
Choosing Between Fixed and Removable Prostheses
Timothy A. Hess, DDS, MAGD, discusses clinical considerations when developing treatment plans for appliance-based restorative care.
Timothy A. Hess, DDS, MAGD, discusses clinical considerations when developing treatment plans for appliance-based restorative care
Editor’s Note: The views expressed in this interview are the author’s.
Edentulous or terminal dentition patients are present in most dental practices. General practitioners and specialists are often asked to provide options and treatment for these individuals. This process begins by determining the types of prosthetic therapies that are possible, based on evaluations of the patient’s teeth, bone and soft tissues. Due to the variety of options and complexity of these types of prosthetics, as well as possible biological consequences (such as removal of significant supporting bone), a detailed consultation and informed consent are needed before initiating treatment.
With these considerations in mind, Decisions in Dentistry asked Timothy A. Hess, DDS, MAGD, of the University of Washington School of Dentistry in Seattle to share his perspectives on factors affecting the choice between fixed or removable prostheses for implant-supported restorations.
Where does the clinician start when planning an implant-supported prosthetic case?
Simply stated, with the maxillary arch. Recently, Ricardo Mitrani, DDS, MSD, and Jack Goldberg, DDS, MS, introduced the Lip-Tooth-Ridge concept for diagnosing edentulous patients, establishing risk and providing effective therapy (article in press). In my estimation, this well-thought-out concept also has application when assessing terminal dentition patients. Unfortunately — and all too often — clinicians fail to develop an appropriate treatment plan for full-arch restorations using fixed, fixed removable or removable prostheses. This can lead to esthetic and functional failures, requiring innovative solutions from laboratory technicians to “save” the case.
Restoring clinicians need to use a logical and sequential approach to treatment planning. Educators, such as Robbins, Rouse, Spear, Kois and others,1–7 have suggested planning protocols that start with the position of the anterior six teeth from an esthetic standpoint. These protocols consider static and dynamic lip movement, and subsequently build the posteriors and opposing mandibular arch in harmony — esthetically and functionally — with the anterior six. A helpful guideline for positioning the incisal edge comes from a study by Misch8 in which he used the canine as the guide to set the incisal edge, and therefore the incisal plane. He found that, on average, the edge of the canine falls within 1 mm of the maxillary lip line in repose with few outliers. This is particularly useful for female patients, who often show more varied upper lip anatomy (both in length and shape) than male patients.
Special attention must be paid to lip mobility when planning the finish line of a fixed removable prosthesis. On average, the lip moves from 6 to 8 mm, and the hypermobile lip moves even more. If the restoring dentist does not take lip movement into account, it can result in an esthetic failure in which the transition line between the prosthesis and gingiva is clearly visible. Another possible failure is when the lip becomes trapped on the flange in an elevated position. In these cases, the only solution acceptable to the patient may be the use of botulinum toxin-A to reduce lip movement; on average, movement can be reduced by 5 mm with botulinum toxin-A.9,10
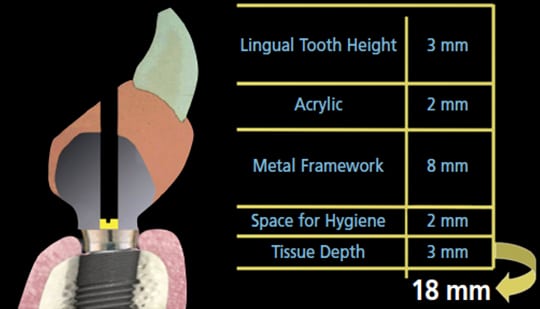
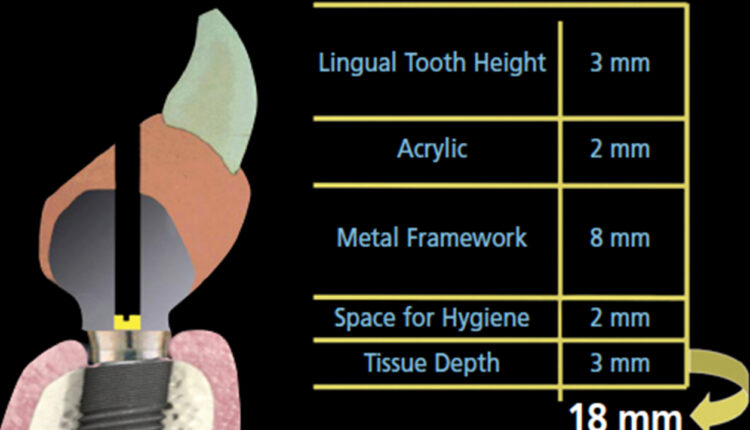
A common error in treatment planning is failing to ensure adequate space for the prostheses. Phillips and Wong11,12 outlined space requirements for fixed removable, as well as bar-and-clip, prosthetics. In 2002, the fixed removable hybrid prosthesis (FRHP) had a cast framework, and their recommendation for 18 mm in the anterior is based on a screw-access hole in the cingulum of these anterior teeth (Figure 1). Although 18 mm is a good guideline, it can be reduced with the advent of more streamlined, milled titanium frameworks. The restoring clinician should have a conversation with the laboratory technician in order to understand exactly how much space the technician needs to provide an esthetic and functional prosthesis with adequate strength.
What are the indications for use of an implant-supported fixed prosthesis in the maxilla?
If the patient has only a defect of tooth structure, the clinician can consider fixed metal/ceramic or fixed zirconia restorations. While the connector size will need to be at least 7 mm (depending on the material selected), even that may prove inadequate. In addition, these restorations may not satisfy some patients’ esthetic demands if the gingival architecture is flat and tooth-colored porcelain or composite must be added to create papilla and the appearance of a gingival scallop. Traditionally, the biggest drawback of a fixed prosthesis is cost — but even though an FRHP may be a less costly alternative, it comes with a potential biologic compromise (namely, bone).
Depending on the implant manufacturer, FRHPs are marketed under a variety of names. All basically use a concept of four implants placed and loaded immediately, with abutments to connect a modified denture based on the success of Branemark et al13 and, more recently, Malo et al14 and Lopes et al.15
A word of caution: It is common for general practitioners to think that because they restore single and multiple implants on a regular basis they have the skill set to perform implant-based denture procedures. The FRHP procedure is a denture-driven treatment and requires experience and skill in fitting, fabrication and repair of complete dentures.
Why choose a fixed removable hybrid rather than a zirconia prosthesis?
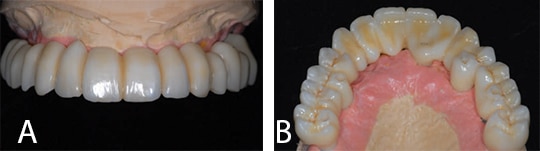
Although many clinicians prefer a prosthesis made entirely from zirconia (Figures 2A and 2B), use of this material raises its own set of considerations. Briefly, concerns regarding a full zirconia prosthesis include: 1) chipping of layered porcelain (if present) due to differing coefficients of thermal expansion; 2) uncertainty of the actual flexural strength and fatigue toughness of the zirconia framework based on possible failure to follow recommended firing cycles; 3) concern regarding multilayered zirconia frameworks chipping due to the percentage of cubic versus tetragonal zirconia in the layers; 4) difficulty creating realistic colors of gingiva and translucency; and 5) cost of fabrication and repair.
Today, the classic FRHP is a milled titanium bar wrapped with denture acrylic with denture teeth. Advantages include fabrication expense, the ability to repair broken teeth or acrylic, abundant choices in denture teeth from a cosmetic, wear and cost standpoint, and esthetic options to mimic the color of the gingiva with acrylic (Figure 3).
One engineering concept to consider is an FRHP system’s “sacrificial” component. It could be argued that in an FRHP fabricated with acrylic and denture teeth, the latter are the sacrificial components. The question becomes: When fabricating a prosthesis, is it not better to control where the failure occurs with time? After all, a failing or broken implant or abutment is more difficult to repair than a piece of plastic. By the same token, if a zirconia prosthesis chips or fractures, the only option is the costly replacement of the entire prosthesis.

What are the indications for use of an implant-supported removable prosthesis in the maxilla?
There are two primary indications for removable prostheses: inadequate lip support due to horizontal loss of maxillary bone (requiring a buccal flange), and lip dynamics that would produce an unfavorable esthetic result due to the position of the junction of the prosthesis and soft tissues.
In the first situation, a removable implant-supported prosthesis is warranted because the bone and soft tissues are deficient. In this case, a buccal flange is created to replace the missing structures; in addition, the appliance must be removable for hygiene. Considering the recommendations of Phillips and Wong,11,12 if 11 to 12 mm of vertical space exists, clinicians can utilize a telescopic-type attachment. However, if the ridge defect also includes a significant vertical component, the practitioner should consider a bar-and-clip overdenture — in which case 15 mm of space is required.
An additional consideration are patients who have not experienced horizontal loss of maxillary bone, but are simply unhappy with their lip support. If an evaluation of incisal edge position and tooth angulation indicates the deficiency is in the soft tissues of the lip, the clinician must be cautious about fabricating a prosthesis that creates an unnatural projection of the maxillary arch. Instead, soft tissue augmentation with dermal fillers may be warranted. The timing of any dermal filler placement should be discussed with the surgeon in order to determine whether it should occur before or after delivery of the final prosthesis.
In the second scenario — in which lip dynamics pose a risk of creating an unesthetic result — a removable prosthesis with a buccal flange should be considered. Another option would be a reduction of bone to change the position of the junction. However, this comes at the biological cost of bone — which the patient may not be receptive to, or that is not possible based on the need for adequate bone to support the implants.
What is the role of advanced digital technologies, including computer aided design/computer aided manufacturing (CAD/CAM), in fixed or removable prosthetic treatment?
Although some might assume the answer would focus on milled, full-arch prostheses, CAD/CAM and other digital technologies play a bigger role than merely creating the final restoration. Cone beam computed tomography (CBCT), for example, allows the restoring dentist and surgeon to evaluate possible sites for implant placement. In some cases, guides for fully guided surgeries can be created utilizing the CBCT information and merging with scans of models or scans created intraorally.
Intraoral scans work well in terminal dentition cases in which adequate hard tissue (i.e., tooth structure) remains. Although the clinical ability to create accurate intraoral scans of soft tissues — and recording the displaceability of such tissue — may not be ideal at this point, scanning technology is improving.16,17 Nevertheless, many clinicians still prefer to make a conventional impression for an immediate complete denture (ICD) and scan the model created. Some may argue that because the ICD is being converted, complete accuracy of the intaglio surface is unnecessary and an intraoral scan is adequate. But if the case cannot be loaded immediately, it is likely the ICD will have to be relined due to bone reduction that may have occurred. The surgeon and restoring dentist need to communicate how much bone reduction is needed to obtain sufficient space for the final prosthesis. The restoring dentist should fabricate the surgical guide. If possible, the restorative dentist should be present the day of surgery to verify bone reduction, the anterior-posterior spread of implants, attachment of angled abutments in the correct position, and convert the ICD to an interim FRHP.
Implant design software can be used to plan implant placement, which will also allow fabrication of surgical guides. These can be milled using CAM technology or printed with a three-dimensional printer. Many clinicians believe that fully guided surgery is unnecessary, impractical and unduly expensive. An alternative is to create a basic surgical guide by duplicating the ICD and fabricating the guide in orthodontic resin (Figure 4). Pressed firmly against the palate, it provides a measure of bone reduction for the surgeon, and a basic trough to guide placement of the implants and their corresponding abutments.

Perhaps the best use of CAD/CAM in FRHP treatment is fabrication of milled titanium bar frameworks, which tend to be stong, light and extremely accurate.18,19 Ultimately, the rapid development of CAD/CAM dentures looks to improve the process for both the patient and clinician. Early adopters may have been frustrated with the unrealized promise of “two-visit” dentures. With the introduction of a try-in step with most systems, however, clinical results have improved to the point both clinicians’ and patients’ expectations are being met. Currently, the merging of CAD/CAM dentures with milled titanium bars is in its infancy, but this is a positive development in creating economical, esthetic FRHPs that are easily repairable.
Any final thoughts?
While choosing an FRHP can be a reasonable option from both the clinician’s and patient’s perspective, each needs to understand the available treatment options — as well as advantages and disadvantages of each therapeutic approach. Ultimately, before attempting to restore a complex implant-supported prosthetic case, if the clinician does not have a strong prosthodontic background, he or she should consider additional training, supervision by a qualified mentor, or referral to a prosthodontist.
REFERENCES
- Robbins JW, Rouse JS. Global Diagnosis: A New Vision of Dental Diagnosis and Treatment Planning. Hanover Park, IL: Quintessence Publishing Co, Inc.; 2016.
- Spear F. Diagnosing and treatment planning inadequate tooth display. Br Dent J. 2016;221:463–472.
- Spear F. Too much tooth, not enough tooth: making decisions about anterior tooth position. J Am Dent Assoc. 2010;141:93–96.
- Tak On T, Kois JC. Digital smile design meets the dento-facial analyzer: optimizing esthetics while preserving tooth structure. Compend Contin Educ Dent. 2016;37:46–50.
- Simeone P, Leofreddi G, Kois JC. Managing severe periodontal esthetic challenges: the restorative-surgical connection. Int J Periodontics Restorative Dent. 2016;36:83–93.
- Kois DE, Kois JC. Comprehensive risk-based diagnostically driven treatment planning: developing sequentially generated treatment. Dent Clin North Am. 2015;59:593–608.
- Kois JC, Filder BC. Anterior wear: orthodontic and restorative management. Compend Contin Educ Dent. 2009;30:420–422,424,426–429.
- Misch CE. Guidelines for maxillary incisal edge position — a pilot study: the key is the canine. J Prosthodont. 2008;17:130–134.
- Polo M. Botulinum toxin type A (Botox) for the neuromuscular correction of excessive gingival display on smiling (gummy smile). Am J Orthod Dentofacial Orthop. 2008;133:195–203.
- Suber JS, Dinh TP, Prince MD, Smith PD. OnabotulinumtoxinA for the treatment of a “gummy smile.” Aesthet Surg J. 2014;34:432–437.
- Phillips K, Wong KM. Vertical space requirement for the fixed-detachable, implant-supported prosthesis. Compend Contin Educ Dent. 2002;23:750–752,754,756.
- Phillips K, Wong KM. Space requirements for implant-retained bar-and-clip overdentures. Compend Contin Educ Dent. 2001;22:516–518,520,522.
- Branemark PI, Svensson B, van Steenberghe D. Ten-year survival rates of fixed prostheses on four or six implants ad modum Branemark in full edentulism. Clin Oral Implants Res. 1995;6:227–231.
- Malo P, de Araujo Nobre M, Lopes A, Moss SM, Molina GJ. A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up. J Am Dent Assoc. 2011;142:310–320.
- Lopes A, Malo P, de Araujo Nobre M, Sanchez-Fernandez E. The NobelGuide All-on-4 treatment concept for rehabilitation of edentulous jaws: a prospective report on medium– and long–term outcomes. Clin Implant Dent Relat Res. 2015;Suppl 2:406–416.
- Lee J-H. Improved digital impressions of edentulous areas. J Prosthet Dent. 2017;117:448–449.
- Kim JE, Kim NH, Shim JS. Fabrication of a complete, removable dental prosthesis from a digital intraoral impression for a patient with an excessively tight reconstructed lip after oral cancer treatment: a clinical report. J Prosthet Dent. 2017;117:205–208.
- Pozzi A, Tallarico M, Moy PK. Four-implant overdenture fully supported by a CAD-CAM titanium bar: A single-cohort prospective 1-year preliminary study. J Prosthet Dent. 2016;116:516–523.
- Zitzmann NU, Marinello CP. A review of clinical and technical considerations for fixed and removable implant prostheses in the edentulous mandible. Int J Prosthodont. 2002;15:65–72.
The author wishes to thank Keith M. Phillips, DMD, MSD, CDT, FACP, Darrin A. Rapoport, BDS, MSD, Ricardo Mitrani, DDS, MSD, and Jack Goldberg, DDS, MS, for their assistance with this perspective.
The author reports that he has previously been compensated for lectures by Nobel Biocare and Straumann, and provides uncompensated product reviews for Komet USA and Sagemax Bioceramics.
From Decisions in Dentistry. April 2017;3(4):29–31.
