
 IBNJAAFAR/ISTOCK/GETTY IMAGES PLUS
IBNJAAFAR/ISTOCK/GETTY IMAGES PLUS
Application of Cvek Pulpotomy in Treating Head and Neck Radiation Cases
This case report describes the use of a Cvek pulpotomy in a patient with a history of head and neck radiation to help mitigate the risk of osteoradionecrosis of the jaw.
PURCHASE COURSE
This course was published in the March 2021 issue and expires March 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the March 2021 issue and expires March 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Explain the risks and incidence of osteoradionecrosis of the jaw (ONJ) in dental patients.
- Describe a Cvek pulpotomy, and, when indicated, its clinical application, especially in the conservative treatment of patients at risk of ONJ.
- Discuss the presentation of ONJ, as well as clinical parameters that support successful outcomes in a Cvek pulpotomy.
Had and neck cancer has been trending down in the United States since 2002.1 However, it is the ninth most common malignant neoplasm in the world, with high incidence, prevalence and mortality.2 When these patients are treated with radiotherapy, there is a possibility of osteoradionecrosis of the jaw (ONJ), especially postoperatively from surgical dental treatment that traumatizes the bone and challenges its healing capacity. Other risk factors include peri-resective surgery of the jaw, continued alcohol and tobacco use after radiotherapy, poor oral hygiene, diabetes mellitus type 2, and total radiation dose more than 50 gray (Gy).3,4
A diagnosis of ONJ is based on clinical presentation and observation: irradiated bone becomes devitalized and exposed through the overlying skin or mucosa without healing for three months, and without recurrence of the tumor.5 The clinical presentations of ONJ are pain, drainage, and fistulation of the mucosa or skin.5 Other bone diseases of the jaw can be similarly diagnosed in this fashion — for example, osteomyelitis of the jaw and medication-related ONJ.6,7 Additionally, ONJ warrants lifelong attention for head and neck cancer survivors because post-radiotherapy extraction is associated with gradually increased risk of ONJ over time (peaking at four to five years).8 Although ONJ occurs typically in the first years after radiotherapy, patients remain at indefinite risk.3
This paper describes the application of Cvek pulpotomy to provide noninvasive care to a patient with a history of head and neck radiation. The goal was to mitigate the risk of ONJ. The patient had a vital tooth with rampant caries and complex root morphology. Rather than perform an invasive extraction or challenging endodontic therapy with poor prognosis, a Cvek pulpotomy on a mesiobuccal and mesiolingual canal was rendered as the treatment of choice. Traditionally, Cvek pulpotomy is indicated for injured permanent incisor teeth in young patients with exposed vital pulp tissue and immature apices.9 The procedure involves the removal of a small portion of the vital coronal pulp as a means of preserving the remaining coronal and radicular pulp tissues, thus eliminating bacteria from the dentin-pulp complex.10 This treatment preserves pulpal function, while allowing continued root development.11 The innate capacity of pulp tissue to be repaired in the absence of microbial contamination did not indicate this treatment could not be performed successfully in older patients.12 Evidence suggests the patient’s age and status of the root apex did not affect the reported successful outcome.12 The critical determinant of success is the complete removal of the inflamed pulp, rather than the status of the root apex.12

CASE REPORT
A 73-year-old male presented for emergency care with a chief concern of sharp pain from a lower left tooth. Clinical examination revealed tooth #18 had mesiobuccal cusp fracturing, with extensive decay. Pulp testing of #18 showed no abnormalities and the pulpal tissues were diagnosed as vital. A periapical radiograph showed no signs for apical periodontitis, but the tiny projection lines of the periodontal ligament indicated a strong curvature of mesial root(s), as shown in Figure 1.13 A comprehensive medical and dental examination was administered. The medical history included well-controlled hypertension, type 2 diabetes, osteoarthritis and sleep apnea. A prior history of tobacco use before quitting 12 years ago was noted. The patient was diagnosed in 2010 with acoustic neuroma in his left ear when a magnetic resonance imaging scan revealed a 2.5-cm mass at the internal auditory canal consistent with acoustic neuroma. The patient was treated with stereotactic radiosurgery of 12.5 Gy in a single fracture/dose. Six doses were administered, for a total dose of 75 Gy. Primary complaints of tinnitus and significant hearing loss out of the left ear were major side effects of radiosurgery. No fascial numbness or weakness, significant balance loss or vertigo were reported.
Awareness of the potential complication of ONJ was taken into consideration. The patient’s total radiotherapy dose had exceeded 50 Gy. Root canal therapy was recommended. An alternative treatment plan for hyperbaric oxygen with extraction was discussed. The patient elected to save his tooth and declined the more invasive treatment. Prior to endodontic therapy, cone beam computed tomography (CBCT) volumetric imaging was performed. The

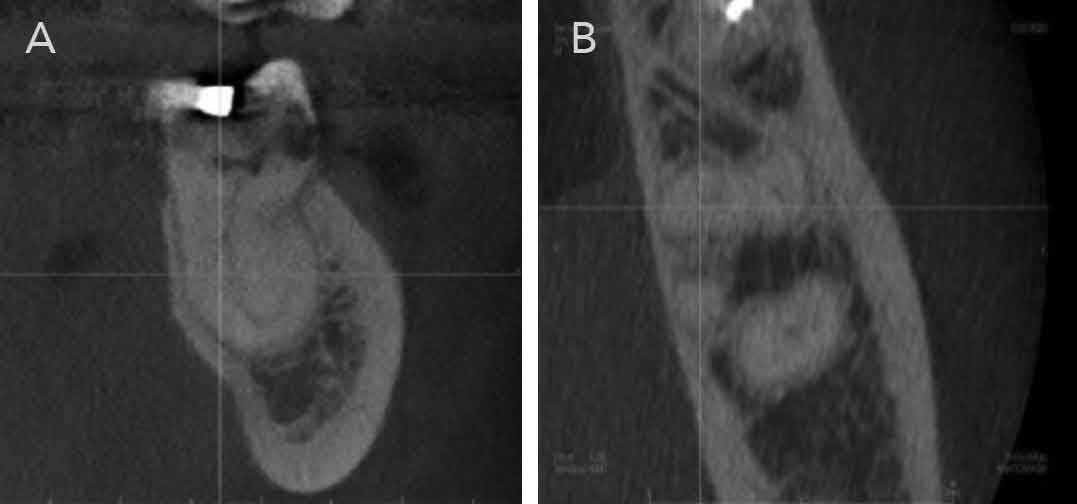
CBCT scan was accompanied by a formal radiology interpretation from a board certified oral and maxillofacial radiologist. The radiographic finding for tooth #18 included mesiobuccal coronal caries to the pulp, an intact periodontal ligament space, and mesial and distal roots with no evidence of apical inflammation. The mesial root bifurcated in its lingual/apical half, as shown in Figure 2 and Figure 3A. The anatomic variation of the root anatomy of tooth #18 is called radix entomolaris (RE), as shown in Figure 3B.
During the initial visit, all buccal and occlusal caries were excavated. The tooth was deemed restorable and temporized. The patient was referred for endodontic treatment on tooth #18. In conjunction with a dental microscope, the procedure was completed under dental dam isolation. Tooth #18 had three identifiable canals. A Cvek pulpotomy on a mesiobuccal and mesiolingual canal was performed. Bioceramic root repair was placed over the canal, and the opening cavity was sealed. The distal canal was accessed, shaped, disinfected and obturated. A postoperative radiograph confirmed the obturation of the distal canal, as shown in Figure 4. The patient was referred back to his dentist for the permanent restoration of the crown. A follow-up image of tooth #18 was taken (Figure 5) during the core and crown restorative procedure two months after the initial Cvek procedure. The patient reported no postoperative symptoms.
DISCUSSION
Background: The management of irradiated patients with cancer in the head and neck region represents a challenge for multidisciplinary teams. Radiotherapy promotes cellular and vascular decreases that compromise the healing response rate, and ONJ is the most severe sequelae caused by radiotherapy.14 It is associated with previous extractions, especially those carried out post-irradiation.15 Research suggests the incidence of ONJ cases in the mandible ranges between 2% and 22%.16 It affects the mandible more often than the maxilla or any other bones of the head and neck.16 A systemic review by Nabil and Samman15 demonstrated the total incidence of ONJ after tooth extraction in irradiated patients was 7%. The patient’s total radiotherapy dose, in addition to the presence of unusual root canal morphology, was taken into consideration when determining treatment.
Like the number of root canals, the number of roots may also vary.13 Mandibular first molars can have an additional root located lingually (RE) or buccally (radix paramolaris [RP]), as mentioned in the literature by Carabelli.17 The separate RE is mostly situated in the same buccolingual plane. A superimposition of both roots can appear on the preoperative radiograph, resulting in an inaccurate diagnosis.13 In most cases, the use of CBCT or a second radiograph taken from a more mesial or distal angle (30 degrees) can be used to achieve an accurate diagnosis. An accurate diagnosis of these supernumerary roots can avoid complications or a missed canal during root canal treatment.13
The presence of an RE or RP has clinical implications for endodontic treatment.13 Cvek pulpotomy is the preferred option in treating teeth diagnosed with anatomic anomalies, such as RE and den invaginatus, as traditional root canal therapy would be difficult or impossible.10 The prevention or healing of endodontic pathology depends on a thorough chemo-mechanical cleansing and shaping of the root canals before a dense root canal filling with a hermetic seal.13
Apart from a radiographic diagnosis, clinical inspection of the tooth crown and analysis of the cervical morphology of the roots by means of periodontal probing can facilitate identification of an additional root.13 An extra cusp (tuberculum paramolare) or more prominent occlusal distal or distolingual lobe, in combination with a cervical prominence or convexity, can indicate the presence of an additional root.13 If an RE or RP is diagnosed before endodontic treatment, the operator knows what to expect or where to look once the pulp chamber has been opened.13
Management: The vitality of dental pulp is essential for long-term tooth survival.12 As noted, a Cvek pulpotomy involves the removal of a small portion of the vital coronal pulp as a means of preserving the remaining coronal and radicular pulp tissues by eliminating bacteria from the dentin-pulp complex.10 The aim is to remove inflamed or necrotic tissue to uncover deeper, healthy pulp tissue in the pulp chamber.10 This includes removal of 1 to 3 mm of the exposed pulp; that is, the inflamed superficial pulp tissue is amputated up to the level of a healthy pulp.11

The control of hemorrhage using hemostatic agents is important to enhance the success rate of Cvek pulpotomies.12 Hemorrhage of exposed dental pulp tissue is, in part, due to the inflammatory response of the pulp to bacteria and their by-products from carious dentin.12 Halting bleeding allows capping materials to be placed in a relatively dry environment.12 Sodium hypochlorite has been suggested to remove the coagulum, control hemorrhage, remove dentin chips, and aid formation of a dentin bridge.12 Appropriate capping material, such as a bioceramic root repair agent, mineral trioxide aggregate, or calcium-enriched mixture, should be placed gently and directly in contact with noninflamed pulp tissue, with only passive contact with the pulp.11 A good restoration that prevents bacterial penetration into the tooth is essential to the success of a Cvek pulpotomy.11 Additionally, the presence of a healthy periodontium is necessary for success.12 Teeth with moderate to severe periodontal disease are not suitable candidates for this treatment.12 These factors contribute to the reported success rate of 93% to 96% for a partial pulpotomy.12 While the literature indicates pulp exposures of 4 mm or less may have a good prognosis after a Cvek pulpotomy, the prognosis in teeth with pulp exposures of more than 4 mm has not yet been clarified.11

In cases in which the teeth are severely structurally compromised in patients who have undergone radiation therapy or who are taking bisphosphonates, the Cvek technique can be used as an intermediate step in managing pain for individuals at risk of ONJ who are undergoing hyperbaric oxygen treatment in preparation for an extraction. The use of hyperbaric oxygen with extraction as a treatment alternative is recommended per the Marx protocol. Marx theorized the formation of hypoxic-hypocellular hypovascular tissue and breakdown of collagen driven by persistent hypoxia as the cause of chronic nonhealing wounds.16 These explanations formed the cornerstone for the use of hyperbaric oxygen in the treatment of ONJ.16
CONCLUSION
Head and neck cancer patients who are diagnosed and treated early with effective therapy have a good long-term prognosis, yet they will all be affected by the radiotherapy.18 Patients treated with head and neck radiation have diminished healing capacity in the irradiated region and therefore require conservative treatment to avoid ONJ.8 In this case report, in addition to presenting with a rare tooth morphology, the patient was considered at high risk for ONJ. The patient had a vital tooth with rampant caries, so rather than perform an invasive extraction or challenging endodontic therapy with poor prognosis, a conservative treatment was selected.
Based on the premise of the innate capacity of pulp tissue to repair itself in the absence of microbial contamination,12 Cvek pulpotomy is a technique that is worth considering when providing conservative endodontic treatment to a population at risk for ONJ secondary to head and neck radiotherapy. With proper case selection, Cvek pulpotomy remains a prudent treatment choice in an adult patient whose treatment tooth has completed its root development.
REFERENCES
- Mourad M, Jetmore T, Jategaonkar AA, Moubayed S, Moshier E, Urken ML. Epidemiological trends of head and neck cancer in the United States: A SEER population study. J Oral Maxillofac Surg. 2017;75:2562–2572.
- Gomes EP, Aranha AM, Borges AH, Volpato LE. Head and neck cancer patients’ quality of life: analysis of three instruments. J Dent (Shiraz). 2020;21:31–41.
- Jereczek-Fossa BA, Orecchia R. Radiotherapy-induced mandibular bone complications. Cancer Treat Rev. 2002;28:65–74.
- Sathasivam HP, Davies GR, Boyd NM. Predictive factors for osteoradionecrosis of the jaws: A retrospective study. Head Neck. 2018;40:46–54.
- Harris M. The conservative management of osteoradionecrosis of the mandible with ultrasound therapy. Br J Oral Maxillofac Surg. 1992;30:313–318.
- De Antoni CC, Matsumoto MA, Silva AA, et al. Medication-related osteonecrosis of the jaw, osteoradionecrosis, and osteomyelitis: A comparative histopathological study. Braz Oral Res. 2018;32:e23.
- Chronopoulos A, Zarra T, Ehrenfeld M, Otto S. Osteoradionecrosis of the jaws: definition, epidemiology, staging and clinical and radiological findings. A concise review. Int Dent J. 2018;68:22–30.
- Wang TH, Liu CJ, Chao TF, Chen TJ, Hu YW. Risk factors for and the role of dental extractions in osteoradionecrosis of the jaws: A national-based cohort study. Head Neck. 2017;39:1313–1321.
- Sari S. Cvek pulpotomy: report of a case with five-year follow-up. ASDC J Dent Child. 2002;69:27–30,11.
- Hargreaves KM, Berman LH, Rotstein I. Cohen’s Pathways of the Pulp. 11th ed. St Louis, Mo: Mosby; 2016.
- Bimstein E, Rotstein I. Cvek pulpotomy — revisited. Dent Traumatol. 2016;32:438–442.
- Ghoddusi J, Forghani M, Parisay I. New approaches in vital pulp therapy in permanent teeth. Iran Endod J. 2014;9:15–22.
- Calberson FL, De Moor RJ, Deroose CA. The radix entomolaris and paramolaris: clinical approach in endodontics. J Endod. 2007;33:58–63.
- Koga DH, Salvajoli JV, Alves FA. Dental extractions and radiotherapy in head and neck oncology: review of the literature. Oral Dis. 2008;14:40–44.
- Nabil S, Samman N. Incidence and prevention of osteoradionecrosis after dental extraction in irradiated patients: a systematic review. Int J Oral Maxillofac Surg. 2011;40:229–243.
- Tsai CJ, Hofstede TM, Sturgis EM, et al. Osteoradionecrosis and radiation dose to the mandible in patients with oropharyngeal cancer. Int J Radiat Oncol Biol Phys. 2013;85:415–420.
- Carabelli G. Systematisches Handbuch der Zahnheilkunde. 2nd ed. Vienna: Braumuller und Seidel; 1844:114.
- Mod D, Mod H, Jha AK. Oral and dental complications of head and neck radiotherapy and their management. J Nepal Health Res Counc. 2013;11:300–304.
From Decisions in Dentistry. March 2021;7(3):36–39.

