

Clear Aligners vs Traditional Braces
This evidence-based comparison covers treatment outcomes, length of treatment, patient-reported experiences, relapse tendencies, risk of root resorption, and effects on oral health.
PURCHASE COURSE
This course was published in the October/November 2025 issue and expires November 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the October/November 2025 issue and expires November 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 370
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the biomechanical principles of clear aligner therapy and how they differ from fixed orthodontic appliances.
- Evaluate the clinical efficacy, limitations, and patient-reported outcomes associated with clear aligner therapy compared to fixed appliances.
- Apply evidence-based criteria to case selection and treatment planning.
Clear aligner therapy has gained widespread popularity as a more esthetic, patient-friendly alternative to traditional fixed appliances. However, its efficacy in managing complex malocclusions that require intricate orthodontic mechanics remains debated.1 While aligners offer advantages, such as improved patient compliance, oral hygiene, and comfort, they also present biomechanical limitations that must be carefully considered.
Aligner therapy relies on shape-molding, where the geometry of the aligner creates controlled forces to move teeth. Despite advancements in materials and digital treatment planning, aligners are constrained by the fixed flexural rigidity of the material, which limits force predictability and consistency. Unlike fixed appliances, whose force systems can be adjusted dynamically, aligners operate within a more restricted biomechanical framework and suffer from rapid force degradation due to material fatigue.1
A key challenge is controlling complex root movements, such as torque and bodily translation. Fixed appliances, particularly nickel-titanium wires, maintain consistent energy transfer, making them more effective for root positioning and space closure. In contrast, aligners experience a significant decline in force delivery within days of wear. Fixed appliances allow for nuanced adjustments (eg, wire bending and torque additions), providing greater control over tooth movements, which is challenging to replicate with aligners.1 Comparing the two modalities highlights key mechanical differences.
Treatment Outcomes
Previous studies have identified clear aligner therapy as an adequate alternative for treatment compared to fixed orthodontics in nongrowing patients with mild to moderate malocclusions and nonextraction protocols.2 When comparing patients of varying degrees of overbite, Khosravi et al3 reported that aligner therapy maintained overbite in patients with normal pretreatment overbite, reduced overbite by 1.5 mm on average for open bite cases, and provided 1.5 mm of bite opening in deep bite cases without significant changes in the vertical dimension or mandibular plane angle. This study served to discredit the claim that the thickness of the aligner material interferes with freeway space and contributes to a posterior bite block effect.3
The literature reflects roughly a 50% discrepancy between predicted and clinical outcomes with clear aligner therapy, ultimately requiring multiple rounds of refinement. This can be attributed to differences in point of force application, intrinsic properties of the aligner material, and the “watermelon seed effect.” Orthodontists have also reported that between 70% and 80% of their patients require a mid-course correction with aligner treatment, some of which convert to fixed appliances altogether.1 Rajan et al4 found a clinically significant shortfall in the ability of aligners to express torque in maxillary central incisors when greater than 10° of lingual root torque was planned in the three-dimensional simulation of teeth’s predicted movement. The changes in torque were less than half of what was prescribed, and this was not influenced by the inclusion of power ridges or aligner change protocol. Therefore, regarding virtual treatment planning with clear aligner therapy, providers should consider overcorrection of certain aspects of the malocclusion to obtain desired outcomes, particularly when torque changes are desired.
In deep bite cases, Dianiskova et al,5 reported the mean curve of spee (COS) leveling accuracy from clear aligners to be 62%, and the mean overbite reduction accuracy as 61%. In other words, clear aligner therapy had a moderate accuracy in achieving intended programmed movements for COS leveling and overbite reduction.5,6
Furthermore, Djeu et al7 compared treatment outcomes for patients treated with clear aligner therapy and fixed appliances and found that the aligner group scored 13 points higher on the American Board of Orthodontists grading system, subsequently resulting in a 27% lower passing rate. The greatest discrepancy in scores were associated with posterior torque, occlusal contacts, overjet, and sagittal molar relationship. Similarly, a study by Kravitz et al8 reported the accuracy of tooth movement with clear aligner therapy to be 41%, emphasizing the need to be aware of this therapy’s limitations and importance of case selection.
The above studies emphasize the need for adequate case selection for aligner therapy, as well as overcorrection when planning clear aligner cases with complex movements such as torque or deep bite correction. Overcorrection refers to the provider adding additional movements into the aligner setup, such as torque or curve of spee leveling, beyond what would be needed for traditional braces, to ensure the aligner expresses the desired tooth movement.
Treatment Time
When discussing length of treatment, the answer is not clear whether aligner therapy or traditional braces result in shorter treatment times. However, the literature shows that several factors can account for treatment time discrepancies, which may sway the clinician to prefer one over the other in certain circumstances. One study, for instance, found that clear aligner therapy might lengthen treatment time for complex cases compared to fixed appliances; however, aligner therapy might be able to treat mild, nonextraction cases faster.2 On the other hand, a systematic review by Alam et al9 found that fixed appliances and aligner therapy had comparable overall efficacy in inducing orthodontic tooth movement, but noted a significant reduction in treatment time for aligner therapy.
What has been shown consistently is the importance of estimating patient compliance. The use of fixed appliances is largely in the control of the orthodontist, allowing for constant and continuous force around the clock. The typical wear-protocol for clear aligner therapy is 22 hours per day for patients to allow for adequate time with appropriate force application. Thus, the use of clear aligners requires increased patient compliance to achieve desired treatment outcomes.
With appropriate case selection and a compliant patient, the chances of achieving desired tooth movement increases. Additionally, as described by Borda et al,10 clear aligner therapy showed a decrease in emergency visits and in number of appointments compared to fixed appliances in treating teenage populations with mild malocclusions, resulting in an average treatment duration of 16.9 months for clear aligners versus 23.4 months for fixed appliances (mean DI of 11.9).
Patient-Reported Outcomes
In assessing patient-reported outcomes, Cardoso et al,11 reported that during the first few days of treatment, patients treated with clear aligner therapy felt lower levels of pain than those treated with fixed appliances. However, after the initial treatment period and up to 3 months, no differences were noted between the two treatment modalities. White et al12 agreed with these findings, and added that discomfort with fixed appliances occurred after the first and second adjustments, and peaked between the first and third day following treatment, especially while eating.
Relapse
Regardless of the orthodontic appliance used, retention should be a key aspect of the treatment plan, allowing patients to maintain their dentition’s alignment, function, and health for life. Accordingly, the implementation of post-treatment retention protocols is essential for both clear aligner therapy and fixed appliances.
Previous studies have compared the differences in retention outcomes for patients treated with clear aligner therapy vs fixed braces. Kuncio et al13 looked at post-treatment outcomes for patients treated with clear aligner therapy and conventional fixed appliances using the same retention protocol: 6 months of full-time Essix retainer wear followed by nightly use for at least 6 additional months. Authors found that patients using both appliances experienced similar decreases in total alignment and mandibular anterior alignment. Interestingly, the clear aligner group demonstrated more relapse in the maxillary anterior region.13
Root Resorption
Root resorption is a critical concern in all orthodontic treatment modalities, including fixed appliances and clear aligner therapy. Apical root resorption, the most common form, involves the irreversible loss of hard tissue at the root apex during orthodontic movement.14 Advances in cone-beam computed tomography (CBCT) have enhanced the assessment of root resorption, allowing for more precise comparisons between clear aligners and fixed appliances. Research indicates a lower prevalence and reduced severity of apical root resorption in patients treated with clear aligners vs conventional brackets and archwires.15 A systematic review and meta-analysis further confirmed that, when controlling for variables such as age, malocclusion classification, and treatment plan, clear aligners were associated with a lower incidence of resorption.16 These findings have led some clinicians to prefer aligners for patients with a history of root resorption or a predisposition to this complication.
The reduced risk of root resorption with aligners is attributed to their force application. Unlike fixed appliances, which exert continuous forces through archwire engagement, aligners deliver lighter, more controlled, and intermittent forces due to their removability for eating and oral hygiene.17,18 This intermittent force may facilitate periods of cemental repair, reducing cumulative resorption risk.19 Additionally, aligners exert less torque and intrusive forces, factors implicated in root resorption pathogenesis.
Despite promising evidence, orthodontists must interpret these findings cautiously. Individual factors, including genetic predisposition, root morphology, treatment duration, and force magnitude, play crucial roles. As clear aligner protocols evolve, further long-term CBCT and histological studies are needed to clarify root resorption mechanisms across treatment modalities. A comprehensive understanding of risk factors will enable clinicians to tailor treatment plans, optimizing both esthetic and functional outcomes while preserving long-term dental integrity.
Periodontium
The intersection of orthodontics and periodontics highlights the need for an interdisciplinary approach to treatment planning, particularly for patients with periodontal compromise. Orthodontic forces impact the periodontium, and failure to consider these effects may lead to exacerbation of periodontal diseases, attachment loss, or gingival recession.20 With a growing number of adults seeking orthodontic care, many with pre-existing periodontal conditions, understanding the biomechanical and biological implications of different appliances is essential for optimizing both short-term success and long-term stability.
Systematic reviews and meta-analyses have compared the periodontal effects of clear aligners and fixed appliances, evaluating parameters such as probing depths, plaque index, gingival index, bleeding on probing, and gingival recession. One found statistically significant advantages for clear aligners, including lower plaque index scores, improved gingival index scores, and shallower probing depths over time. At all measured intervals, aligner patients exhibited less gingival recession and reduced bleeding on probing compared to those treated with fixed appliances.21
These differences are attributed primarily to the removable nature of clear aligners, which facilitate superior oral hygiene compared to fixed appliances, where brackets, bands, and archwires create bacterial retention sites. The absence of ligatures in aligner therapy further reduces the risk of periodontal inflammation. Additionally, aligners apply intermittent forces, potentially allowing for periodontal recovery and repair, whereas continuous forces from fixed appliances may exacerbate inflammation, particularly in patients with thin periodontal biotypes.17 Clear aligners also enable more controlled and gradual tooth movements, potentially minimizing disruption to the periodontal ligament and inflammatory response.
While evidence suggests that clear aligners may offer periodontal benefits, further high-quality, randomized clinical trials are needed to confirm these findings. Existing studies vary in design, patient populations, and assessment methods, necessitating cautious interpretation. Orthodontists should adopt a case-by-case approach, considering individual periodontal health, oral hygiene capabilities, and overall treatment goals.
Periodontal considerations should be central to orthodontic treatment planning, particularly for patients with compromised periodontal health. Emerging evidence supports clear aligners as a potentially advantageous option for maintaining periodontal stability, reinforcing the importance of collaborative treatment planning between orthodontists and periodontists. Such coordination ensures treatment aligns with both orthodontic and periodontal objectives, optimizing long-term oral health while achieving functional and esthetic goals.
Caries
White spot lesions (WSLs) are a significant concern when selecting the type of orthodontic appliance for treatment. These lesions appear as opaque, white areas on the tooth surface and represent early-stage enamel demineralization, an initial sign of caries development. Numerous studies have investigated the prevalence of WSLs in patients undergoing treatment with both fixed appliances and clear aligners, employing photographic analysis and light-induced fluorescence imaging. The prevailing consensus in the literature is that fixed appliance therapy is associated with a higher incidence of WSLs.22-24 This is largely attributed to the challenges fixed appliances pose for oral hygiene, including restricted access for brushing and flossing, and an increased number of plaque-retentive areas around brackets and wires.
According to a study by Azeem et al,24 approximately 46% of patients treated with fixed appliances develop WSLs within the first year, whereas only 2.85% of aligner patients experience the same. Similarly, a study by Buschang23 reported WSLs in just 1.2% of aligner patients, compared to 26% of those receiving conventional fixed treatment. Given these findings, aligner therapy should be considered — especially for patients with elevated caries risk — as it appears to offer a significantly reduced likelihood of WSL development.
Conclusion
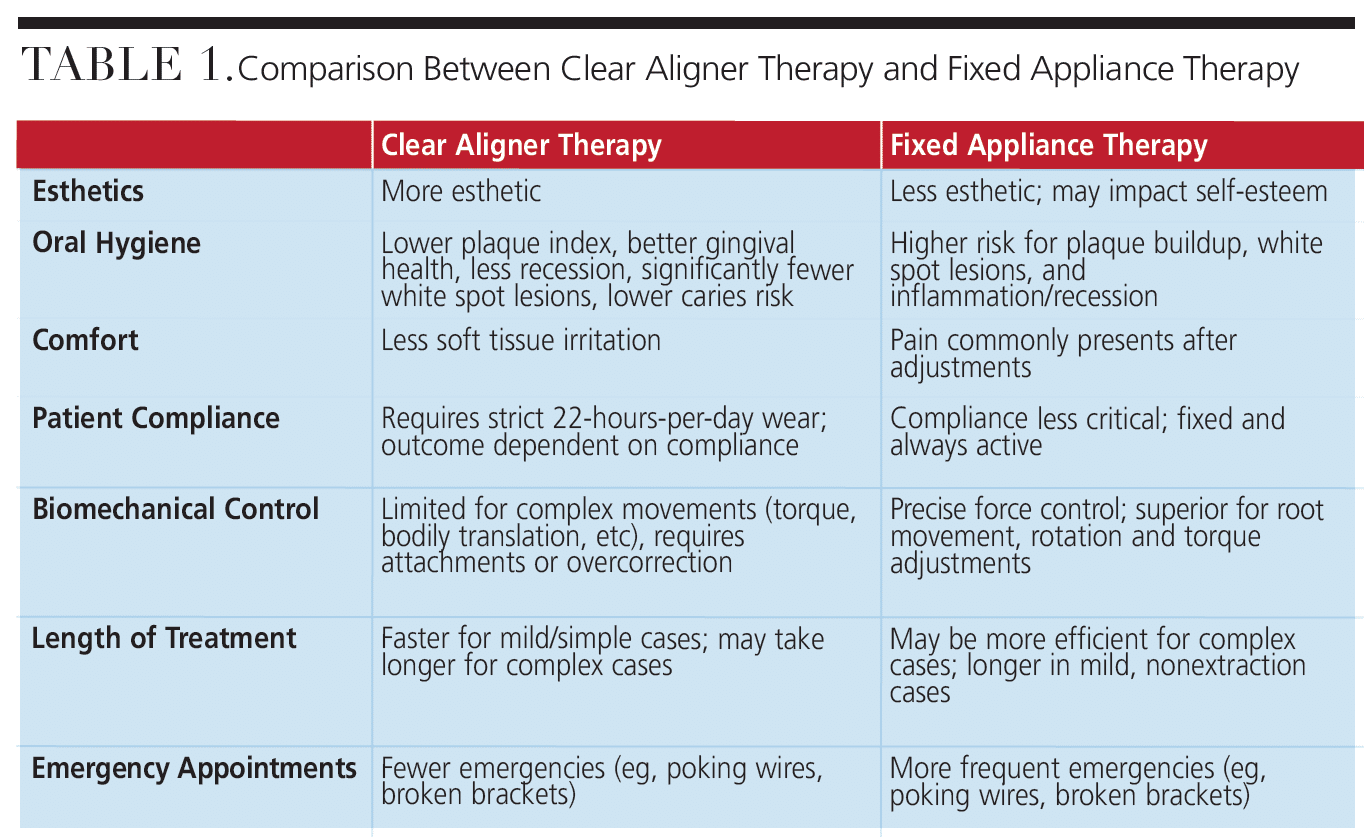
Clear aligners and fixed appliances each have distinct advantages and limitations, making case selection and individual patient needs crucial in treatment planning. As summarized in Table 1, clear aligners offer better esthetics, oral hygiene, and comfort, but are less effective for complex tooth movements and require strict patient compliance. Fixed appliances, on the other hand, provide superior biomechanical control and predictability, especially in complex cases, but are more visible and harder to keep clean. Clinicians need to keep all these factors in mind when deciding on treatment modality type for each orthodontic patient.
References
- Upadhyay M, Arqub SA. Biomechanics of clear aligners: hidden truths & first principles. J World Fed Orthod. 2022;11:1:12–21.
- Papadimitriou A, Mousoulea S, Gkantidis N, & Kloukos D. Clinical effectiveness of Invisalign® orthodontic treatment: a systematic review. Prog Orthod. 2018;19:37–24.
- Khosravi R, Cohanim B, Hujoel P, et al. Management of overbite with the Invisalign appliance. Am J Orthod Dentofacial Orthop. 2017;151:691-699.
- Rajan N, Weir T, Meade MJ. Efficacy of planned moderate to severe torque changes in maxillary central incisors with the Invisalign appliance: A retrospective investigation. Am J Orthod Dentofacial Orthop. 2024;166:375–383.
- Dianiskova S, Rongo R, Sirignano D, et al. Assessment of clinical predictability of overbite reduction and curve of spee levelling in clear aligner treatment. Orthod Craniofac Res. 2025;28:458-465.
- Rossini G, Parrini S, Castroflorio T, Deregibus A, Debernardi CL. Efficacy of clear aligners in controlling orthodontic tooth movement: a systematic review. Angle Orthod. 2015;85:881-889.
- Djeu G, Shelton C, Maganzini A. Outcome assessment of Invisalign and traditional orthodontic treatment compared with the American Board of Orthodontics objective grading system. Am J Orthod Dentofacial Orthop. 2005;128:292-298.
- Kravitz ND, Kusnoto B, BeGole E, Obrez A, Agran B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am J Orthod Dentofacial Orthop. 2009;135:1:27–35.
- Alam MK, Awawdeh M, Alhazmi N, et al. A systematic review of interventions-does Invisalign move teeth as effectively as orthodontic fixed appliances? Sci Cairo. 2024;1:4268902.
- Borda AF, Garfinkle JS, Covell DA, Wang M, Doyle L, Sedgley CM. Outcome assessment of orthodontic clear aligner vs fixed appliance treatment in a teenage population with mild malocclusions. Angle Orthod. 2020;90:485–490.
- Cardoso PC, Espinosa DG, Mecenas P, Flores-Mir C, Normando D. Pain level between clear aligners and fixed appliances: a systematic review. Prog Orthod. 2020;21:3.
- White DW, Julien KC, Jacob H, Campbell PM, Buschang PH. Discomfort associated with Invisalign and traditional brackets: A randomized, prospective trial. Angle Orthod. 2017;87:801–808.
- Kuncio D, Maganzini A, Shelton C, Freeman K. Invisalign and traditional orthodontic treatment postretention outcomes using the American Board of Orthodontics objective grading system. Angle Orthod. 2007;77:864-869.
- Baumrind S, Korn EL, Boyd RL. Apical root resorption in orthodontically treated adults. Am J Orthod Dentofacial Orthop. 1996;110:311-320.
- Li Y, Deng S, Mei L, et al. Prevalence and severity of apical root resorption during orthodontic treatment with clear aligners and fixed appliances: a cone beam computed tomography study. Prog Orthod. 2020;21:1.
- Fang X, Qi R, Liu C. Root resorption in orthodontic treatment with clear aligners: A systematic review and meta-analysis. Orthod Craniofac Res. 2019;22:259-269.
- Acar A, Canyürek U, Kocaaga M, Erverdi N. Continuous vs. discontinuous force application and root resorption. Angle Orthod. 1999;69:159-164.
- Levander E, Malmgren O, Eliasson S. Evaluation of root resorption in relation to two orthodontic treatment regimes. A clinical experimental study. Eur J Orthod. 1994;16:223-228.
- Ballard DJ, Jones AS, Petocz P, Darendeliler MA. Physical properties of root cementum: part 11. Continuous vs intermittent controlled orthodontic forces on root resorption. A microcomputed-tomography study. Am J Orthod Dentofacial Orthop. 2009;136;1:1-9.
- Gkantidis N, Christou P, Topouzelis N. The orthodontic-periodontic interrelationship in integrated treatment challenges: a systematic review. J Oral Rehabil. 2010;37:377-390.
- ElNaghy R, Al-Qawasmi R, Hasanin M. Does orthodontic treatment using clear aligners and fixed appliances affect periodontal status differently? Evid Based Dent. 2023;24:73-74.
- Rouzi M, Zhang X, Jiang Q, Long H, Lai W, Li X. Impact of clear aligners on oral health and oral microbiome during orthodontic treatment. Int Dent J. 2023;73:603–611.
- Buschang PH, Chastain D, Keylor CL, Crosby D, Julien KC. Incidence of white spot lesions among patients treated with clear aligners and traditional braces. Angle Orthod. 2019;89:359-364.
- Azeem M, Hamid WU. Incidence of white spot lesions during orthodontic clear aligner therapy. Journal of the World Federation of Orthodontists. 2017;6(3):127-130.
From Decisions in Dentistry. October/November 2025;11(5):32-35.

