory replenishment, cell phone-generated reminders to perform key tasks (e.g., spore testing), and digital archiving of autoclave cycles and automated instrument cleaning. Measurement tools are available to assess a practice’s safety culture,32 including the National Institute for Occupational Safety and Health Survey (available at cdc.gov/niosh/stopsticks/survey.html).33
Ultimately, effective infection prevention in the dental setting requires all team members to follow accepted guidelines and regulations. Competency and compliance with asepsis protocols benefit patients, oral health professionals and society at large.
KEY TAKEAWAYS
- Following best practices in infection prevention is integral to maintaining patient and practitioner health and safety.
- The growing global threat posed by antibiotic resistance further underscores the importance of disease prevention.
- Best practices for the dental setting are detailed in the U.S. Centers for Disease Control and Prevention’s (CDC) Guidelines for Infection Control in Dental Health-Care Settings — 2003.12
- The CDC also offer a plain-language synopsis of best practices and checklists: Summary of Infection Prevention Practices in Dental Settings: Basic Expectations for Safe Care.13
- Strategies to promote compliance include education and training, designating an office infection control coordinator, using engineering and work controls, and keeping team members’ immunizations up to date.12,13,15,16
REFERENCES
- Radcliffe RA, Bixler D, Moorman A, Cleveland JL. Hepatitis B virus transmissions associated with a portable dental clinic, West Virginia, 2009. J Am Dent Assoc. 2013;144:1110–1118.
- Oklahoma Department of Health. Dental Healthcare-Associated Transmission of Hepatitis C. Final Report of Public Health Investigation and Response, 2013. Available at: ok.gov/health2/documents/Dental%20Healthcare_Final%20Report_2_17_15.pdf. Accessed August 30, 2017.
- Urciuoli A. Burlington dental patients told to get tested for hepatitis and HIV. Available at: globalnews.ca/news/3544446/burlington-dental-patients-told-to-get-tested-for-hepatitis-and-hiv/. Accessed August 30, 2017.
- Ricci ML, Fontana S, Pinci F. Pneumonia associated with a dental unit waterline. Lancet. 2012;379:684.
- American Dental Association. Nontuberculosis mycobacterial infection linked to pulpotomy procedures and possible dental waterline contamination reported in California and Georgia. September 21, 2016. Available at: ada.org/en/science-research/science-in-the-news/nontuberculosis-mycobacterial-infection-linked-to-pulpotomy-procedures. Accessed August 30, 2017.
- U.S. Centers for Disease Control and Prevention. Healthcare-associated Infections. Mycobacterium abscessus in Healthcare Settings. Available at: cdc.gov/hai/organisms/mycobacterium.html. Accessed August 30, 2017.
- Nessar R, Cambau E, Reyrat JM, Murray A, Gicquel B. Mycobacterium abscessus: a new antibiotic nightmare. J Antimicrob Chemother. 2012;67:810–818.
- U.S. Centers for Disease Control and Prevention. Healthcare-Associated Infections. Multidrug-Resistant Tuberculosis. Available at: cdc.gov/tb/publications/factsheets/drtb/mdrtb.htm. Accessed August 30, 2017.
- U.S. Centers for Disease Control and Prevention. Healthcare-Associated Infections. Pseudomonas aeruginosa in Healthcare Settings. Available at: cdc.gov/hai/organisms/pseudomonas.htm. Accessed August 30, 2017.
- Kurita H, Kurashina K, Honda T. Nosocomial transmission of methicillin-resistant Staphylococcus aureus via the surfaces of the dental operatory. Br Dent J. 2006;201:297–300.
- World Health Organization. WHO Urges Action Against HIV Drug Resistance Threat. Available at: who.int/mediacentre/news/releases/2017/hiv-drug-resistance/en/. Accessed August 30, 2017.
- U.S. Centers for Disease Control and Prevention. Guidelines for Infection Control in Dental Health-Care Settings — 2003. Available at: cdc.gov/mmwr/preview/mmwrhtml/rr5217al.htm. Accessed August 30, 2017.
- U.S. Centers for Disease Control and Prevention. Summary of Infection Prevention Practices in Dental Settings: Basic Expectations for Safe Care. Available at: cdc.gov/oralhealth/infectioncontrol/pdf/safe-care.pdf. Accessed August 30, 2017.
- Occupational Safety and Health Administration. Medical & Dental Offices. A Guide to Compliance with OSHA Standards. Available at: osha.gov. Accessed August 30, 2017.
- Cleveland JL, Gray SK, Harte JA, Robison VA, Moorman AC, Gooch BF. Transmission of blood-borne pathogens in US dental health care settings: 2016 update. J Am Dent Assoc. 2016;147:729–738.
- Cleveland JL, Bonito AJ, Corley TJ, et al. Advancing infection control in dental care settings: Factors associated with dentists’ implementation of guidelines from the Centers for Disease Control and Prevention. J Am Dent Assoc. 2012;143:1127–1138.
- Laramie AK, Bednarsh HS, Isman B, et al. Use of bloodborne pathogens exposure plans in private dental practices: results and clinical implications of national survey. Compend Contin Educ Dent. 2016;38:398–407.
- McCarthy GM, Koval JJ, MacDonald JK. Compliance with recommended infection control procedures among Canadian dentists: results of a national survey. Am J Infect Control. 1999;27:377–384.
- Kelsch N, Davis CA, Essex G, Laughter L, Rowe DJ. Effects of mandatory continuing education related to infection control on the infection control practices of dental hygienists. Am J Infect Control. March 17, 2017. Epub ahead of print.
- Palenik CJ, Miller CH. Creating the position of office safety coordinator. Dent Assist. 2002;71:10–14.
- Organization for Safety, Asepsis and Prevention. Team Huddle Defining the role of the infection control coordinator: Part 2. Infection Control in Practice. 2015;14:1–4.
- Occupational Safety and Health Administration. Quick Reference Guide to the Bloodborne Pathogens Standard. Available at: www.osha.gov/SLTC/bloodbornepathogens/bloodborne_quickref.html. Accessed August 30, 2017.
- U.S. Centers for Disease Control and Prevention. DentalCheck. Available at: cdc.gov/oralhealth/infectioncontrol/dentalcheck.html. Accessed August 30, 2017.
- Flodgren G, Hall AM, Goulding L, et al. Tools developed and disseminated by guideline producers to promote the uptake of their guidelines. Cochrane Database Syst Rev. 2016;8:CD010669.
- U.S. Food and Drug Administration. FDA Basics. Available at: fda.gov/AboutFDA/Transparency/Basics/ucm194879.htm. Accessed August 30, 2017.
- O’Connor H, Armstrong N. An evaluation of washer-disinfectors (WD) and dishwashers (DW) effectiveness in terms of processing dental instruments. J Ir Dent Assoc. 2014;60:84–89.
- Rutala WA, Gergen MF, Weber DJ. Efficacy of a washer-disinfector in eliminating healthcare-associated pathogens from surgical instruments. Infect Control Hosp Epidemiol. 2014;35:883–885.
- Boyce JM, Kelliher S, Vallande N. Skin irritation and dryness associated with two hand-hygiene regimens: soap-and-water hand washing versus hand antisepsis with an alcoholic hand gel. Infect Control Hosp Epidemiol. 2000;21:442–448.
- Boyce JM, Pittet D; Healthcare Infection Control Practices Advisory Committee; HICPAC/SHEA/ APIC/IDSA Hand Hygiene Task Force. Guideline for Hand Hygiene in Health-Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Society for Healthcare Epidemiology of America/Association for Professionals in Infection Control/Infectious Diseases Society of America. MMWR Recomm Rep. 2002;51(RR-16):1–45.
- Siegel JD, Rhinehart E, Jackson M, Chiarello L, Healthcare Infection Control Practices Advisory Committee. 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings. Available at: cdc.gov/hicpac/pdf/isolation/Isolation2007.pdf. Accessed August 30, 2017.
- Baig AS, Knapp C, Eagan AE, Lewis RN, Radonovich LJ. Health care workers’ views about respirator use and features that should be included in the next generation of respirators. Am J Infect Control. 2010;38:18–25.
- Sorra JS, Nieva VF. Hospital Survey on Patient Safety Culture. AHRQ Publication No. 04-0041.Rockville, Maryland: Agency for Healthcare Research and Quality; 2004.
- The National Institute for Occupational Safety and Health. Stop Sticks Campaign. Safety Culture: Evaluation Survey. Available at: cdc.gov/niosh/stopsticks/survey.html. Accessed August 30, 2017.
Featured image by GEORGERUDY/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. October 2017;3(10):22–25.
