
 BRANIMIR76/ISTOCK/GETTY IMAGES PLUS
BRANIMIR76/ISTOCK/GETTY IMAGES PLUS
Diagnosing Incidental Thyroid Calcifications on Dental Images
Early detection of thyroid nodules is critical in differentiating between malignant and nonmalignant lesions in order to implement appropriate management strategies.
PURCHASE COURSE
This course was published in the December 2020 issue and expires December 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the December 2020 issue and expires December 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the prevalence and causes of thyromegaly (goiter).
- Describe methods for. diagnosing and treating goiter, as well as conditions that may have a similar radiographic appearance.
- Explain malignancy. rates with thyroid nodules.
The term goiter refers to an enlarged thyroid, or thyromegaly. Goiters can exhibit solitary nodules or multiple thyroid nodules (multinodular) that are either normal, functioning or nonfunctioning. They are classified as nontoxic or toxic, and can be a sign of thyroid disorders that cause the thyroid gland to produce too little hormone (hypothyroid) or too much (hyperthyroid). Goiters occur in approximately 15.8% of the population, and are more prominent in females age 40 and older. Additional risk factors include genetics, endogenous elements, facial radiation exposure, and iodine deficiency — which is the most common cause of goiters. A majority of patients with goiter can be asymptomatic, while those with symptoms can exhibit tussis, dyspnea, dysphagia, or tightness in the throat due to substernal expansion into the chest. Treatment of overactive thyroids includes medicinal approaches or use of radioactive iodine. Surgery can be advised for large goiters that obstruct the airway or cause dysphagia, as well as for certain metastatic thyroid nodules.1–3
Technological advances in imaging modalities have improved oral health professionals’ ability to identify thyroid nodules. Clinically, they are detected incidentally — often with the use of computed tomography (CT) scans, positron emission tomography, and magnetic resonance imaging (MRI).3
A thyroid nodule is a lesion in the thyroid gland that is different radiologically from its outlining parenchyma. Thyroid nodules are not uncommon. They are found in 50% to 60% of adults, and, as noted, are more prevalent in females, with an occurrence ratio of 4:1 female to male. In addition, their occurrence increases to 50% in women age 70 and older.4
To properly manage thyroid nodules, it is necessary to first differentiate the lesions and identify them as neoplastic or nonneoplastic. Thyroid nodules must be evaluated for potential thyroid cancer because 5% to 15% are pathologically malignant.5 Thyroid-stimulating hormone (TSH) has proven to be an important factor in thyroid nodule formation, as increased levels of serum TSH correlate with higher prevalence of thyroid malignancy.1 Treatment includes fine-needle aspiration biopsy (FNAB) and surgical removal, while less invasive management includes periods of observance.
 Postoperatively, FNAB has proven to be the gold standard of differentiation between benign and malignant nodules.5 It is the physician’s discretion whether the nodule requires fine-needle aspiration, or whether the nodules may be actively monitored.6 According to the American Thyroid Association, FNAB is recommended for nodules that measure greater than 1 cm in size. Nodules measuring less than 1 cm do not require biopsy unless there is involvement of lymph nodes, previous exposure to radiation, or a family history of thyroid cancer. A few factors that can increase risk of malignancy include genetics, gender, age, and past history of radiation therapy to the head or neck regions. If the patient is not predisposed to having a high risk for thyroid cancer, it is permissible to monitor the nodule with no further intervention.7
Postoperatively, FNAB has proven to be the gold standard of differentiation between benign and malignant nodules.5 It is the physician’s discretion whether the nodule requires fine-needle aspiration, or whether the nodules may be actively monitored.6 According to the American Thyroid Association, FNAB is recommended for nodules that measure greater than 1 cm in size. Nodules measuring less than 1 cm do not require biopsy unless there is involvement of lymph nodes, previous exposure to radiation, or a family history of thyroid cancer. A few factors that can increase risk of malignancy include genetics, gender, age, and past history of radiation therapy to the head or neck regions. If the patient is not predisposed to having a high risk for thyroid cancer, it is permissible to monitor the nodule with no further intervention.7
Contrary to some reports, no correlation has been shown between the risk of malignancy and nodule size, as studies have demonstrated the volume and diameter of a thyroid nodule cannot be used as sole factors for predicting malignancy or if surgical resection is indicated.5
Several modalities are useful when imaging thyroid masses, including ultrasound, CT scans and MRI. In general, ultrasound is preferred due to its sensitive detection methods and ability to reveal malignancies compared to other imaging techniques.4 Thyroid cancer incidence has been increasing steadily over time, especially in patients with small papillary cancers.6 A few radiographic features of thyroid mass malignancy include microcalcification, solid composition, hypoechoic patterns, and increased vascularity.5
Case Report
A 78-year-old female patient presented to a university clinic for a routine dental appointment. The patient’s medical history included thyroid disease, hypertension and liver/kidney disease. Her medication list included levothyroxine daily for hypothyroidism, a condition in which the thyroid gland does not produce adequate thyroid hormone. A thorough dental exam was completed, and a comprehensive treatment plan composed. The plan consisted of extraction of tooth #31 due to nonrestorability, and definitive treatment options included implant placement at sites #19 and #20 to restore posterior function in the lower-left posterior sextant.
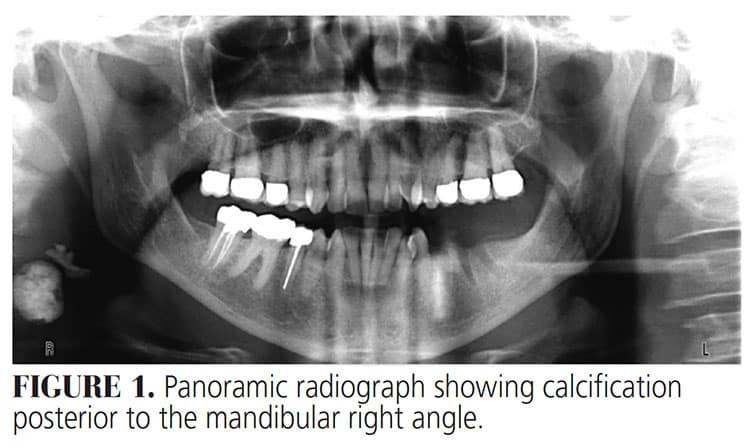
A diagnostic panoramic radiograph was captured, and incidental findings displayed a well-defined, ovoid, mixed lesion posterior to the mandibular right angle (Figure 1). Ultrasound was performed and findings demonstrated a hypoechoic nodule in the right thyroid lobe measuring 4 x 8 mm, with an isthmus of 3 mm in thickness, and a second hypoechoic nodule in the right thyroid lobe measuring 6 mm in thickness. The right thyroid lobe measured 2.9 x 1.1 x 1.0 cm. A hypoechoic nodule measuring 6 x 7 mm was found in the left thyroid lobe, which measured 3 x 0.7 x 1.3 cm. The jugular and carotid arteries were patent, with no distinct mass found. The results indicated bilateral, small thyroid nodules compatible with multinodular goiter. Treatment was not deemed necessary, and a six-month follow-up was recommended.
 Which of the following is most likely the diagnosis?
Which of the following is most likely the diagnosis?
- Carotid calcification
- Thyroid calcification
- Sialolith
- Tonsillolith
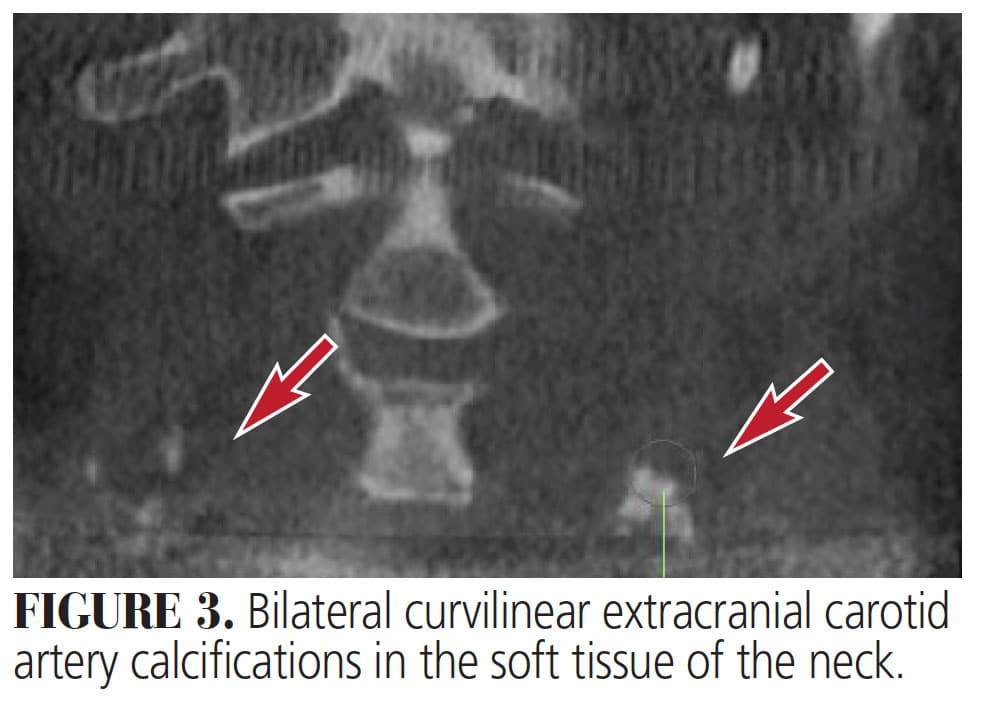
![FIGURE 3. Bilateral curvilinear extracranial carotid artery calcifications in the soft tissue of the neck.]() Discussion
Discussion
The patient’s gender, age, current thyroid condition and ultrasound reports, as well as the nodule’s appearance on the panoramic radiograph, strongly align with a diagnosis of thyroid goiter. The nodules discovered were less than 1 cm large. The patient was asymptomatic and not predisposed to having a high risk of thyroid cancer; therefore, treatment was not suggested at this time and she was advised to monitor the nodules.
Besides goiter, it is important to consider other entities that can also present as soft tissue calcifications on panoramic radiographs or cone beam computed tomography (CBCT). Some of these include extracranial carotid calcification, lymphoid tissue calcification/tonsillolith, and submandibular sialolith.
Extracranial Carotid Calcification — Atherosclerosis is an inflammatory arterial disease in which there are fatty plaque formations (atheromas) lining arterial walls. These plaques cause arteries to narrow, resulting in circulation restrictions when obstruction overtakes more than 50% to 70% of the diameter of the lumen, thus potentially manifesting in cerebrovascular accidents.8 Atheromas are the main calcifications that demand prompt treatment or a specialist referral.9 Carotid artery atherosclerosis accounts for approximately 5% of strokes.8 The gold standard of assessing and determining calcifications is duplex ultrasonography, but they can also be incidentally discovered on panoramic imaging (Figure 2) or CBCT scans (Figure 3) as radiopaque images. Panoramic radiography can play a vital role in early detection of atherosclerosis of the carotid artery if the plaques are positioned between the C3 and C4 cervical vertebrae, or the carotid bifurcation.8
With panoramic imaging, atheromas typically present as radiopaque masses along the common carotid artery area (which subsequently bifurcates into the internal and external carotid arteries), and are located on the inferior corners of a panoramic radiograph. However, panoramic imaging alone cannot be used to detect or confirm presence of extracranial calcified carotid atheromas due to low sensitivity. Two-dimensional images can alter the interpretation of calcifications, which can negatively affect clinical results.8 Risk factors for atherosclerosis include obesity, high cholesterol, hypertension, diabetes and chronic kidney disease, as well as lifestyle habits and genetic predisposition. It is also noted that carotid complications can be associated with primary hyperparathyroidism.10 Early detection is optimal for reducing the prevalence and detrimental effects of atherosclerosis.
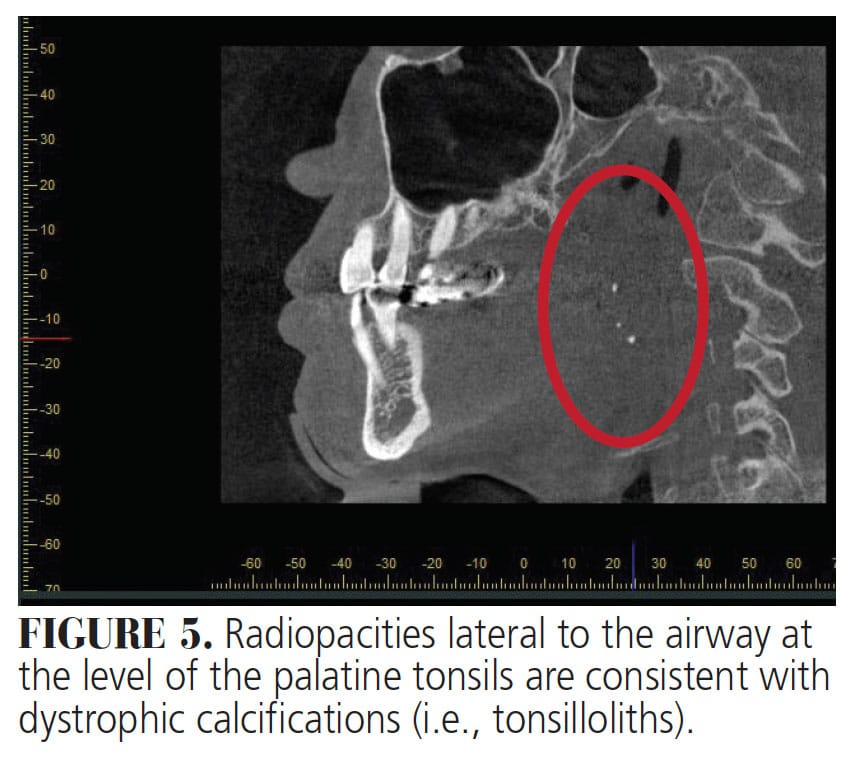
 Lymphoid Tissue Calcification/Tonsillolith — Tonsilloliths are concretions composed of calcium salts, tissue debris and other minerals found in tonsillar crypts. Their size can range from several millimeters to a few centimeters. They are primarily located in tonsillar tissue (69.7%), but are also found in the palatine tonsil or tonsillar fossa. They occur more commonly in adults, with the average age of onset being 46 years old, with an occurrence ratio of 2:1 male to female.11 Studies have shown that symptoms in the presence of tonsillar calculi are independent of their size. Tonsilloliths can produce symptoms such as otalgia, pharyngitis, swelling in tonsillar fossa, dysphagia and halitosis, but they can also be asymptomatic.12 Smaller lesions can be removed by curettage, while excision or tonsillectomy are considered for larger lesions.12 Tonsilloliths can be detected incidentally on routine panoramic (Figure 4) or CBCT radiographs (Figure 5). Clinically, CBCT scans and MRI can be useful diagnostic tools in depicting and diagnosing calcified lesions in the tonsillar region. When observed on a panoramic radiograph, tonsilloliths may present as single or multiple, round or irregular, unilateral or bilateral radiopaque masses superimposed onto the mandibular ramus, with a prevalence of 2% to 16%.13
Lymphoid Tissue Calcification/Tonsillolith — Tonsilloliths are concretions composed of calcium salts, tissue debris and other minerals found in tonsillar crypts. Their size can range from several millimeters to a few centimeters. They are primarily located in tonsillar tissue (69.7%), but are also found in the palatine tonsil or tonsillar fossa. They occur more commonly in adults, with the average age of onset being 46 years old, with an occurrence ratio of 2:1 male to female.11 Studies have shown that symptoms in the presence of tonsillar calculi are independent of their size. Tonsilloliths can produce symptoms such as otalgia, pharyngitis, swelling in tonsillar fossa, dysphagia and halitosis, but they can also be asymptomatic.12 Smaller lesions can be removed by curettage, while excision or tonsillectomy are considered for larger lesions.12 Tonsilloliths can be detected incidentally on routine panoramic (Figure 4) or CBCT radiographs (Figure 5). Clinically, CBCT scans and MRI can be useful diagnostic tools in depicting and diagnosing calcified lesions in the tonsillar region. When observed on a panoramic radiograph, tonsilloliths may present as single or multiple, round or irregular, unilateral or bilateral radiopaque masses superimposed onto the mandibular ramus, with a prevalence of 2% to 16%.13
 Submandibular Sialolith — Sialolithiasis is a common salivary disorder, with more than 80% of cases occurring in the submandibular glands and Wharton’s duct, resulting in acute or chronic inflammation.14 Their size ranges from approximately 1 to 10 mm, (Figure 6) with the average sialolith measuring 6 to 9 mm. Large sialoliths are called megaliths and are greater than 15 mm. They can expand at a rate of up to 1 to 1.5 mm annually.15 The exact etiology is still unknown, although it is found that presence of systemic disease, such as gout, predisposes patients to sialolithiasis.16 It is suggested that stone formation can occur due to intracellular micro-calculi formation. Sialolithiasis is more prominent in men than women, and 75% of cases occur unilaterally.17 Sialoliths are ovoid shaped, yellow in color, and made up of calcium phosphate, hydroxyapatite and other calcific concretions. Salivary submandibular sialoliths are composed of organic (18%) and inorganic (82%) material.16 Its saliva is more alkaline in nature and has a higher mucous content, which may be a significant reason why stones are more prevalent in the submandibular duct/gland.17 Sialolithiasis can cause pain, swelling, infection, and decrease salivary secretion because the stones cause obstruction of saliva, resulting in salivary gland atrophy due to salivary stasis.9 Accurate diagnosis can depend on proper evaluation, preoperative history, clinical examination and radiography. Occlusal radiographs enable accurate visualization of radiopaque salivary stones.15
Submandibular Sialolith — Sialolithiasis is a common salivary disorder, with more than 80% of cases occurring in the submandibular glands and Wharton’s duct, resulting in acute or chronic inflammation.14 Their size ranges from approximately 1 to 10 mm, (Figure 6) with the average sialolith measuring 6 to 9 mm. Large sialoliths are called megaliths and are greater than 15 mm. They can expand at a rate of up to 1 to 1.5 mm annually.15 The exact etiology is still unknown, although it is found that presence of systemic disease, such as gout, predisposes patients to sialolithiasis.16 It is suggested that stone formation can occur due to intracellular micro-calculi formation. Sialolithiasis is more prominent in men than women, and 75% of cases occur unilaterally.17 Sialoliths are ovoid shaped, yellow in color, and made up of calcium phosphate, hydroxyapatite and other calcific concretions. Salivary submandibular sialoliths are composed of organic (18%) and inorganic (82%) material.16 Its saliva is more alkaline in nature and has a higher mucous content, which may be a significant reason why stones are more prevalent in the submandibular duct/gland.17 Sialolithiasis can cause pain, swelling, infection, and decrease salivary secretion because the stones cause obstruction of saliva, resulting in salivary gland atrophy due to salivary stasis.9 Accurate diagnosis can depend on proper evaluation, preoperative history, clinical examination and radiography. Occlusal radiographs enable accurate visualization of radiopaque salivary stones.15
When detectable on a panoramic radiograph, depending on its location within the submandibular gland or salivary duct, a sialolith often presents as a unilateral, oval or elongated homogenously radiopaque mass that may be located inferior to the mandibular angle or superimposed on the body of the mandible.17
Other imaging techniques that can be utilized are sialography, CBCT, sialoendoscopy and scintigraphy. Sialography is used to visualize the ductal morphology, detect salivary stones, and note signs suggesting Sjogren’s syndrome. On the other hand, CBCT scans are a less invasive method to visualize calculus and the gland’s ductal system, and are proven to be superior in revealing stenosis, strictures, and stone identification (compared to traditional sialography).18 Generally, CBCT sialography is considered the modality of choice in viewing obstructive salivary gland cases because it offers three-dimensional reconstruction of images, which, in turn, allows complex anatomy to be viewed from any slice of thickness and direction.19
Treatment modalities for sialolithiasis vary depending on size of the stone, location, and presence of infection. For smaller sialoliths, sialoendoscopy and extracorporeal short-wave lithotripsy are appropriate treatment methods; alternatives include bimanual palpation or flushing the stone from the ductal orifice and prescribing an antistaphylococcal, penicillinase-resistant antibiotic.16 Treatment for larger sialoliths include sialolithectomy and transpolar sialolithotomy with sialodochoplasty.18
![FIGURE 6. Punctate radiopacity within the right floor of mouth, consistent with a right submandibular sialolith within the right submandibular duct (i.e., Wharton’s duct).]() Summary
Summary

Goiter is the common term for thyromegaly. Incidence is common in females age 40 and older and patients with high levels of TSH, and those with a history of hypothyroidism should be clinically assessed and evaluated for an enlarged thyroid and presence of thyroid nodules. Multinodular goiters can be toxic (producing too much hormone) or nontoxic (not producing adequate hormone). With thyroid nodules, approximately 7% is prone to malignancy, and early detection is critical in differentiating between malignant and nonmalignant lesions, and initiating treatment accordingly.
Approaches to treating multinodular goiters depend on size, FNAB results, rate of growth, and risk of malignancy. Thyroid nodules can be detected on panoramic or CBCT radiographs. This review article can serve as a useful resource for clinicians encountering multiple thyroid nodules on diagnostic orofacial radiographic images.
References
- Dauksiene D, Petkeviciene J, Klumbiene J, et al. Corrigendum to “Factors Associated with the Prevalence of Thyroid Nodules and Goiter in Middle-Aged Euthyroid Subjects.” Int J Endocrinol. 2019;2019:1.
- Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26:1–133.
- Pemayun TD. Current diagnosis and management of thyroid nodules. Acta Med Indones. 2016;48:247–257.
- Fisher SB, Nancy DP. The incidental thyroid nodule. CA Cancer J Clin. 2018;68:97–105.
- Bestepe N, Ozdemir D, Baser H, et al. Is thyroid nodule volume predictive for malignancy? Arch Endocrinol Metab. 2019;63:1–8.
- Nabhan F, Matthew DR. Thyroid nodules and cancer management guidelines: comparisons and controversies. Endocr Relat Cancer. 2017;24:R13–R26.
- Roman BR, Morris LG, Davies L. The thyroid cancer epidemic, 2017 perspective. Curr Opin Endocrinol Diabetes Obes. 2017;24:332–336.
- Khosropanah SH, Shahidi SH, Bronoosh P, Rasekhi A. Evaluation of carotid calcification detected using panoramic radiography and carotid doppler sonography in patients with and without coronary artery disease. Br Dent J. 2009;207:E8,discussion 162–163.
- Missias EM, Nascimento E, Pontual M, et al. Prevalence of soft tissue calcifications in the maxillofacial region detected by cone beam CT. Oral Dis. 2018;24:628–637.
- Borba DL, Hipólito UV, Pereira YC. Early diagnosis of atherosclerosis with panoramic radiographs: a review. J Vasc Bras. 2016;15:302–307.
- Misirlioglu M, Nalcaci R, Adisen MZ, Yardimci S. Bilateral and pseudobilateral tonsilloliths: Three dimensional imaging with cone-beam computed tomography. Imaging Sci Dent. 2013;43:163–169.
- Kanotra S, Kanotra S, Paul J. A giant tonsillolith. Indian J Otolaryngol Head Neck Surg. 2008;60:277–280.
- Abdelkarim AZ, Lozanoff S, Abu el Sadat SM, Syed AZ. Osteoma cutis and tonsillolith: a cone beam computed tomography study. Cureus. 2018;10:e3003.
- Kolomiiets SV, Udaltsova KO, Khmil TA, Yelinska AM, Pisarenko OA, Shynkevych VI. Difficulties in diagnosis of sialolithiasis: a case series. Bull Tokyo Dent Coll. 2018;59:53–58.
- Alkurt MT, Ilkay P. Unusually large submandibular sialoliths: report of two cases. Eur J Dent. 2009;3:135–139.
- Siddiqui SJ. Sialolithiasis: an unusually large submandibular salivary stone. Br Dent J. 2002;193,89–91.
- Capote TS, Goncalves MA, Goncalves A, Goncalves M. Panoramic radiography — diagnosis of relevant structures that might compromise oral and general health of the patient. In: Virdi M, ed. Emerging Trends in Oral Health Sciences and Dentistry. London: InTech Open; 2015:733–762.
- Arifa SP, Christopher PJ, Kumar S, Kengasubbiah S, Shenoy V. Sialolithiasis of the submandibular gland: Report of cases. Cureus. 2019;11:e4180.
- Abdel-Wahed N, Amer ME, Abo-Taleb NS. Assessment of the role of cone beam computed sialography in diagnosing salivary gland lesions. Imaging Sci Dent. 2013;43:17–23.
From Decisions in Dentistry. December 2020;6(11): 26-28, 31.

