
 HIDESY/ISTOCK/GETTY IMAGES PLUS
HIDESY/ISTOCK/GETTY IMAGES PLUS
Caring for Patients With Autism Spectrum Disorder
The following strategies will prove helpful when caring for patients with autism spectrum disorder.
PURCHASE COURSE
This course was published in the February 2020 issue and expires February 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the February 2020 issue and expires February 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify behaviors associated with autism spectrum disorder (ASD), and the impacts of this developmental condition on access to dental treatment and the provision of care.
- List clinical strategies that can be helpful when treating patients with ASD.
- Explain the typical onset timing of ASD symptoms, and why evidence-based techniques can help support successful patient behavior during dental visits.
Autism spectrum disorder (ASD) is a complex developmental condition that involves persistent difficulties with social interaction and communication, restrictive interests and repetitive behaviors.1 The effects of ASD and severity of symptoms are different in each individual,2 as ASD describes a spectrum of neurodevelopmental functioning.3 Symptoms typically appear in the first two years of life, and the prevalence is estimated at 1 in 59 children, with males four times more likely to be impacted than girls.1
Autism has specific persistent challenges, and one of the areas of atypical presentation relates to social communication. These challenges may present as difficulties with interactions — such as back and forth conversation, nonverbal communication, eye contact, expressing emotional states, and not understanding the point of view of another person.1,2 Thus, gaining information about oral health may be more challenging when assessing a patient’s oral health care needs, comfort level, and feelings of anxiety regarding treatment.
Another area of atypical presentation in individuals with autism relates to sensory characteristics. Patients with ASD may experience central nervous system dysfunction that impacts sensory perceptions; consequently, the individual may demonstrate hypo- or hypersensitive responses. For example, hyposensitive responses may be characterized by under-responsivity — meaning, the patient will require a larger amount of sensory input to engage. This may manifest as not responding to a name or greeting, or providing low indications of discomfort during caries preparation procedures. On the other hand, hypersensitive responders may show high levels of sensitivity to relatively benign sensory experiences — lights and touch might feel overwhelming and unwelcome, for instance, or the sounds of instruments and handpieces may prove unbearable.3 Oral health professionals who are aware of the patient’s sensory profile may be able to provide more effective support.
In addition to social communication and sensory challenges, a final area of atypical presentation may involve an individual with autism exhibiting behavior characteristics, such as restrictive and repetitive patterns of behaviors, interests or activities. Examples of repetitive motor movements include hand flapping, toe walking and speaking in atypical pitches,2,4 while specialized interests may include topics such as trains or computers. Understanding a patient’s specialized interests and propensity for enacting specific behaviors can help guide the dental team’s approach before and during treatment.
DENTAL TREATMENT PATTERNS
Patients with autism often require adapted dental treatment to meet their oral health needs.5 Specific challenges may occur in the dental setting due to disruptive behaviors resulting from fear and anxiety. As a result, pharmacological sedation may be necessary, ranging from minimal sedation (achieved through oral, transmucosal or inhalation anxiolysis) to deeper forms of sedation and general anesthesia.5 Various sedative agents (used alone or in combination) are suggested, and commonly include nitrous oxide, diazepam, hydroxyzine chlorhydrate, alphaprodine chlorhydrate and prometazine hydrochloride.6 Intravenous conscious sedation may be necessary for patients with autism who have reduced ability to cope with dental procedures.7 Although this method is common in the literature, the success of its implementation is limited.6 The administration of nitrous oxide requires a certain level of communication with the patient, which, considering the social communicative challenges, can be difficult to achieve in patients with ASD.6 In turn, this can complicate successful sedation and potentially do nothing to improve the patient’s ability to cooperate.7
Although current dental curriculum encourages the implementation of sedative agents as a form of support for patients with autism, such curriculum is not tailored to address the increased anxiety this patient population may possess. Approximately 40% of children diagnosed with autism exhibit anxiety disorders that can exacerbate deficits in communication and socialization, while increasing inappropriate behaviors.8 Therefore, dental teams may automatically assume implementing sedative agents is the best course of treatment; however, this approach may have adverse effects, such as nausea, vomiting and obstruction of the superior respiratory conducts.8
BARRIERS TO CARE
Research has substantiated specific barriers that individuals with autism experience in the dental setting.5,6,8–13 Three main themes in the research indicate that limited access to clinicians, communication difficulties, and internalizing behavior had adverse impacts on accessing dental care.
First and foremost, it can be difficult to find dentists and dental staff willing to care for this population.10 Many oral health professionals believe they lack the proper knowledge and training to treat these patients.11
Second, communication challenges limit the patient’s ability to express dental needs, such as indicating an area of pain.11 This also makes it difficult for patients to effectively communicate fears or concerns during treatment, which increases patient anxiety.8
Third, patients may exhibit externalizing and internalizing behaviors. While anxiety during dental exams is a common experience for many, it may be exacerbated in patients with ASD. Whether the dental visit is a novel or repeated experience, patients may have anxiety from a lack of understanding of what will happen during the appointment. They may also fear the discomfort from associated noises, smells, taste and physical interactions. Dental handpieces, suction equipment, operatory lights and personal touch are all stimuli that can exaggerate sensitivities and make patients uncomfortable.8 Consequently, the special characteristics associated with autism — such as hypersensitivity — may contribute to exaggerated behavioral responses during treatment and impede cooperation.12
Problem behaviors make dental examinations difficult, prompting some dentists to consider sedation, physical restraint, or referral to a pediatric specialist.8 The stress associated with dental visits often prompts families to avoid or delay appropriate dental care.12 Furthermore, there is a strong relationship between the number of previous experiences of pain during dental treatments and dental anxiety,14 which indicates that many patients may arrive with heightened anxiety and face increased risk for behavioral problems.
SUCCESSFUL INTERVENTIONS
As the prevalence of ASD increases, more dental teams will encounter patients with ASD. These interactions necessitate an increase in autism-specific interventions that contribute to positive patient behavior. In turn, this will reduce anxiety among the patient, caregiver and dental team, resulting in a more positive visit. Interestingly, Weil and Inglehart13 found that only 32% of general dentists indicated an interest in treating patients with autism. One specific strategy to overcome a main barrier to dental treatment is training in the characteristics of autism (and how these characteristics relate to dentistry), and implementing evidence-based practices when planning and providing care.
Evidence-based practices are strategies that have met rigorous scientific criteria on the effectiveness of supporting individuals with ASD.15 Dental professionals can be trained in these practices so they have the tools and strategies to successfully care for patients with ASD — perhaps in conjunction with sedative agents or as an alternative to them. A wide variety of evidence-based practices can be utilized in dental settings to increase patients’ understanding and compliance during dental procedures. These practices not only increase the dental team’s ability to serve patients with ASD, they also may be used to eliminate or ease anxiety about visiting the dentist.
POSITIVE BEHAVIORAL SUPPORTS
Behavioral supports are research-based strategies that decrease problem behaviors by teaching new skills. In the context of dentistry, the aim is to reduce problem behaviors, such as anxiety and fight-or-flight behavioral responses. These supports are free and easy to implement. In addition, multiple supports can be used before and during treatment.
Priming: The use of priming allows a patient to preview or learn about a future event. Priming activities are typically short and involve a presentation of task materials — such as dental handpieces and instruments — to the patient to build familiarity.15,16 Prior to appointments, dental team members can recommend priming as a strategy to caregivers. Providing an opportunity for patients with high anxiety to visit the clinic, view the instruments and meet with dental staff before an appointment is an excellent way to prime.
Positive Stimulus Pairing: This occurs when a preferred stimulus (e.g., a favorite toy) is paired with a non-preferred stimulus (e.g., the dental provider). The association of a favorite toy with the clinician may reduce the patient’s anxiety about the dental visit. For example, when a patient enters the examination room, a favorite stuffed animal may be seated on the dental chair.16,17
Distraction: This technique involves focusing the patient’s attention on an item or action other than the dental procedure.18 Discussing or showing pictures of a preferred topic may distract the patient from the brief discomfort associated with the procedure.
Embedding Interests: This approach can help promote motivation and participation. The idea is that embedding the patient’s interests into the appointment will keep the child motivated to participate calmly.19 For example, if a patient loves trains, place a small train on the instrument table, talk about trains during the procedure, refer to a dental tool as “train toothbrush,” and draw a train on the patient’s paper bib.
Providing Choices: This technique allows patients with autism to have some control in the dental setting.20 This may be as simple as choosing the color of a toothbrush at the beginning of the appointment or deciding whether to give a high five or handshake. Choices can be simple and embedded into interactions multiple times during the exam.
Reinforcement: The use of reinforcement encourages behaviors conducive to successful dental visits.21 For example, if a patient is sitting calmly in the chair, praise the specific behavior, “Great job sitting with calm hands and body!” Patients can receive immediate reinforcement after a desired action, and can also receive delayed reinforcement, such as earning a favorite toy when treatment is complete.22 Figure 1 is an example of a visual reinforcement chart showing a preferred item that a patient may earn after a successful dental visit.

VISUAL SUPPORTS
Visual learning is a specific strength of individuals with ASD. Visual supports present verbal directions or information in a visual format and help increase comprehension of a situation. These supports typically include the exchange or display of images, drawings or photographs to represent tasks, needs, goals and rewards.23 Such supports help patients with autism understand, structure and predict activities in their daily lives.23
Video Modeling: This technique uses video recording to provide a visual model of the targeted behavior or skill.24 Video modeling may be used to demonstrate behaviors that are appropriate for the dental setting, such as sitting up in the chair and opening wide when asked by the dental professional. Examples can be found online and are effective when used before a dental visit so the patient knows what to expect and appropriate behavior during the appointment.
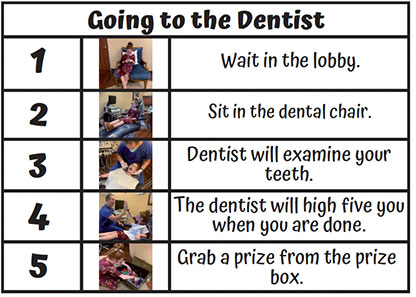
Visual Schedules: This tool shows the order of an event and can be created using words, pictures or objects. Such schedules act as a reminder for the patient of the day’s events, preparing the individual for activities and transitions that will occur during the visit.25 A visual schedule for a dental appointment lists the activities that will take place during the examination in chronological order. The patient has a visual structure of what will occur and when the appointment will end. Figure 2 provides an example of a visual schedule.
Social Stories: Designed to help individuals with autism understand and follow specified social protocol,26 social stories are individualized short stories that may increase appropriate social interactions by providing relevant components of a given situation.27 Specific to the dental setting, the social story may describe indirect, explicit language what happens at an appointment, specific behaviors that are expected, and connect positive reinforcement to a successful visit. This is a great strategy for priming the patient before the appointment; consequently, dental teams may wish to recommend that families use a social story prior to arriving.
Power Cards: The power card strategy teaches specific behaviors that can be used in a difficult situation, and should be paired with an individual’s special interests (an example is shown in Figure 3). Power cards can be used in conjunction with other visual supports, such as social stories, and can be helpful before and during the appointment.28 The cards, which can be any size, serve as visual reminders of how the patient should act in a given situation. The card introduces a specific scenario — in this case, a dental visit — with a visual cue. Easy to incorporate in the dental setting, power cards teach positive behavior and provide appropriate responses to challenging situations.

CONCLUSION
As the prevalence of individuals with ASD increases, the question is not if dental teams will encounter a patient with autism, but when. Although research demonstrates that patients with ASD face multiple barriers in accessing oral health care, practitioners can address these challenges by implementing evidence-based practices designed to improve oral health outcomes in this patient population.
The practices and strategies discussed in this article offer dental teams free, easy-to-implement tools that may be used to increase positive behavior, reduce stress, and promote communication when treating patients with autism.
REFERENCES
- U.S. Centers for Disease Control and Prevention. CDC. Data and Statistics, Autism Spectrum Disorders. Avaliable at: https://www.cdc.gov/ncbddd/autism/data.html. Accessed January 3, 2020.
- American Psychological Association. Autism Spectrum Disorder. Available at: https://www.apa.org/topics/autism/index. Accessed January 15, 2020.
- Charman T, Jones CR, Pickles A, Simonoff E, Baird G, Happé F. Defining the cognitive phenotype of autism. Brain Res. 2011;1380:10–21.
- Sasson NJ, Nowlin RB, Pinkham AE. Social cognition, social skill, and the broad autism phenotype. Autism. 2013;17:655–667.
- Lim MA, Borromeo GL. The use of general anesthesia to facilitate dental treatment in adult patients with special needs. J Dent Anesth Pain Med. 2017;17:91–103.
- Chandrashekhar S, Bommangoudar JS. Management of autistic patients in dental office: a clinical update. Int J Clin Pediatr Dent. 2018;11:219–227.
- Mawhinney RL, Hope A. Sedation for dental and other procedures. Anaesth Intensive Care Med. 2017;18:423–426.
- Elmore JL, Bruhn AM, Bobzien JL. Interventions for the reduction of dental anxiety and corresponding behavioral deficits in children with autism spectrum disorder. J Dent Hyg. 2016;90:111–120.
- Limeres-Posse J, Castaño-Novoa P, Abeleira-Pazos M, Ramos-Barbosa I. Behavioural aspects of patients with autism spectrum disorders (ASD) that affect their dental management. Med Oral Patol Oral Cir Bucal. 2014;19:e467–472.
- Norwood KW, Slayton RL. Oral health care for children with developmental disabilities. Pediatrics. 2013;131:614–619.
- Thomas A, Shetty P, Sowmya B, Kodgi V. Barriers to dental care for children with autism spectrum disorder — a pilot study. J Dent Med Sci. 2016;15:100–105.
- Isong IA, Rao SR, Holifield C, et al. Addressing dental fear in children with autism spectrum disorders: a randomized controlled pilot study using electronic screen media. Clin Pediatr (Phila). 2014;53;230–237.
- Weil TN, Inglehart MR. Dental education and dentists’ attitudes and behavior concerning patients with autism. J Dent Educ. 2010;74:1294–1307.
- Blomqvist M, Dahllöf G, Bejerot S. Experiences of dental care and dental anxiety in adults with autism spectrum disorder. Autism Res Treat. 2014;2014:238764.
- Schreibman L, Whalen C, Stahmer AC. The use of video priming to reduce disruptive transition behavior in children with autism. J Posit Behav Interv. 2000;2:3–11.
- Randall KR, Lambert JM, Matthews MP, Houchins-Juarez NJ. Individualized levels system and systematic stimulus pairing to reduce multiply controlled aggression of a child with autism spectrum disorder. Behav Modif. 2017;42:422–440.
- Byrne BL, Rehfeldt RA, Aguirre AA. Evaluating the effectiveness of the stimulus pairing observation procedure and multiple exemplar instruction on tact and listener responses in children with autism. Anal Verbal Behav. 2014;30:160–169.
- Giles A, Swain S, Quinn L, Weifenbach B. Teacher-implemented response interruption and redirection: training, evaluation, and descriptive analysis of treatment integrity. Behav Modif. 2018;42:148–169.
- Ninci JM. Embedded Interest Interventions for Individuals With Autism Spectrum Disorder: A Quality Review, Meta-Analysis, and Single-Case Research Evaluation. Available at: https://www.semanticscholar.org/paper/Embedded-Interest-Interventions-for-Individuals-A-Ninci/39ca18a605d4e379295 b42926a6e33be12e8d6f2. Accessed January 15, 2020.
- Rispoli M, Lang R, Neely L, et al. A comparison of within-and across-activity choices for reducing challenging behavior in children with autism spectrum disorders. J Behav Educ. 2013;22:66–83.
- Cividini-Motta C, Ahearn WH. Effects of two variations of differential reinforcement on prompt dependency. J Appl Behav Anal. 2013;46:640–650.
- Weston R, Hodges A, Davis TN. Differential reinforcement of other behaviors to treat challenging behaviors among children with autism: a systematic and quality review. Behav Modif. 2018;42:584–609.
- Yeganyan M. vSked: Designing and Evaluating An Interactive User Generated Content Driven Visual Scheduling System for Use in Classrooms for Children With Autism. Available at: https://www.learntechlib.org/ p/125429/. Accessed January 15, 2020.
- Cardon TA, Guimond A, Smith-Treadwell AM. Video modeling and children with autism spectrum disorder: a survey of caregiver perspectives. Educ Treat Child. 2015;38.
- Yeganyan MT, Cramer M, Boyd LA, Hayes GR. vSked: An Interactive Visual Schedule System for Use in Classrooms for Children With Autism. In: Proceedings of the 9th International Conference on Interaction Design and Children. Association for Computing Machinery, New York; 2010:319–322.
- Lorimer PA, Simpson RL, Smith Myles B, Ganz JB. The use of social stories as a preventative behavioral intervention in a home setting with a child with Autism. J Posit Behav Interv. 2002;4:53–60.
- Scattone D, Tingstrom DH, Wilczynski SM. Increasing appropriate social interactions of children with autism spectrum disorders using social stories. Focus Autism Other Dev Disabl. 2006;21:211–222.
- Keeling K, Myles BS, Gagnon E, Simpson RL. Using the power card strategy to teach sportsmanship skills to a child with autism. Focus Autism Other Dev Disabl. 2003;18:105–111.
From Decisions in Dentistry. February 2020;6(2):26–28,31.

