
 MARCO HERRNDORFF / ISTOCK / GETTY IMAGES PLUS
MARCO HERRNDORFF / ISTOCK / GETTY IMAGES PLUS
Caries Concerns in Older Adults
Dental professionals play an important role in helping this population maintain their natural dentition and oral health.
PURCHASE COURSE
This course was published in the October 2022 issue and expires October 2025. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the October 2022 issue and expires October 2025. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 250
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Explain population projections for older adults in the United States and the ramifications for oral health professionals when treating this demographic.
- Identify caries risk factors for older adults.
- Describe interventions and other strategies for managing caries risk in this patient population.
- Discuss potential dexterity issues with older adults, as well as devices, modifications and techniques that can be suggested to facilitate effective self-care.
Americans continue to live longer and more active lives. In the future, this improved quality and quantity of life is projected to surpass current statistics. By 2060, the number of Americans age 65 and over will grow to 98 million from 46 million currently.1–3 As such, oral health professionals are in a unique position to empower and motivate patients to remain free from oral disease well into old age. As health status changes over time, patients can work with oral health professionals to prevent caries and periodontal disease, helping them maintain a healthy dentition. Preventive care is critical to this population because of the many complexities that may arise during treatment for a range of health issues, as well as gingival recession that is often associated with advancing years.
While evidence of coronal caries in older adults is minimal, the literature suggests an increased risk for root caries among this patient cohort.4 The Healthy People 2030 initiative, developed by the U.S. Department of Health and Human Services, identifies oral health objectives, and one of these is to reduce the amount of untreated root decay.5 Approximately 29% of older adults have untreated root caries. Overall, more than 90% of American older adults have experienced dental caries.6 The National Institutes of Health reports that 93% of adults age 65 and older have experienced caries and 18% have untreated decay.7
BARRIERS TO CARE
Financial, cultural and structural barriers to care exist for older adults.8 Untreated decay is more prevalent among those experiencing poverty. Approximately one-third of older adults living in poverty have untreated decay, while only 7% of non-poor older adults have untreated decay.9 Older adults may have lost dental insurance coverage upon retirement, and thus go without care.10 This population may have other financial burdens brought on by medical conditions. For example, older adults living with Alzheimer’s disease may need around-the-clock care with little to no resources to support dental care.11 Older adults with financial resources experience better oral health outcomes, including maintaining a natural dentition for a longer period of time.
Cultural barriers to care exist, including those related to language, perception and socioeconomic status. Untreated caries rates are more than double among Mexican-Americans and Black non-Hispanic Americans compared to non-Hispanic white Americans.9 These oral health inequalities continue to grow as the topic of whether oral health is an essential component of Americans’ healthcare benefits is hotly debated.9
Structural barriers also exist for older adults. Those living in rural locations may have difficulty accessing care due to a lack of providers or transportation.12 For older adults living in nursing homes or assisted living communities, this barrier has been amplified during the COVID-19 pandemic.13 Early in the pandemic, these facilities had to isolate their residents to protect their health, and the increased isolation, which may persist today, caused some to postpone dental care.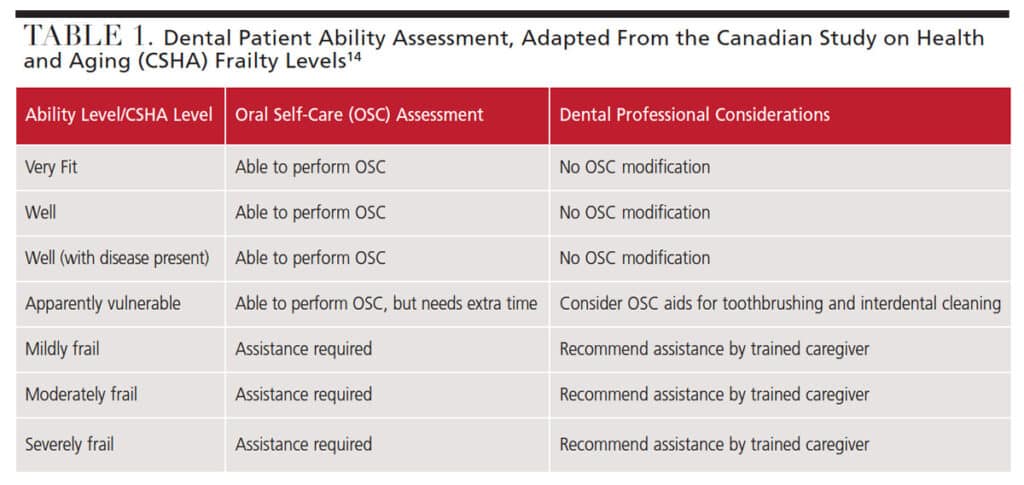
ASSESSING PATIENT SELF-CARE ABILITY AND ORAL HYGIENE
When determining what oral self-care strategies are best suited for older adults, dental professionals should consider the patient’s ability and dependence on others.8 Individuals living in nursing homes or assisted living facilities may be dependent on caregivers for oral self-care.12 Caregivers need to be educated about oral self-care delivery tailored to the individual’s needs. By using a clinical assessment tool, such as the Canadian Study on Health and Aging Clinical Frailty Scale, providers can recommend appropriate oral self-care aids based not only on the clinical examination, but also an evaluation of the patient’s ability to perform the tasks (Table 1).8,14
Dental providers can make informed decisions regarding oral self-care recommendations and treatment after clinical assessment of the patient. In addition to evaluating the patient’s ability to properly clean the teeth and mouth, clinicians should consider other factors, including the use of medications that reduce salivary function.15 Older adults who experience common medical conditions, such as diabetes and hypertension, may experience xerostomia due to the use of prescription medications.15 The decrease of the protective saliva in the oral environment also increases the patient’s risk for caries.
Older adults experiencing xerostomia may benefit from salivary substitutes and the salivary stimulation gained by chewing sugar-free gum containing xylitol.16 Over-the-counter saliva substitutes, lozenges and oral melts are also available that contain xylitol.17 For older adults with xerostomia, a sialogogue may be indicated.16
Conditions such as rheumatoid arthritis, Alzheimer’s disease and Parkinson’s disease may impact joints, therefore limiting mobility and making oral self-care difficult.15 For older adults who are unable to independently use manual oral self-care tools, devices such as electric toothbrushes and power flossers should be considered.
Among this cohort, some patients may also experience depression, which can lead to a lack of motivation or energy to perform oral self-care.15 These patients may also have a poor diet.6,15 Poor oral health may lead to impairment of mastication and thus contribute to poor nutrition.10 Recommendations should be made for foods with cariostatic properties.6 Oral health professionals should incorporate nutrition counseling into oral self-care instruction for this patient group. Beginning with a comprehensive nutritional assessment that includes a thorough review of personal, medical and dental histories, providers can motivate the patient to incorporate behavioral changes that support nutritional health.18,19
For all older adults (especially those presenting with poor oral hygiene), additional appointment time may be needed to review proper brushing, flossing and rinsing techniques. Patients should have a tailored set of recommendations that are based on the assessment of their needs and abilities.

PREVENTION AND MANAGEMENT STRATEGIES
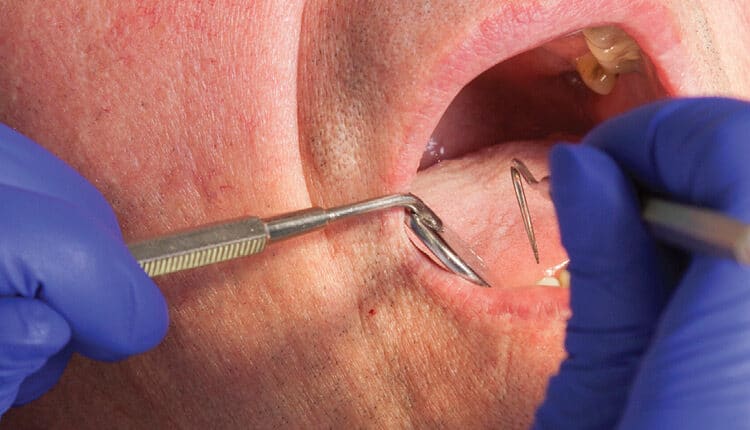
A study by Gao et al11 suggests a tell-show-do approach to teaching oral self-care methods is effective with older adults (Figure 1). Any professional recommendation related to oral self-care should be demonstrated for the patient, who should then perform the technique so the professional can ensure correct technique that can be replicated at home. While many of the oral self-care recommendations made for this group mirror those for the rest of the population, each patient’s individual needs and abilities should be assessed.
As noted, many older adults are at increased risk for caries. Consequently, professional fluoride treatments and at-home fluoride mouthrinses may be recommended for those at increased risk.20 Some mouthrinses are formulated to be gentle on the sensitive mouths of older patients, all of whom should use fluoride toothpaste.
For patients with weakened tooth structure or untreated caries, silver diamine fluoride (SDF) may be an option.15 In 2018, the American Dental Association (ADA) stated that SDF could be used as a nonrestorative treatment. And in 2020, the ADA supported the use of SDF to arrest caries.15 This agent has been found to arrest root caries in older adults when applied at six-month intervals.21
TOOTHBRUSHING TECHNIQUES
Toothbrushing methods should also be selected with the patient’s dexterity in mind, as those with a limited range of movement may require caregiver support and assistance. These individuals may benefit from special toothbrushes with modified handles.22 As adults age, hand-grip strength decreases and dexterity can be affected.23–25 Toothbrushes with a tennis ball or bicycle grip attached to the handle can assist patients facing these issues.
Additionally, brushing techniques can be tailored based on patient ability.26 The Bass and modified Bass methods are popular, but the required angulation of the brush (pointed toward the gingiva at 45° to the tooth) may be difficult for older adults with limited dexterity.19 Stillman and modified Stillman toothbrushing methods allow for massage of the tissue and removal of soft debris along the gingival margin. According to Bowen and Pieran,18 this technique should be considered for patients with recession. For older adults with fixed prosthetics and partial dentures, the Charters toothbrushing technique — which involves placing the brush at a 45° angle to the occlusal plane while making overlapping, vibratory strokes — should be recommended.19
INTERPROXIMAL CLEANING RECOMMENDATIONS
A study that tracked older adults over five years found that those who flossed experienced reduced caries incidence.27 Oral health professionals should consider the following factors when determining interproximal cleaning recommendations: dental anatomy, integrity of the gingiva, and interproximal bone levels.19 Available in different shapes and sizes to accommodate variances in anatomy and embrasure spaces, interdental brushes are exceptionally effective in biofilm removal on concave tooth surfaces.19 In such areas, dental floss or tape may not be able to cleanse properly, as these tools are less likely to adapt to the tooth anatomy.
Clinicians should select an appropriately sized interdental brush by assessing the embrasure space. A slightly larger brush than embrasure space should be chosen to allow for effective interdental cleaning.18 For older adults with bridgework, floss threaders or tufted floss should be used to cleanse under pontics and interproximal areas of abutment teeth. For patients with limited dexterity and those without caregivers to help with oral self-care, power flossers may be recommended. Water flossers may be effective for interdental cleaning in older adults with limited dexterity.19
While the assessment of the oral cavity and consideration of the patient’s ability should inform oral self-care instruction, dental professionals should also consider the patient’s environment. Whether a patient lives alone can be important when making recommendations for vulnerable older adults. Additionally, caregivers should be involved in oral health education.
CONCLUSION
Age impacts oral disease prevalence indirectly through impairment of cognitive and physical capability, and directly on a cellular level.8 Limitations due to ability and barriers to care must be recognized when developing oral self-care recommendations. Dental professionals should advocate for individualized oral self-care plans, including recommendations for brushing and interdental cleaning.8 As the older adult population continues to grow, so does the need for dental teams to deliver tailored oral self-care recommendations to their patients.
REFERENCES
- American Psychological Association. Older Adults: Health and Age-Related Changes. Available at: https://www.apa.org/pi/aging/resources/guides/older. Accessed August 31, 2022.
- U.S. Centers for Disease Control and Prevention. Older Persons’ Health. Available at: https://www.cdc.gov/nchs/fastats/older-american-health.htm. Accessed August 31, 2022.
- World Health Organization. Ageing. Available at: https://www.who.int/health-topics/ageing#tab=tab_䁯. Accessed August 31, 2022.
- Hendre AD, Taylor GW, Chavez EM, Hyde S. A systematic review of silver diamine fluoride: effectiveness and application in older adults. Gerontology. 2017;34:411–419.
- U.S. Department of Health and Human Services. Healthy People 2030. Available at: https://health.gov/healthypeople/objectives-and-data/browse-objectives/oral-conditions/reduce-proportion-older-adults-untreated-root-surface-decay-oh-04. Accessed August 31, 2022.
- Blostein FA, Jansen EC, Jones AD, Marshall TA, Foxman B. Dietary patterns associated with dental caries in adults in the United States. Community Dent Oral Epidemiol. 2020;48:119–129.
- National Institute of Dental and Craniofacial Research. Dental Caries (Tooth Decay) in Seniors (Age 65 and Older). Available at: https://www.nidcr.nih.gov/research/data-statistics/dental-caries/seniors. Accessed August 31, 2022.
- Tonetti MS, Bottenberg P, Conrads G, et al. Dental caries and periodontal diseases in the ageing population: call to action to protect and enhance oral health and well‐being as an essential component of healthy ageing — Consensus report of Group 4 of the joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J Clin Periodontol. 2017;44:S135–S144.
- Yarbrough C, Vujicic, M. Oral health trends for older Americans. J Am Dent Assoc. 2019;150:714–716.
- Allin S, Farmer J, Quinonez, C, et al. Do health systems cover the mouth? Comparing dental coverage for older adults in eight jurisdictions. Health Policy. 2020;124:998–1007.
- Gao S, Chu C, Young F. Oral health and care for elderly people with Alzheimer’s disease. Int J Environ Res Public Health. 2020;17:5713.
- Madunic D, Gavic L, Kovacic I, Vidovic N, Vladislavic J, Tadin A. Dentists’ opinions in providing oral healthcare to elderly people: a questionnaire-based online cross-sectional survey. Int J Environ Res Public Health. 2021;18:3257.
- Aquilanti L, Santarelli A, Mascitti M, Procaccini M, Rappelli G. Dental care access and the elderly: what is the role of teledentistry? A systematic review. Int J Environ Res Public Health. 2020;17:9053.
- Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173:489–495.
- Chan AKY, Tamrakar M, Jiang CM, Lo ECM, Leung KCM, Chu CH. Common medical and dental problems of older adults: a narrative review. Geriatrics. 2021;6:76.
- Taverna M. Xerostomia diagnosis and management. Dimensions of Dental Hygiene. 2020:18(4):22–26.
- Salinas T. Dry mouth treatment: Tips for controlling dry mouth. Available at: https://www.mayoclinic.org/diseases-conditions/dry-mouth/expert-answers/dry-mouth/faq-20058424. Accessed August 31, 2022.
- Bowen DM, Pieran JA. In: Darby and Walsh Dental Hygiene Theory and Practice. 5th ed. St. Louis: Elsevier; 2020.
- Boyd LD, Mallonee LF, Wyche CJ, Halaris, JF. Wilkins’ Clinical Practice of the Dental Hygienist. 13th ed. Burlington, Mass: Jones & Bartlett; 2021.
- American Dental Association. Clinical Recommendations for Use of Professionally Applied or Prescription Strength, Home-Use Topical Fluoride Agents for Caries Prevention in Patients at Elevated Risk of Developing Caries. Available at: https://www.ada.org/-/media/project/ada-organization/ada/ada-org/files/resources/research/ada_evidence-based_topical_fluoride_chairside_guide.pdf?rev=28cbb81b6c994cc79e⭷b62e606d0e9&hash=13BA63A12312AE4E6B0754330FF8CF9B. Accessed August 31, 2022.
- Mitchell C, Gross A, Milgrom P, Mancl L, Prince D. Silver diamine fluoride treatment of active root caries lesions in older adults: a case series. J Dent. 2021;105:103561.
- Phadraig CMG, Farag M, McCallion P, Waldron C, McCarron M. The complexity of tooth brushing among older adults with intellectual disabilities: Findings from a nationally representative survey. Disabil Health J. 2020;13:100935.
- Shin NR, Yi YJ, Choi JS. Hand motor functions on the presence of red fluorescent dental biofilm in older community-dwelling Koreans. Photodiagnosis Photodyn Ther. 2019;28:120–124.
- Saintrain MVL, Saintrain SV, Sampaio EGM, et al. Older adults’ dependence in activities of daily living: Implications for oral health. Public Health Nurs. 2018;35:473–481.
- Dayanidhi S, Valero-Cuevas FJ. Dexterous manipulation is poorer at older ages and is dissociated from decline of hand strength. J Gerontol. 2014;69:1139–1145.
- Rajwani AR, Quaraophia S, Hawes ND, et al. Effectiveness of manual toothbrushing techniques on plaque and gingivitis: A systematic review. Oral Health Prev Dent. 2020;20:843–854.
- Marchesan JT, Bryd KM, Moss K, et al. Flossing is associated with improved oral health in older adults. J Dent Res. 2020;99:1047–1053.
From Decisions in Dentistry. October 2022;8(10):32-35.

