

Beyond Survival Rates to True Success With All-on-4 Implants
As demand for full-arch rehabilitation grows, clinicians must evaluate All-on-4 outcomes for tissue health, prosthetic integrity, and patient satisfaction.
The global population affected by severe periodontitis and edentulism will significantly grow in the coming decades.1 Thus, treatment for edentulism or terminal dentition will continue to remain in high demand. Gaining popularity since 2000, the All-on-4 concept advocates placing four implants in ideal loading distribution to support the fixed full-arch prosthesis. The technique effectively overcomes the drawbacks of complete dentures (CD) and is at a reasonable price point for patients.
In the literature, the long-term implant success rate and prosthetic success rate of All-on-4 ranges from 91.9% to 99.6%.3 However, a biologic complication rate of 18.9% to 25.5% in addition to a mechanical complication rate of 7.3% to 36.7 % should not be overlooked.3 Success of All-on-4 treatment should not be based solely on implant survival rate but also on the absence of prosthetic complications, stable peri-implant tissue, esthetic results, and patient-reported outcomes.
Success of Osseointegration With Healthy Peri-Implant Tissue
Evaluating the outcomes of All-on-4 treatment is essential. Although implant- and prosthesis-related parameters are extensively used in research for evaluation, the applicable translation into clinical settings is lacking.
When beginning the comprehensive evaluation for All-on-4 treatment, the success of osseointegration and the health of peri-implant tissue should be assessed. Removal of the prosthesis is recommended to provide better access and visibility. Successful osseointegration could be readily determined with the absence of clinical mobility. An implant stability quotient test and radiographic evaluation are effective auxiliary diagnostic tools. Peri-implant tissue should be evaluated with the following parameters: probing depth; signs of inflammation (bleeding, suppuration, abscess/sinus tract); peri-implant tissue appearance (color, texture, consistency); peri-implant soft-tissue quality; and any patient-reported symptoms such as pain or swelling (Table 1).
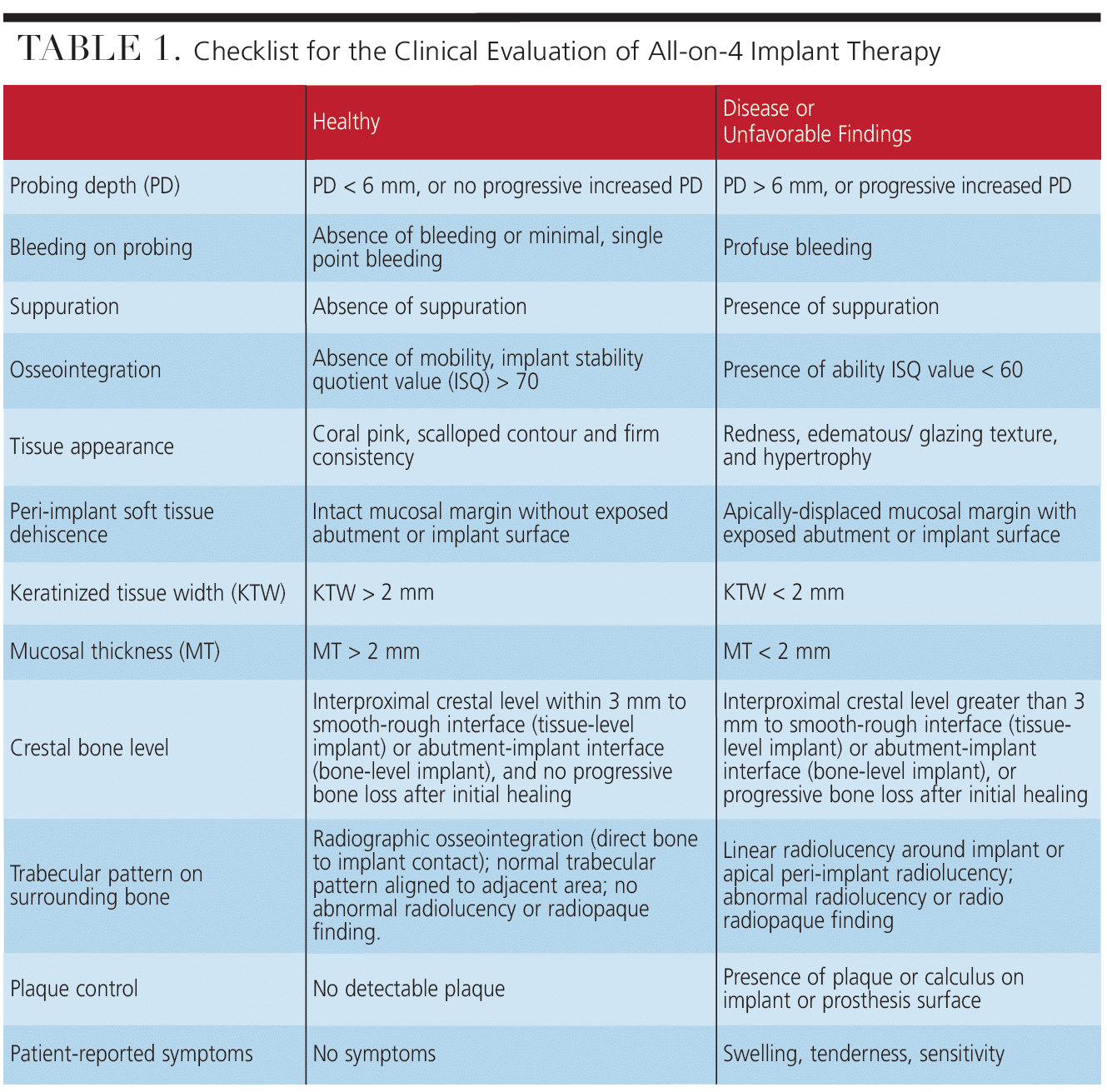
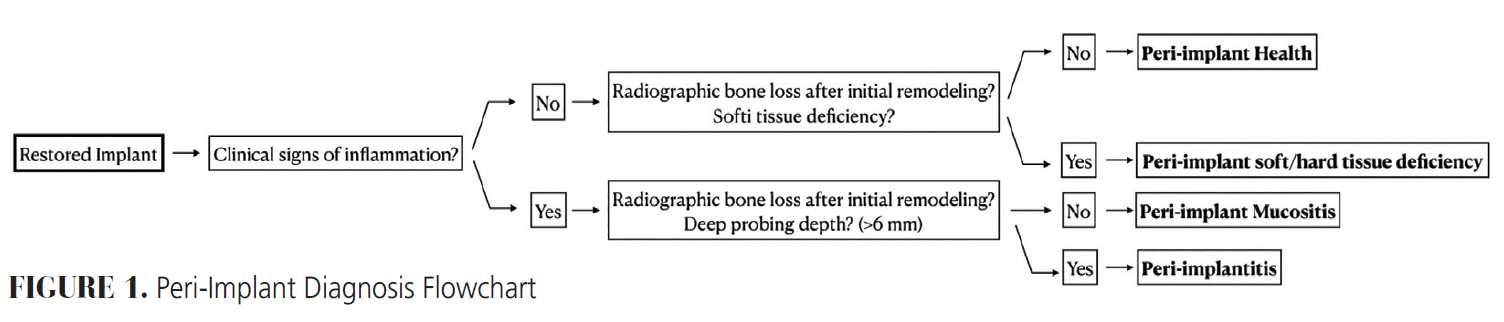
Periapical radiographs should be updated for monitoring crestal bone level and trabecular bone pattern of surrounding bone. Cone-beam computed tomography (CBCT) should be considered when the morphology of bony defects needs further investigation or when the two-dimensional image fails to provide sufficient information. After thorough data collection, diagnosis for implants should be assigned according to American Academy of Periodontology/European Federation of Periodontology 2018 classification (Figure 1).4
Marginal Bone Loss
Marginal bone loss has been considered physiologic bony remodeling during the first year after implant placement. Historically, 1.5 mm marginal bone loss was considered normal when most implants used an external connection design. The evolution of implant design (surface treatment, nontitanium abutment material, internal connection, and platform switching) and subcrestal implant placement minimize physiologic bone remodeling.
A periapical radiograph taken at 1-year follow-up can serve as a good reference to determine whether progressive bone loss occurs after the initial bone remodeling. In addition, tilted implants are not a risk factor for marginal bone loss, so bone loss around tilted implants should be within the same limit as axially placed implants.5
Soft Tissue Condition
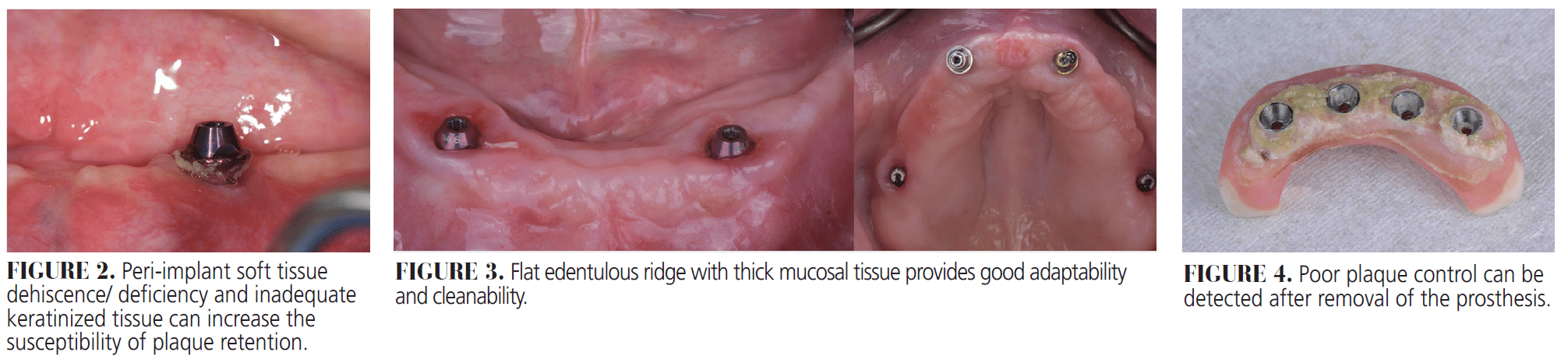
According to the consensus report of the Cairo conference, soft tissue conditions of implants should always be evaluated.6 Adequate (more than 2 mm) keratinized tissue width/attached tissue width and thick peri-implant mucosal thickness not only provide stability of the crestal bone level but also can reduce the susceptibility to peri-implant disease. Various methods can be applied to measure mucosal thickness, such as bone sounding, ultrasonic image, surface scan, CBCT, or superimposition of surface scan and CBCT.7 Peri-implant soft tissue dehiscence/deficiency (PSTD) is the apical displacement of the peri-implant soft tissue margin (Figure 2). Early management of PSTD could prevent adverse consequences, such as compromised esthetics, impaired plaque control, and peri-implant disease.8
When soft tissue condition is unfavorable or when PSTD presents, soft tissue grafting should be considered for phenotype modification or keratinized tissue augmentation. Lastly, contour and tissue quality at the edentulous ridge should also be evaluated. An ideal tissue platform for the base of the hybrid prosthesis should be a flat ridge covered with thick keratinized mucosa to provide better adaptation and cleanability (Figure 3).
Oral Hygiene and Maintenance
According to recommendations from the American College of Prosthodontists, maintenance for fixed full-arch prosthesis should be rendered every 2 to 6 months based on the patient’s risk profile.9 Patients’ self-care protocol should be reviewed at each maintenance appointment. In addition, predisposing factors for poor plaque control, such as enlarged prosthesis-tissue gap, calculus, and exposed threads should be properly identified (Figure 4). Furthermore, changes in the patient’s medical history that may impact his or her oral care, including hyposalivation, parafunctional habits, mucositis, decreased dexterity, or lack of motivation, should also be carefully noted. Lastly, oral hygiene instruction should be modified accordingly.
Esthetics
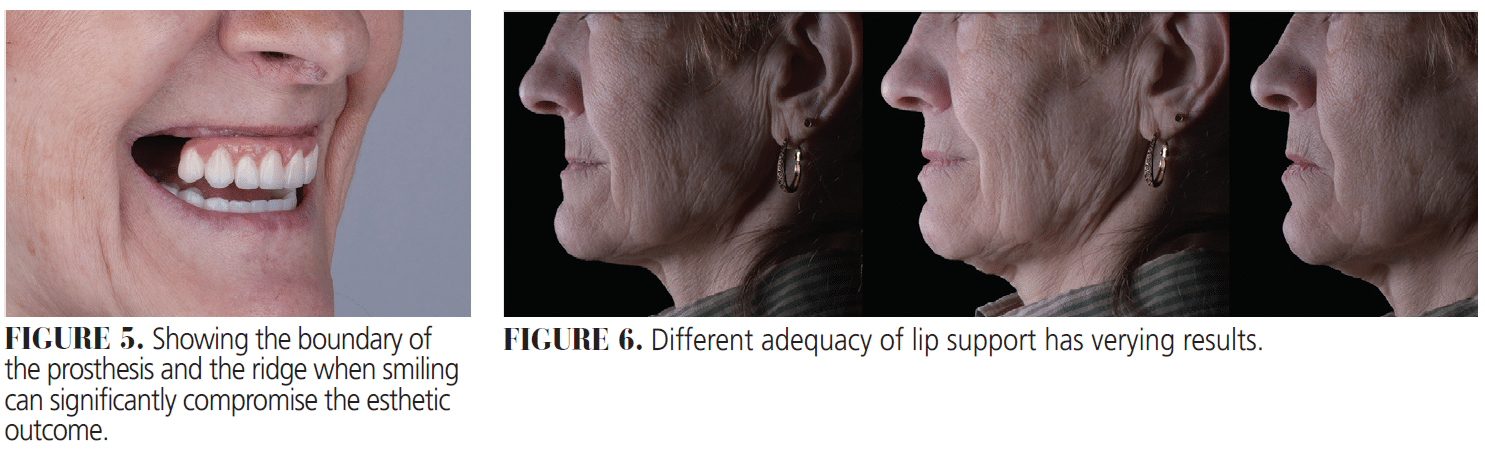
Esthetic evaluation should be performed to exclude the following three major complications to ensure a successful esthetic outcome. First, the boundary between the prosthesis and the mucosa should not be visible during full animation (Figure 5). Additional caution must be taken if the patient has lip hypermobility, vertical maxillary excess, or short upper lip.
Second, the adequacy of lip support provided by the prosthesis should be evaluated. Ideal lip contour can be evaluated with nasolabial angle and the display of teeth, however, the patient’s preference should also be considered (Figure 6).
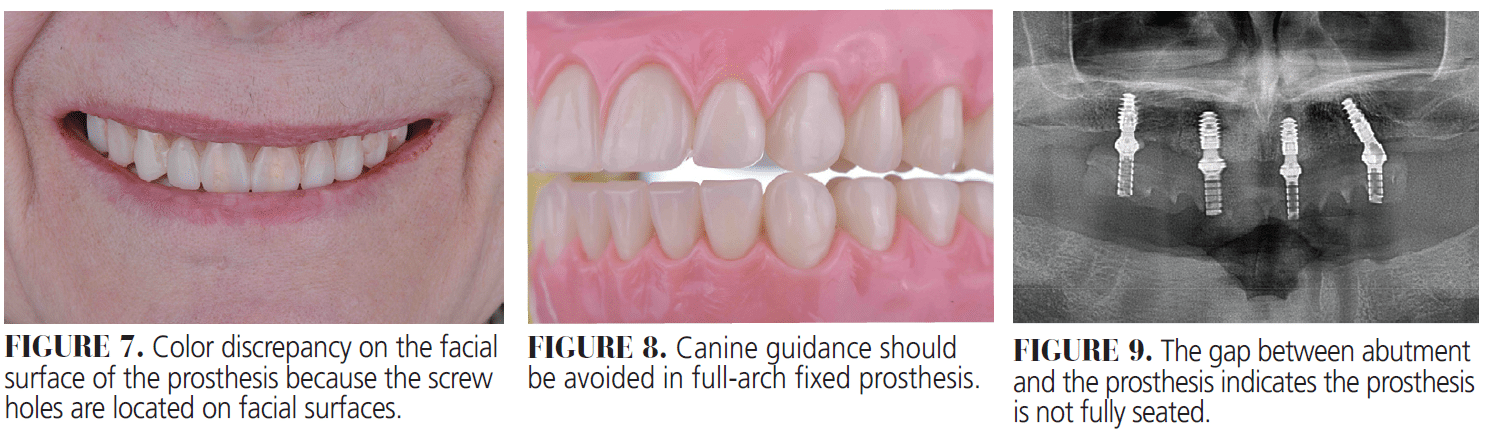
The third complication is the visibility of screw access channels on the facial surface of the prosthesis. Angled multiunit abutments can be used to correct the opening of screw holes of malpositioned implants (Figure 7). Refabrication of the prosthesis should be considered when the esthetic outcome cannot meet the patient’s expectations.
Patient Satisfaction
Generally speaking, edentulous patients’ satisfaction and quality of life improve after receiving fixed full-arch prostheses.10 Replacing the implant-retained removable overdenture with fixed full-arch prosthesis can significantly increase patient satisfaction.11 However, treatment planning should also account for differences in the ease of cleaning between these two options. Due to mobility of the lower jaw during articulation, tongue motion, limited keratinized gingival tissue, and decreased contact surface area with the prosthesis, lower satisfaction is usually reported in mandibular treatment.12
Phonetics
Speech performance can be significantly altered after a fixed full-arch prosthesis is placed.13 The first evaluation of phonetics should be conducted at the provisional stage. Wearers of fixed full-arch prostheses exhibit articulation disorders involving /s/, followed by /z/, /t/, and /d/.14 Significant speech distortions were observed, especially for /s/, at 1, 3, and 6 months after the delivery of the fixed full-arch prosthesis. However, speech articulation returned to the normal range spontaneously after 1 to 3 years.14 Waiting at least 1 year before refabricating the prosthesis is recommended because muscles can adapt to the new prosthesis.
Occlusion
What type of occlusion should be used in fixed full-arch prosthesis is still controversial. Balanced occlusion without interferences is required for immediate loading, ensuring excursive movements do not overload the provisional restorations or disrupt early osseointegration.15 Occlusal scheme after osseointegration should be determined based on the dentition of the opposing arch. When the opposing prosthesis is a CD, bilateral balanced occlusion is recommended. Conversely, when the opposing arch is not a CD, group function occlusion should be used.15 One in vitro study showed canine guidance was significantly correlated with higher complication rates, such as major chipping compared to group function occlusion (Figure 8).16,17 When metal-acrylic is used for the All-on-4 prostheses, the prosthesis should be checked to ensure it maintains group function during every recare appointment because the material tends to wear over time.
Connection of the Prosthesis
Panoramic or periapical radiographs should be updated to assess the fit of connection between the prostheses and abutments during maintenance recare to avoid potential mechanical complications (Figure 9).15
Common Complications
As mentioned above, complications in All-on-4 treatment are not rare. Not only should these complications be checked at every recare appointment, the identified risk factors should also be properly managed. The most evidence-supported risk indicator for mechanical complications is bruxism.
Bruxism patients are 15 times more likely to experience mechanical complications for All-on-4 treatments.18 Other risk indicators for mechanical complications include gender, canine guidance, length of time the prosthesis is in place, and the type of opposing dentition. The most frequent major complications were wear of prosthetic material (5.85%/year) and framework fracture (1.69%/year). The most common minor complications were loss of screw access hole material (5.18%/year) and minor wear of prosthetic material (3.57%/year).19
Conclusion
All-on-4 is a predictable treatment modality for patients experiencing edentulism or terminal dentition. Biological and prosthetic comprehensive outcome evaluation should be performed properly and regularly to ensure the patient’s satisfaction with the treatment. Early detection and management of risk factors are essential to provide the long-term stability of a successful outcome.
References
- Nascimento GG, Alves-Costa S, Romandini M. Burden of severe periodontitis and edentulism in 2021, with projections up to 2050: The Global Burden of Disease 2021 study. J Periodontal Res. 2024;59:823-867.
- Emami E, Michaud PL, Sallaleh I, Feine JS. Implant-assisted complete prostheses. Periodontol 2000. 2014;66:119-131.
- Maló P, de Araújo Nobre M, Lopes A, Ferro A, Botto J. The All-on-4 treatment concept for the rehabilitation of the completely edentulous mandible: A longitudinal study with 10 to 18 years of follow-up. Clin Implant Dent Relat Res. 2019;21:565-577.
- Hopp M, de Araújo Nobre M, Maló P. Comparison of marginal bone loss and implant success between axial and tilted implants in maxillary All-on-4 treatment concept rehabilitations after 5 years of follow-up. Clin Implant Dent Relat Res. 2017;19:849-859.
- Caton J, Armitage G, Berglundh T, et al. A new classification scheme for periodontal and peri-implant diseases and conditions – Introduction and key changes from the 1999 classification. J Periodontol. 2018;89(Suppl 1):S1–S8.
- Del Amo FSL, Yu SH, Sammartino G, et al. Peri-implant Soft Tissue Management: Cairo Opinion Consensus Conference. Int J Environ Res Public Health. 2020;17:2281.
- Ferry K, AlQallaf H, Blanchard S, Dutra V, Lin WS, Hamada Y. Evaluation of the accuracy of soft tissue thickness measurements with three different methodologies: An in vitro study. J Periodontol. 2022;93:1468-1475.
- Zucchelli G, Tavelli L, Stefanini M, et al. Classification of facial peri-implant soft tissue dehiscence/deficiencies at single implant sites in the esthetic zone. J Periodontol. 2019;90:1116-1124.
- Kumar S, Kar K, Jivraj S. Maintenance of full-arch implant-supported restorations: peri-implant and prosthetic considerations. In: Graftless Solutions for the Edentulous Patient. Princeton, New Jersey: Springer Nature; 2023:495-515.
- Martín-Ares M, Barona-Dorado C, Guisado-Moya B, Martínez-Rodríguez N, Cortés-Bretón-Brinkmann J, Martínez-González JM. Prosthetic hygiene and functional efficacy in completely edentulous patients: satisfaction and quality of life during a 5-year follow-up. Clin Oral Implants Res. 2016;27:1500-1505.
- Yao CJ, Cao C, Bornstein MM, Mattheos N. Patient-reported outcome measures of edentulous patients restored with implant- supported removable and fixed prostheses: a systematic review. Clin Oral Implants Res. 2018;29(Suppl 16):241-254.
- Fontijn-Tekamp FA, Slagter AP, Van Der Bilt A, et al. Biting and chewing in overdentures, full dentures, and natural dentitions. J Dent Res. 2000;79:1519-1524.
- Meira IA, Gama LT, Prado-Tozzi DA, Pinheiro MA, Rodrigues Garcia RCM. Speech in implant-supported and removable complete denture wearers: A systematic review. J Prosthet Dent. 2022;128:1230-1238.
- Fonteyne E, Van Doorne L, Becue L, Matthys C, Bronckhorst E, De Bruyn H. Speech evaluation during maxillary mini-dental implant overdenture treat- ment: A prospective study. J Oral Rehabil. 2019;46:1151-1160.
- Penarrocha-Diago M, Penarrocha-Diago M, Zaragozí-Alonso R, Soto-Penaloza D. Consensus statements and clinical recommendations on treatment indications, surgical procedures, prosthetic protocols and complications following All-On-4 standard treatment. 9th Mozo-Grau Ticare Conference in Quintanilla, Spain. J Clin Exp Dent. 2017;9:e712-e715.
- Türker N, Alkiş HT, Sadowsky SJ, Şebnem Büyükkaplan U. Effects of occlusal scheme on all-on-four abutments, screws, and prostheses: a three-dimensional finite element study. J Oral Implantol. 2021;47:18-24.
- Nikellis T, Lampraki E, Romeo D, et al. Survival rates, patient satisfaction, and prosthetic complications of implant fixed complete dental prostheses: a 12-month prospective study. J Prosthodont. 2023;32:214-220.
- Chochlidakis K, Ercoli C, Einarsdottir E, et al. Implant survival and biologic complications of implant fixed complete dental prostheses: An up to 5-year retrospective study. J Prosthet Dent. 2022;128:375-381.
- Chochlidakis K, Einarsdottir E, Tsigarida A, et al. Survival rates and prosthetic complications of implant fixed complete dental prostheses: An up to 5-year retrospective study. J Prosthet Dent. 2020;124:539-546.
From Decisions in Dentistry. October/November 2025;11(5):16-19.
