

Clinical Manifestations of Kidney Disease
Patients with this common condition may present with a variety of oral side effects.
Patients with this common condition may present with a variety of oral side effects
Kidney disease is a progressively debilitating condition that leads to end-stage renal disease (ESRD), in which the kidneys cease to support daily bodily function — requiring either dialysis or a kidney transplant. The progression to kidney failure may take as long as 10 to 20 years. Diabetes and high blood pressure are the most common causes of ESRD in the United States.1
After rising nearly 600% from 1980 to 2009, the incidence of ESRD in the U.S. has stabilized. Today, more than 871,000 people receive treatment for kidney disease. An aging population, as well as the increased prevalence of obesity, diabetes and hypertension, have contributed to the rapid increase in ESRD cases.2 The number of deaths from ESRD rose from 10,478 in 1980 to 90,118 in 2009.3 Cardiovascular disease associated with ESRD is the most frequent cause of death among older adults.2
Because the kidneys perform critical functions, including expelling waste (especially urea), producing red blood cells, regulating blood pressure, and creating calcitrol (which regulates calcium, phosphate and vitamin D) ESRD is particularly debilitating.4 Kidney disease often does not exhibit any symptoms until it is in the advanced stages. Oral health professionals can help detect early warning signs by evaluating patients for high blood pressure and diabetes, and determining whether patients have a history of heart or kidney disease. If these signs are present, the patient should be referred to a physician, as early treatment can reduce the likelihood of ESRD developing.
Renal failure is associated with a decreased glomerular filtration rate (GFR), which calculates how much blood moves through the glomeruli (small filters in the kidneys that remove waste from the blood) each minute.1 Healthy adults have a GFR of about 140; normal is greater than 90. Children and older adults usually have lower GFR levels. A GFR less than 15 is indicative of kidney failure. Measuring blood urea nitrogen (BUN) is another indicator of waste, or urea, in the blood. Urea is produced from the breakdown of protein already in the body that is gained through diet. A high BUN level usually means that kidney function is less than normal, but other factors may also affect the reading. Bleeding in the intestines, congestive heart failure and certain medications may increase BUN levels. As these levels rise, symptoms of kidney disease may appear, such as a bad taste in the mouth, poor appetite, nausea and vomiting. Monitoring BUN levels can help clinicians ascertain whether a patient is receiving the correct amount of dialysis. Sometimes a low reading may also mean the individual is not eating enough protein. The normal level for healthy individuals is 7 mg/dL to 20 mg/dL in adults, and 5 mg/dL to 18 mg/dL in children. Patients on dialysis have higher BUN levels (usually 40 mg/dL to 60 mg/dL). A nephrologist and dietitian can help determine whether a patient’s BUN level is in the correct range.5
When the kidneys fail, the body fills with extra water and waste products (i.e., uremia). Individuals with ESRD will often feel ill and fatigued. Common symptoms include nausea and loss of appetite, itching and dry skin, and numbness in the hands. Patients may experience excessive thirst and breath malodor. These are caused by the presence of nitrogen and other toxins in the blood.2
There are two main types of dialysis. In peritoneal dialysis, a fluid called dialysate is delivered daily into the abdominal cavity via a catheter to capture waste products from the blood. This allows toxic solutes to diffuse from the peritoneal capillaries to the dialysate. After a few hours, the dialysate containing the body’s waste is drained away.5–7 In hemodialysis, the patient’s blood is sent through a machine that filters waste products. The purified blood is returned to the body through an arteriovenous shunt. During treatments, patients are given heparin to ease blood exchange and prevent clotting.6–8
FINDINGS IN THE ORAL CAVITY
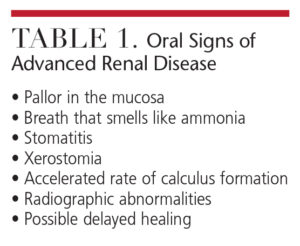 Renal failure may cause a variety of changes in the oral cavity. Paleness of the mucosa is caused by a normochromic/normocytic anemia due to decreased production of erythropoietin. Urea accumulation in the saliva can cause the breath to smell like ammonia. Patients may experience increased calculus formation due to altered serum calcium-phosphate production. A uremic stomatitis may develop because of elevated levels of urea nitrogen in the blood. This may manifest as red mucosal ulcers or a thick gray exudate covering the mucosa.7–9
Renal failure may cause a variety of changes in the oral cavity. Paleness of the mucosa is caused by a normochromic/normocytic anemia due to decreased production of erythropoietin. Urea accumulation in the saliva can cause the breath to smell like ammonia. Patients may experience increased calculus formation due to altered serum calcium-phosphate production. A uremic stomatitis may develop because of elevated levels of urea nitrogen in the blood. This may manifest as red mucosal ulcers or a thick gray exudate covering the mucosa.7–9
Many patients with renal failure experience renal osteodystrophy. This bone disease occurs when the kidneys are unable to maintain the proper levels of calcium and phosphorus in the blood, leaving the bones demineralized and weak. Renal osteodystrophy can begin many years before symptoms appear. In children, enamel hypoplasia may result due to the disturbances in calcium and phosphate metabolism. Well circumscribed, unilocular or multilocular radiolucencies may be seen on X-rays. These central giant cell lesions are referred to as brown tumors, due to hemosiderin pigmentation.10
Additional oral manifestations of kidney disease include loss of lamina dura, decreased trabeculation, ground glass appearance on radiographs, and abnormal bone healing after extractions.11 Occasionally, narrowing of pulp chambers may be seen.10 Table 1 lists the oral symptoms of advanced renal disease.
XEROSTOMIA
Xerostomia is common among patients with kidney disease because of the altered fluid balance in the oral cavity. In a study of 79 patients who either were undergoing dialysis or had received a kidney transplant, approximately 30% complained of xerostomia.12 This may be caused by this population’s high use of antihypertensive medications. When xerostomia is present, the risk of caries, altered taste sensations, candidiasis, and soreness caused by the rubbing of an oral prosthesis on the mucosa increase. Additionally, patients undergoing hemodialysis often experience a metallic taste and a white-coated tongue.12
Patients with ESRD take multiple medications, some of which can cause xerostomia. Hemodialysis has a transient stimulatory effect on the salivary flow rate, but overall salivary rates are still lower than in healthy individuals. In patients with diabetes, the salivary flow rate is further reduced. Patients undergoing hemodialysis experience saliva that has an increased viscosity and reduced buffering capacity. Drinking water to alleviate xerostomia symptoms cannot be recommended for patients with ESRD due to excessive water retention, but chewing sugar-free gum and/or gum containing xylitol may provide relief.13 While the research is mixed on the efficacy of artificial saliva and oral lubricants in patients undergoing hemodialysis, these products may provide some comfort.14 Secretagogues, including pilocarpine and cevimelin, that stimulate salivary flow have not been fully studied in this patient population.14
To reduce the risk of caries in patients with ESRD, the use of fluoride and cetylpyridinium chloride is indicated.15,16 Also, calcium phosphate technologies — such as amorphous calcium phosphate (ACP), casein phosphopeptide-ACP, calcium sodium phosphosilicate, and tri-calcium phosphate — may support remineralization, thereby reducing caries risk by supplying the oral cavity with additional calcium and phosphate ions.
PERIODONTAL HEALTH
As chronic kidney disease progresses to ESRD, patients’ gingival and periodontal status worsens.17 Patients with ESRD have higher scores on the Decayed Missing Filled Teeth Index, demonstrate statistically significant periodontal destruction, and experience increased incidence of periapical dental infections.18 Patients with chronic kidney disease may be unaware of their increased risk for oral disease.19
Chronic adult periodontal disease increases systemic inflammation, which may interfere in the management of ESRD. Affected individuals are at greater risk of mortality due to atherosclerotic complications, such as myocardial infarction, cardiac arrhythmia and cerebral vascular disease. Infection is the second most common cause of mortality. Moderate to severe periodontitis increases serum inflammatory markers. As such, it is possible that the treatment of periodontitis may reduce the inflammatory burden of ESRD, thus reducing the risk for mortality.4
key takeaways
- An aging U.S. population, as well as the increased prevalence of obesity, diabetes and hypertension, have contributed to the rapid increase in cases of end-stage renal disease (ESRD).2
- Dental providers can help detect early warning signs by evaluating patients for high blood pressure and diabetes, and determining whether patients have a history of heart or kidney disease.
- Among the many oral manifestations of kidney disease are loss of lamina dura, decreased trabeculation, ground glass appearance on radiographs, and abnormal bone healing after extractions.11 Breath malodor and xerostomia are common complaints.
- Besides implementing caries preventive regimens, clinicians should closely monitor these patients’ gingival and periodontal health, as both tend to worsen as chronic kidney disease progresses to ESRD.17
- Oral health professionals should be aware of the potential for excessive bleeding and anemia in patients undergoing dialysis. In addition, the possible need for antibiotic premedication should be discussed with a patient’s medical team before providing dental treatment.
DENTAL TREATMENT
Oral health professionals should be aware of the potential for excessive bleeding and anemia in patients undergoing dialysis. These patients take heparin to prevent clot formation while their blood is in the dialyzer. Fortunately, heparin has a short half-life, and dental treatment can be performed safely the day after dialysis. Hemodialysis causes physical destruction of platelets, however, which can increase bleeding. A platelet count should be considered if significant bleeding is anticipated during dental treatment.6 As the kidneys are responsible for red blood cell production, treatment should be planned so that excess bleeding does not occur.9 Clinicians may consider performing scaling and root planing in multiple, short appointments, for example, to reduce the potential for bleeding complications. And for the same reason, if a patient needs multiple extractions, the provider should consider scheduling the procedures over multiple appointments rather than in one sitting.
Certain medications should not be prescribed to patients with kidney disease. Tetracycline has a history of precipitating or aggravating renal failure. Nonsteroidal anti-inflammatory drugs are nephrotoxic when prescribed as a long-term medication, and even short-term use may be harmful for patients with advanced kidney disease. Many drugs need alternative dosing regimens when used in patients with severely impaired kidneys.19
Patients undergoing hemodialysis should be premedicated according to American Heart Association guidelines. Individuals using peritoneal dialysis, however, generally do not require premedication, as an arteriovenous shunt is not employed.20
![0316-kidney-2]() CONCLUSION
CONCLUSION
 CONCLUSION
CONCLUSIONPeriodontal disease, enamel abnormalities, premature tooth loss and xerostomia are all more common among patients undergoing dialysis. Clinicians can play a significant role in improving this population’s oral health by providing effective education about preventive therapies and oral hygiene, and emphasizing the importance of regular dental care.21–23 Table 2 discusses the dental management of patients with advanced kidney disease.
With the growing number of older adults in the U.S., oral health care providers are almost certain to treat patients with kidney disease, including ESRD. Interdisciplinary collaboration among the extended health care team is essential for appropriate management of individuals with advanced kidney disease. The need for antibiotic premedication and the potential for excessive bleeding, for example, should be discussed with patients’ medical providers before administering dental treatment. A careful review of medication usage, as well as taking a thorough medical and dental history, can help ensure patients are treated safely and efficiently. Patients’ health care teams should be notified of oral manifestations, such as oral malodor, stomatitis, xerostomia and delayed healing. Dental professionals should be especially vigilant in educating patients with kidney disease about the principles of maintaining good oral health.
References
- Proctor R, Kunar N, Stein A, Moles D, Porter S. Oral and dental aspects of chronic renal failure. J Dent Res. 2005;84:199–208.
- Abboud H, Henrich WL. Stage IV chronic kidney disease. N Engl J Med. 2010;362:56–65.
- United States Renal Data System. 2013 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease. Available at: usrds.org/atlas.aspx. Accessed February 10, 2016.
- Craig RG. Interactions between chronic renal disease and periodontal disease. Oral Diseases. 2008;14:1–7.
- Life Options. Lab Values Explained. Available at: lifeoptions.org/kidneyinfo/labvalues.php. Accessed February 10, 2016.
- Sharma DCG, Pradeep AR. End stage renal disease and its dental management. N Y State Dent J. 2007;73:43–47.
- Kerr AR. Update on renal disease for the dental practitioner. Oral Surg Oral Med Oral Pathol. 2001;92:9–16.
- DeRossi SS, Glick M. Dental considerations for the patient with renal disease receiving hemodialysis. J Am Dent Assoc. 1996;127:211–219.
- Levy HM. Dental considerations for the patient receiving dialysis for renal failure. Spec Care Dentist. 1988;8:34–36.
- Antonelli JR, Hottel TL. Oral manifestations of renal osteodystrophy: a case report and review of the literature. Spec Care Dentist. 2003;23:28–34.
- Rose LF, Genco RJ, Cohen DW. Mealy BL. Periodontal Medicine. St. Louis: BC Decker Inc; 2000:205–212.
- Dirschnabel AJ, Martins Ade S, Dantas SA, et al. Clinical oral findings in dialysis and kidney-transplant patients. Quintessence Int. 2011;42:127–133.
- Ly KA, Milgrom P, Rothen M. The potential of dental-protective chewing gum in oral health interventions. J Am Dent Assoc. 2008;139:553–563.
- Bossola M, Tazza L. Xerostomia in patients on chronic hemodialysis. Nat Rev Nephrol. 2012;8:176–182.
- Plemons JM, Al-Hashimi I, Marek CL, American Dental Association Council on Scientific Affairs. Managing xerostomia and salivary gland hypofunction: executive summary of a report from the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2014;145:867–873.
- Sreenivasan PK1, Haraszthy VI, Zambon JJ. Antimicrobial efficacy of 0.05% cetylpyridinium chloride mouthrinses. Lett Appl Microbiol. 2013;56:14–20.
- Tadakamadla J, Kumar S, Mamatha GP. Comparative evaluation of oral health status of chronic kidney disease patients in various stages and healthy controls. Spec Care Dentist. 2014;34:122–126.
- Thorman R, Neovius M, Hylander B. Clinical findings in oral health during progression of chronic kidney disease to end-stage renal disease in a Swedish population. Scand J Urol Nephrol. 2009;43:154–159.
- Brockman W, Badr M. Chronic kidney disease: pharmacological considerations for the dentist. J Am Dent Assoc. 2010;141:1330–1339.
- Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. J Am Dent Assoc. 2008;139(Suppl):3S–24S.
- Klassen JT, Krasko BM. The dental health status of dialysis patients. J Can Dent Assoc. 2002;68:34–38.
- Naugle K, Darby ML, Bauman DB, Lineberger LT, Powers R. The oral health status of individuals on renal dialysis. Ann Periodontol. 1998;3:197–205.
- Gudapati A, Ahmed P, Rada R. Dental management of patients with renal failure. Gen Dent. 2002;50:508–510.
