
 DRAGANA991/ISTOCK/GETTY IMAGES PLUS
DRAGANA991/ISTOCK/GETTY IMAGES PLUS
Considerations for Asynchronous Teledentistry
The use of teledentistry has the potential to enhance access to care while improving outcomes and reducing costs.
PURCHASE COURSE
This course was published in the July 2021 issue and expires July 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the July 2021 issue and expires July 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Explain the use and benefits of teledentistry in the context of pre-pandemic, pandemic and post-pandemic care.
- Discuss the application and utility of digital technologies, particularly intraoral scanning, in teledentistry.
- Describe how implementation of teledentistry can improve access to care and potentially reduce the cost of oral healthcare.
REGULATORY ADVISEMENT
The regulations regarding teledentistry consist of a patchwork system that can vary greatly from state to state. All dental providers should consult their state practice act to understand what is allowed. During the COVID-19 outbreak, many states changed scope of practice guidelines to allow the utilization and reimbursement of teledentistry, viewing it as an effective way to assess and triage patients while limiting in-office visits — except for those in need of urgent or emergency care.
Teledentistry is an innovative delivery model that helps democratize access to care. This technology frees oral healthcare from the patriarchal/matriarchal, physical and structural constraints of the dentist’s availability, creating dental equity through the use of auxiliary team members. This article will demonstrate how a dental hygienist can initiate quality preventive recall visits and asynchronously (i.e., nonconcurrently) share that clinical data with the supervising dentist to facilitate a diagnosis and treatment plan (if needed). Providers have used teledentistry to deliver care to vulnerable and underserved patients, both rural and urban, for more than a decade. An early example of successful implementation is the University of the Pacific School of Dentistry’s Virtual Dental Home model.1
While dental providers were adept at teledentistry prior to the pandemic, the advent of COVID-19 sparked new interest. In many cases, and especially when dental auxiliaries are involved, use of digital cameras, digital radiography and intraoral scanners (IOS) can play a key role in this clinical approach. This article will primarily focus on the utilization of scanning technology to capture diagnostic data and its resulting impact on preventive recall appointments.
Both before and during the pandemic, teledentistry technologies were used between dental hygienists and dentists to increase access to care in underserved populations, particularly in community healthcare settings. In mid-2020, for example, a pilot program based on earlier programs in California and Arizona was the first prototype used in Missouri. This program provided preventive care to school children and nursing home patients.
The fundamental elements of the teledentistry outreach pilot program were implemented into the authors’ private practice on a limited basis. Teledentistry was utilized as a system to cover hours when the doctor was not available due to vacation, dental conferences or illness. During these times, the dental hygienist was able to facilitate periodic recall and emergency visits in the dentist’s absence. For the periodic recall, the asynchronous visit would include a teledentistry assessment with radiographs and intraoral and extraoral imaging — all contained within the practice management software. In the case of an emergency, pertinent information was gathered and exchanged over a cloud-based system with secure, synchronous teledentistry capabilities.
TRANSFORMATIVE INFLUENCES
The effects of the pandemic transformed the telehealth model within dentistry.2 During the COVID-19 outbreak, many states modified scope of practice guidelines to permit utilization and reimbursement of teledentistry, considering it a valid way to assess and triage patients while limiting in-office visits (except for urgent or emergency treatment).3 During this time, teledentistry was used to screen emergency visits, preserve resources, and conserve personal protective equipment, as recommended by the U.S. Centers for Disease Control and Prevention.4
Operating procedures using teledentistry applications were determined to be an effective and safe way to address initial and recall appointments. In fact, its use to facilitate hygiene assessments and recalls not only supports a high level of dental hygiene care, it also allows dentists to focus on diagnosis and restorative care.5
In clinical application, the authors have adapted and improved delivery of teledentistry services by digitizing diagnostic workflows. Rather than a traditional clinical photography system, IOS technology and other digital modalities are used during hygiene recall and new patient appointments, as well as restorative and orthodontic cases.
DATA CAPTURE
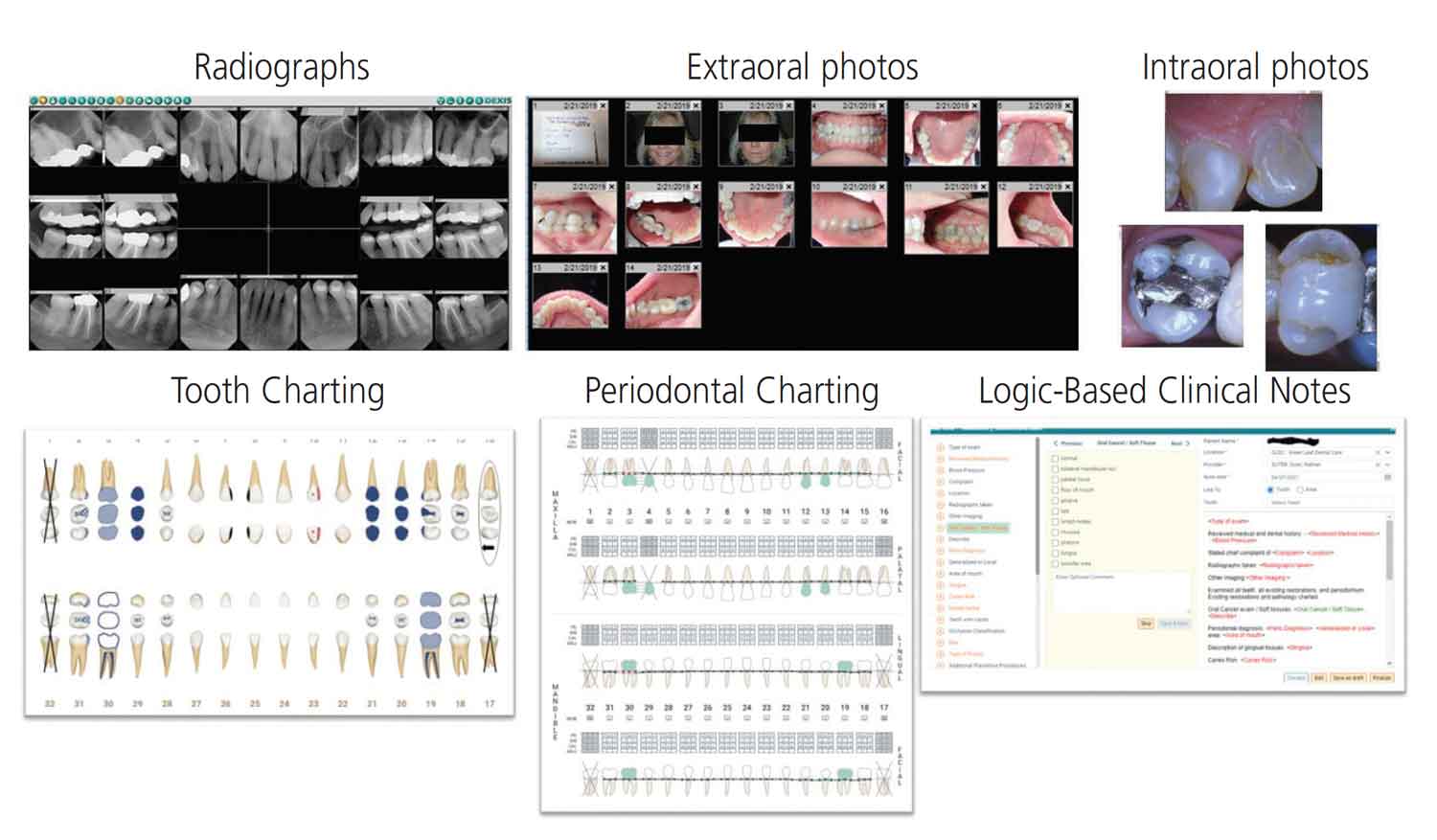
With teledentistry, the dentist must be able to view the patient’s dental condition and occlusal relationships via intraoral/extraoral imagery in order to make a definitive diagnosis and form a treatment plan. Based on the patient’s needs, the initial workflow consists of a comprehensive assessment performed by the dental hygienist, who takes a series of prescribed radiographs and a set of intraoral and extraoral images. In the example shown in Figure 1, the teledentistry intraoral photos were taken with a point-and-shoot camera that has a preset for dental photography. The photo series was similar to an orthodontic set and included a frontal, relaxed smile, mandibular and maxillary arch, left and right buccal view, and the lingual sextants. Capturing diagnostic dental images with a camera is technique sensitive, as it requires the ability to understand lightning, angles and positioning; additionally, including intraoral photographs for teeth with symptoms or conditions can make the procedure time consuming. Depending on the dental setting and internet capacity, the start-to-finish process (image capture, upload and orientation) can take anywhere from 15 to 40 minutes.
In addition to traditional photography, the dental hygienist takes any necessary radiographs based on the recall system, including periapical radiographs of teeth with symptoms or suspicious lesions. The clinician onsite also conducts an intra- and extraoral cancer screening. The extraoral exam involves a visual inspection of the head, face and neck, and palpation of nodes, glands, thyroid and the temporal mandibular joint. During the intraoral examination, the clinician inspects the gingiva, oral mucosa, tongue, palate and floor of the mouth. In case of any suspicious pathology, the dental hygienist obtains historical data from the patient, then takes a photograph and documents the lesion by describing the location, definition of distribution, color and size in the clinical notes. If the patient is age 18 or older, full-mouth periodontal probing is charted annually, along with mobility or other conditions of the periodontium. The dental hygienist reviews and ensures the patient’s teeth are correctly represented in the odontogram. In addition, detailed notes are recorded based on all signs, symptoms, oral cancer screening, or conditions observed during the appointment. Finally, the onsite attending clinician provides the appropriate preventive care scheduled for that patient’s recall.
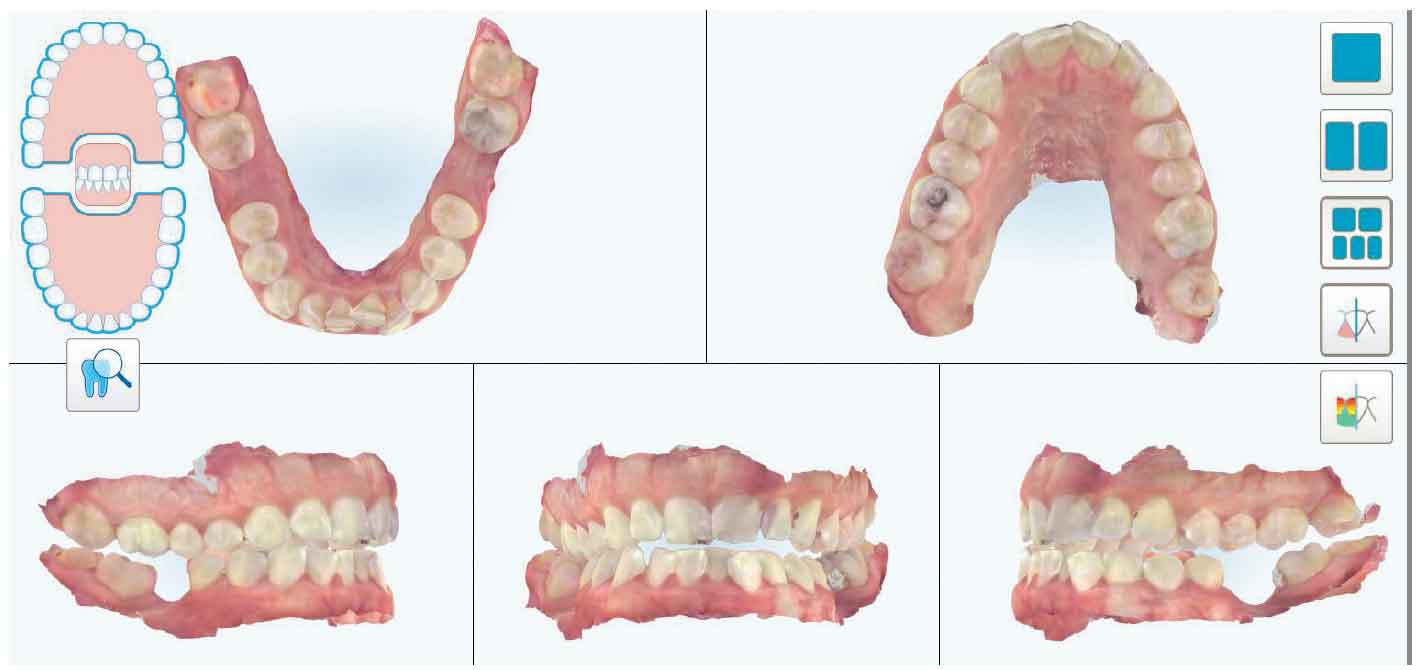
As noted, the authors’ office has replaced traditional photography for teledentistry care and now imagery is captured with IOS technology (Figure 2). When the patient presents for a teledentistry assessment, his or her information is entered into the IOS software. Next, the dental hygienist completes a five- to seven-minute full-mouth scan which encompasses the maxilla, mandible and bite registration. The facilitator then reviews and interprets the scan, making note of anything that may require further clinical investigation. The dental hygienist operating the IOS obtains feedback from the artificial intelligence of the IOS system to improve the images for the dentist. For quality control purposes, the IOS indicates in real time any teeth or areas of the dentition that need further scanning. This improves outcomes, as this process is an enhancement over traditional photographic series and intraoral photographs. Finally, the scan is uploaded into a secure cloud-based system for diagnostic review by the dental team.
Today’s IOS systems provide not just enhanced and predictable imagery, but additional diagnostic features useful in complete examinations. Utilization of this technology allows for more than just a three-dimensional (3D) color model of the patient’s teeth; newer units offer simultaneous capture of additional diagnostic data. The scanner used in the authors’ practice, for example, captures the occlusion, hundreds of intraoral photographs, and near infrared imaging. There are also IOS systems with the capability of capturing fluorescence, articulation with simulated movement, and more through the artificial intelligence feature.
TREATMENT PLANNING IN TELEDENTISTRY
When treatment planning for teledentistry recall patients, all clinical data are used to complete the evaluation and plan treatment. This planning can consist of primary, secondary or tertiary care. Typical procedures might involve prophylaxis, sealants, restorations and prosthodontics. This evaluation incorporates the use of software from the electronic dental record system, IOS, digital radiography, and task management platform. Along with detailed notes from the onsite dental hygienist, the dentist would consider previous radiographs, plus new X-rays at time of recall, combined with IOS imaging.
RECORDS AND MANAGEMENT SYSTEMS
The patient’s dental chart in the practice management system is an ideal place to begin a teledentistry examination — for example, by reviewing the odontogram to understand the existing state of the patient’s dentition after the dental hygienist’s initial assessment. This visual representation of the oral cavity can be enhanced by utilizing condition codes representing any findings by the dental hygienist documented at the asynchronous visit. Such records might indicate diagnostic data in the IOS, radiographs, periodontal charting and clinical notes. This is also the place to review previous clinical notes, medical alerts, allergies and dental treatment history.
The 3D record provides a presentation of the overall dentition and supporting alveolar structures. In previous workflows, it is the authors’ experience that relying on intraoral photographs alone can lead to confusion in interpreting the orientation of the mouth. In addition, using teledentistry photography can result in low-quality or missing images that make treatment planning inconclusive. The IOS can eliminate these errors due to the artificial intelligence in the scanner software that alerts the onsite clinician to areas that were missed during the scanning process. The true color and ability to orient the model allows comparison with the dental record to assess conditions and possible treatment outcomes. Recent studies indicate that using intraoral scans alone were effective in detecting dental findings, although not as effective in detecting periodontal conditions without further information.6
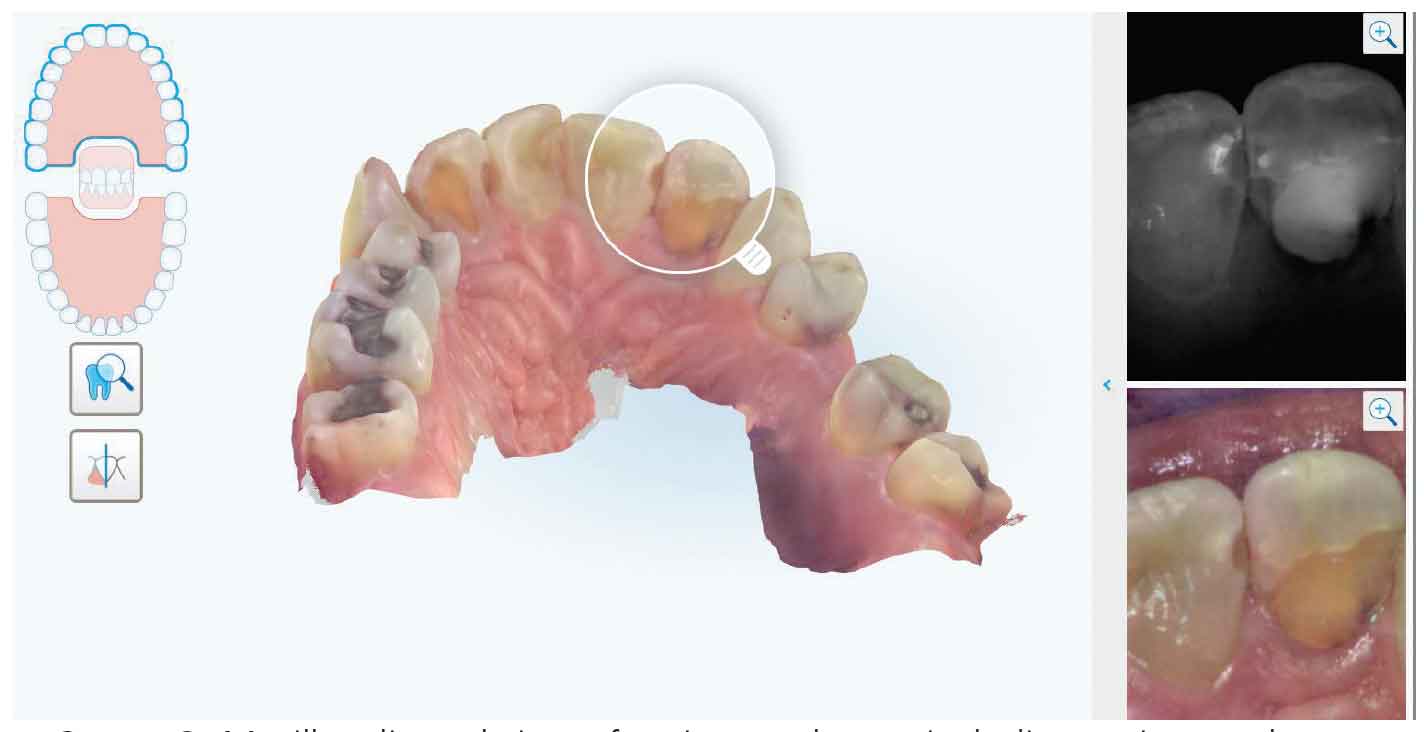
Many of the new IOS systems can record intraoral photos in addition to the 3D model of the dentition. This ability to examine photos of multiple areas and all tooth surfaces provides a detail-oriented way to evaluate the teeth and gingiva. The authors’ IOS system has the functionality to cast a virtual magnifying glass across the model and display both the intraoral photographs and near infrared images onscreen (Figure 3 and Figure 4). By combining the IOS, radiographs and clinical data recorded by the dental hygienist, a complete picture of the patient’s oral health can be assessed. Additional indications for IOS systems may come to light as the technology improves and providers become more comfortable with a digital workflow.7

SCANNER PROS AND CONS
In practice, the scanner has limited functionality for soft tissue analysis. Additional intraoral photographs are taken with a camera for areas of the mouth not covered by the scan. The dental hygienist documents subsequent findings, describing any soft tissue lesions observed during the teledentistry assessment. A study of elderly patients in two countries demonstrates that dental hygienists communicating via teledentistry with dentists can be highly accurate when comparing results to traditional in-person examinations.8 The patients were also more likely to receive regular care.
The patient experience of the IOS process indicates mixed reviews. Sharing the imaging fosters engagement and helps improve patient education and case acceptance, as this new perspective supports conversations about functional issues, disease processes, esthetic concerns and more. During use, concerns have been expressed by patients about the bulkiness of the IOS wand, which can be exacerbated due to the rigidity of the wand when navigating complex anatomy. Additionally, waiting for the artifical intelligence feature to catalog a pontic, missing tooth, tori, or primary teeth can be challenging — not just for the clinician, but also patients — due to time constraints.
PRACTICAL CONSIDERATIONS
Since a dentist’s physical presence is not needed for every patient recall, teledentistry has the potential to allow effective care delivery at lower cost.9 The application of teledentistry can facilitate increased dental hygiene production to offer more services per day. And while the capital investment for an IOS system is steep — they can range between $20,000 and $50,000, plus licensing and user fees — this may be offset by increased production and revenue.
Using teledentistry, the number of dental hygiene patients treated per day can be amplified using multiple dental operatories, as well as offsite visits. This approach can be used to provide care for low-risk recall patients, thereby making the dentist available for face-to-face visits with patients with greater dental needs. In addition, this type of general supervision of dental auxiliaries permits an office to gain productive new hours, therefore increasing revenue and patient access by offering convenient hours (evenings and weekends, for example). All of the aforementioned are potential advantages in efficiency and capacity.
CONCLUSION
Beyond other applications, asynchronous teledentistry can be used for the purpose of maintaining dental hygiene recall patients. The literature has supported this use for more than a decade. Prior to the COVID-19 pandemic, teledentistry was mostly used in public health settings in which dental hygienists would visit schools and nursing homes for data capture to be reviewed by an offsite supervising dentist.10 This article demonstrates that a dental office can offer recall hygiene appointments via teledentistry, with a dentist asynchronously reviewing collected patient data.
The literature indicates the efficacy and potential of new technologies being used for teledentistry. As demonstrated in the authors’ practice, teledentistry is viable in an office setting in response to the pandemic and going forward. In this model, the dental hygiene team documents the patient’s condition via radiographs, intraoral photos, IOS imaging and clinical charting for asynchronous review by a dentist. Combining all of the available clinical data — including documentation of signs and symptoms of hard and soft tissues by a calibrated dental hygienist — the dentist can complete an examination, reach a diagnosis, and develop a treatment plan. This approach has the potential to enhance access to care while simultaneously reducing costs and improving outcomes.
REFERENCES
- Namakian M, Subar P, Glassman P, Quade R, Harrington M. In-person versus “virtual” dental examination: congruence between decision-making modalities. J Calif Dent Assoc. 2012;40:587–595.
- Missouri Coalition for Oral Health. Creating Access: Teledentistry in Missouri. Available at: https://www.oralhealthmissouri.org/2021-conference-creating-access-teledentistry-in-missouri. Accessed May 26, 2021.
- Alabdullah JH, Daniel SJ. A systematic review on the validity of teledentistry. Telemed J E Health. 2018;24:639–648.
- U.S. Centers for Disease Control and Prevention. Hierarchy of Controls. Available at: https://www.cdc.gov/niosh/topics/hierarchy/default.html. Accessed May 26, 2021.
- Suter N. Teledentistry applications for mitigating risk and balancing the clinical schedule. J Public Health Dent. 2020;80(Suppl 2):S126–S131.
- Steinmeier S, Wiedemeier D, Hämmerle CH, Mühlemann S. Accuracy of remote diagnoses using intraoral scans captured in approximate true color: a pilot and validation study in teledentistry. BMC Oral Health. 2020;20:266.
- Suese K. Progress in digital dentistry: The practical use of intraoral scanners. Dent Mater J. 2020;39:52–56.
- Queyroux A, Saricassapian B, Herzog D, et al. Accuracy of teledentistry for diagnosing dental pathology using direct examination as a gold standard: Results of the Tel-e-dent study of older adults living in nursing homes. J Am Med Dir Assoc. 2017;18:528–532.
- Estai M, Bunt S, Kanagasingam Y, Tennant M. Cost savings from a teledentistry model for school dental screening: an Australian health system perspective. Aust Health Rev. 2018;42:482–490.
- Glassman P, Helgeson M, Kattlove J. Using telehealth technologies to improve oral health for vulnerable and underserved populations. J Calif Dent Assoc. 2012;40:579–585.
From Decisions in Dentistry. July 2021;7(7):25-28.

