
Periodontitis and Cardiovascular Diseases Are the Not-So-Silent Killers
An integrated healthcare approach shows that reducing cardiovascular risk through lifestyle changes and systemic inflammation management can also improve periodontal health — and vice versa.
PURCHASE COURSE
This course was published in the October/November 2025 issue and expires November 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the October/November 2025 issue and expires November 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 490
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the bidirectional relationship between periodontitis and cardiovascular disease.
- Evaluate current evidence on how periodontal therapy influences cardiovascular outcomes, such as blood pressure control and reduction in cardiac biomarkers.
- Identify integrated management strategies that include lifestyle modifications, collaborative care, and tailored treatment planning for patients with coexisting periodontal and cardiovascular conditions.
As the global population ages and patients outlive their teeth, the impact of oral and systemic inflammatory diseases becomes more concerning. Noncommunicable diseases (NCDs) contribute to 41 million deaths each year, with cardiovascular disease (CVD) leading NCD-related mortality. This is an umbrella term that includes many different heart and blood vessel problems and is often divided into four main types: coronary heart disease, cerebrovascular disease, peripheral arterial disease, and aortic disease.1
One of the most widespread yet often overlooked NCDs, periodontitis, affects nearly half of the world’s population and is now strongly linked to CVD, among other major health conditions, including diabetes mellitus, rheumatoid arthritis, and chronic kidney disease.2-7 The American Heart Association (AHA) recognizes that periodontal disease shares common risk factors and co-morbidities with CVD, but their association is merely that — an association without causality.1,7 However, strategies aimed at reducing cardiovascular risk, such as lifestyle modifications and management of systemic inflammation, may positively impact periodontal health and vice versa.
Pathophysiology
Periodontitis and CVD have similar patient profiles, including men, smokers, obese or overweight, those with self-reported or diagnosed type 2 diabetes mellitus, and/or those from low socioeconomic backgrounds.7 These conditions improve and impede each other through direct and indirect relations. Hypertension, for example, the leading risk factor for coronary artery disease, can be influenced by periodontal therapy.8 In a recent meta-analysis, the prevalence of hypertension in adults was higher among those diagnosed with periodontitis. However, after interventional periodontal treatment, blood pressure readings improved.8 Likewise, in a study that followed almost 18,000 patients, those with up to 10 missing teeth had increased CVD-related mortality by 6%.9 This underscores the importance of early and effective periodontal treatment, proper oral hygiene, and regular maintenance to minimize tooth loss and cardiovascular risks.
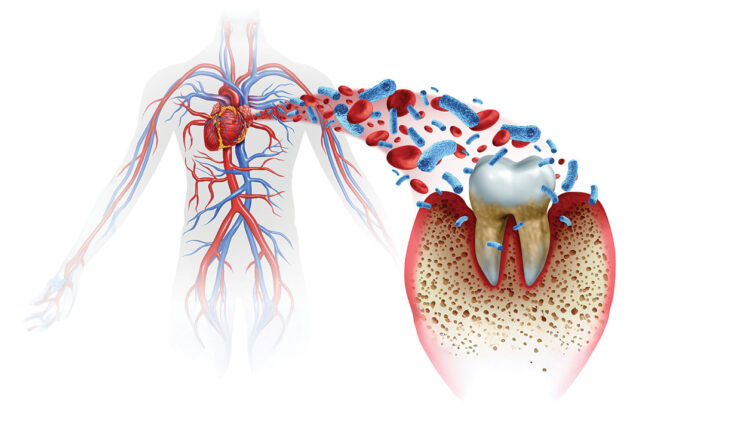
Research has long shown that periodontal diseases may contribute to the development or progression of cardiovascular conditions through direct bacterial dissemination or heightened systemic inflammation.5 Oral bacteria and their byproducts enter the bloodstream via the ulcerated epithelium after brushing or chewing or after professional intervention, including subgingival scaling and root planing in addition to periodontal and oral surgery.10
These bacteria hijack host immune cells in the bloodstream and travel to distant sites, including the cardiovascular system. Polymerase chain reaction assays discovered oral bacteria in atherosclerotic plaques. For example, Streptococcus mutans was found in 78% of cardiovascular specimens containing thrombus tissue. Other periodontal pathogens, such as Aggregatibacter actinomycetemcomitans, Tannerella forsythia, Prevotella intermedia, and Porphyromonas gingivalis, have also been identified.11-14 Despite the growing body of evidence, the precise mechanism by which periodontal pathogens influence atherosclerotic plaques remains unclear.
Even without their migration, periodontal bacteria spawn inflammatory cascades that form these plaques and sustain systemic inflammation, favoring bone resorption and poor wound healing.5,6 Peripheral neutrophils, stimulated by red complex bacteria in periodontal patients, produce elevated levels of reactive oxygen species, which contribute to vascular inflammation and damage release. They also release pro-inflammatory cytokines, such as tumor necrosis factor-alpha, interleukin-1 (IL-1), and IL-6, that lead to atherosclerosis.5,15 Circulating platelets contribute similarly to the host-immune response, releasing cytokines that recruit and modulate immune cells. Significantly elevated platelet counts were identified in periodontal patients, suggesting another link between the digestive and cardiovascular systems.16
Nonsurgical and surgical interventions have been shown to reduce these inflammatory markers over a 6-month period with improved lipid profiles and surrogate markers for CVD.5 These findings offer a direct biochemical link between periodontitis and CVD.
Cardiovascular Management and Impact
Integrated healthcare approaches with early education and intervention are key to improving health outcomes. Patients should be informed of the bidirectional risks of their poor periodontal and/or cardiovascular conditions by both their dental and medical teams. For example, periodontal patients were followed for 13 years, and the severity of their diagnosis was related to CVD events with “severe” cases being four times more likely to have coronary heart disease or stroke.17 These findings were reinforced by a recent systematic review and meta-analysis, which found an increased CVD risk in individuals with periodontitis, highest among those with a severe diagnosis.18 When examining the most vulnerable of these populations, one study of geriatric patients diagnosed with periodontitis grade B or C also reported an increased CVD risk, independent of risk factors such as smoking.19
This information should be used to educate and motivate patients to initiate prompt and effective periodontal therapy. Nonsurgical therapy lowers cardiac biomarker concentrations in patients with chronic periodontitis.20 Effective periodontal treatment was shown to reduce the incidence of acute CVD events, with poor responders experiencing a higher number of acute CVD events.21
Providers should stress the importance of proper self-care as part of these visits. In a large cross-sectional study, subjects who brushed their teeth less than once daily had the highest incidence of acute CVD events.22 A prospective cohort study based on the National Health Insurance System reported that poor oral hygiene, periodontal diseases, and/or tooth loss, were associated with a higher risk of major cardiovascular events, including myocardial infarction, heart failure, and stroke. Just one additional brushing activity per day reduced acute CVD risk, with professional prophylaxes offering further protection.23
But it’s more than just toothbrushing. Poor flossing behavior was associated with higher prevalence of cardiovascular events, increased rick of CVD mortality, and elevated C-reactive protein.24 Taken together, achieving and preserving oral health through effective periodontal treatment, good self-care, and routine maintenance can minimize the risk of cardiovascular diseases. Efforts should be made by dental and medical professionals to improve nutritional habits and lifestyle changes that support oral and overall health.
Common Medications and Side Effects
The impact of medications that manage a variety of cardiovascular diseases, such as high blood pressure or angina, is often overlooked, especially from prescribing physicians. Calcium channel blockers are a drug class that leads to drug-influenced gingival enlargement, according to the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions.25 About one in four patients taking these drugs exhibit this condition, as plaque bacteria is also required to illicit a gingival response. The dosage and duration of these medications is inconsistent with conditional onset, which takes from 40 days up to 6 months.25
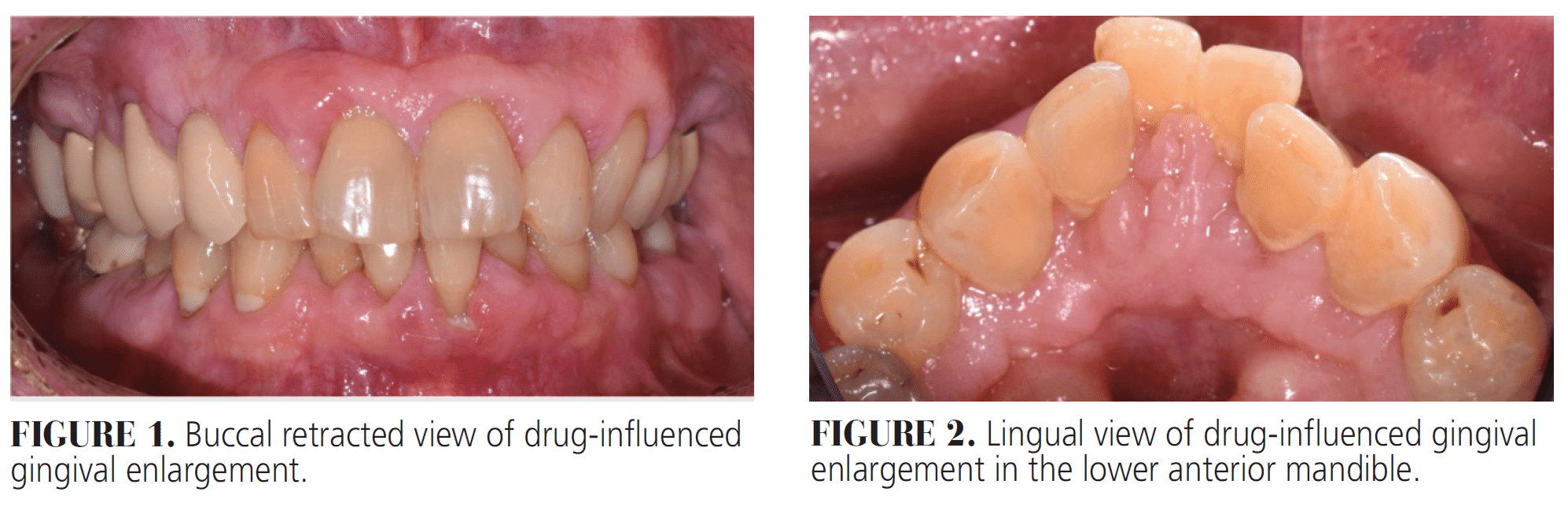
Gingival enlargement usually presents with thick, fibrotic tissues and pebbly or cobblestone-like papillae around the anterior teeth and interproximally more posteriorly (Figures 1 and 2). It is not associated with attachment or tooth loss and tends to be more prominent in the buccal than lingual gingiva and in the maxilla than the mandible.25,26
A histologic sample would reveal increased fibroblasts, collagen, and inflammatory cells.26 This occurs through one of several mechanisms: an upregulated macrophage phenotype that increases osteoblastic activity; increased collagen production via a dysregulation of matrix metalloproteinase (MMP) and tissue inhibitors of MMP activity; and decreased fibroblast apoptosis, leading to an overproduction of collagen and extracellular matrix fibers.26 The resulting hyperplastic tissue complicates oral hygiene, causing increased plaque accumulation and inflammation. Left untreated, this can lead to esthetic and functional disabilities, making way for the progression of periodontal diseases.26,27
As part of the initial workup, dentists should discern whether the patient’s medications are contributing to their gingival condition. If calcium channel blockers, in fact, have led to drug-influenced gingival enlargement, the prescribing physician should be informed of this adverse effect with advisement to consider a different anti-hypertensive or angina drug class.27 This will minimize relapse and offer more complete resolution of their symptoms.
Depending on the severity and extent of hyperplastic tissue and related periodontal breakdown, nonsurgical or surgical treatment should be discussed.27,28 This can include gingivectomy or osseous surgery for patients with suprabony and infrabony defects, respectively. In the very least, frequent professional cleanings and proper self-care should be discussed. If patients cannot discontinue their current medication regimen, they should be seen for one additional recare visit, up to four annually, and undergo surgery as needed, understanding tissue regrowth is inevitable.28
Other CVD-related medications, including blood thinners, directly impact the perioperative period. Most patients on these medications, such as warfarin, antiplatelet, and newer direct-acting oral anticoagulants (eg, apixaban, rivaroxaban), do not need to discontinue their therapy before most dental interventions.29 Current evidence suggests that local measures, such as pressure, hemostatic agents, and suturing, can effectively manage bleeding risks during minor surgical procedures. The American Dental Association (ADA) also notes that for procedures with low to moderate bleeding risk, including extractions of one to three teeth, periodontal surgery, incision and drainage of a localized abscess, and implant placement, the continuation of anticoagulant therapy generally results in minimal bleeding, which can be controlled.29,30
For patients on warfarin or antiplatelet agents, such as clopidogrel, studies show no increased bleeding risk when continuing medication during dental treatments.30,31 The ADA recommends that any modification to anticoagulant therapy should be made in consultation with the patient’s physician. Additionally, the management of direct-acting oral anticoagulants is supported by limited evidence but suggests that these medications do not need to be altered before most dental procedures to uphold patient safety.29,31
Clinical Recommendations
Prescribing physicians should better understand the role of polypharmacy on the oral environment, and it is the responsibility of dentists to bridge this knowledge gap. Oral health professionals are often the first to recognize changes in patients’ oral and/or overall health due to a strict recare frequency. The following outlines clinical recommendations for patients with CVD:
- Comprehensive Examination
Perform a thorough review of their medical history, oral evaluation, and risk assessment. - Risk Communication
Inform patients of the local, systemic, and environmental risk factors that may be exacerbating their periodontal and cardiovascular conditions. Emphasize the bidirectional pathways of these diseases. - Behavioral Modifications
Encourage patients to initiate positive lifestyle changes such as tobacco cessation, improved diet and exercise, proper oral hygiene, and regular maintenance. - Treatment Planning
Develop a personalized plan that considers management and maintenance of their oral and overall health needs. Inform the prescribing physician of any medications that may affect treatment or treatment outcomes. - Antibiotic Prophylaxis
Premedicate patients at risk of infective endocarditis undergoing any procedure that involves gingival tissue manipulation, the periapical region, or perforation of the oral mucosa, following current AHA guidelines. - Nonsurgical Therapy
Initiate timely and effective scaling and root planing to prevent disease progression. Good oral hygiene and lifestyle modifications should be reinforced each visit. - Surgical Periodontal and Implant Therapy
Special considerations should again be made for patients undergoing concomitant anti-hypertensive or anticoagulant/antiplatelet therapy with their medical team to ensure a safe and comfortable experience. - Recare
Patients should be maintained at a recare interval consistent with their periodontal, caries, and occlusal risk factors. Patients unable to undergo more advanced treatment should be seen for one more recare visit annually, up to four.
Patients should be maintained at a recare interval consistent with their periodontal, caries, and occlusal risk factors. Patients unable to undergo more advanced treatment should be seen for one more recare visit annually, up to four.
Conclusions
The growing body of evidence linking periodontitis and CVD underscores the urgent need for a more integrated and holistic approach to healthcare. These two conditions share common risk factors, and their bidirectional relationship highlights the importance of early detection, prevention, and coordinated care. Effective periodontal treatment, personalized oral hygiene, and lifestyle modifications can not only enhance oral health but also contribute to improved cardiovascular outcomes, ultimately, reducing the global burden of non-communicable diseases. The guidelines presented in this article provide valuable direction for both dental and medical professionals, emphasizing the need for collaborative, patient-centered care. By working together to educate patients and manage these interconnected conditions, healthcare providers can significantly improve long-term health outcomes and overall quality of life.
References
- Roth GA, Johnson C, Abajobir A, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70:1-25.
- Sanz M, Del Castillo AM, Jepsen S, et al. Periodontitis and cardiovascular diseases: consensus report. J Clin Periodontol. 2020;47:268-288.
- Chapple IL, Genco R, working group 2 of the joint EFP/AAP. Diabetes and periodontal diseases: consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J Periodontol. 2013;84:S106-112.
- Dietrich T, Sharma P, Walter C, Weston P, Beck J. The epidemiological evidence behind the association between periodontitis and incident atherosclerotic cardiovascular disease. J Periodontol. 2013;84:S70-584.
- Herrera D, Sanz M, Shapira L, et al. Periodontal diseases and cardiovascular diseases, diabetes, and respiratory diseases: Summary of the consensus report by the European Federation of Periodontology and WONCA Europe. Eur J Gen Pract. 2024;30:2320120.
- Linden GJ, Lyons A, Annapieco FA. Periodontal systemic associations: review of the evidence. J Periodontol. 2013;84:S8-S19.
- Sharma P, Dietrich T, Ferro CJ, Cockwell P, Chapple IL. Association between periodontitis and mortality in stages 3-5 chronic kidney disease: NHANES III and linked mortality study. J Clin Periodontol. 2016;43:104-113.
- Hopkins S, Gajagowni S, Gadeer Y, et al. Oral Health and cardiovascular disease. Am J Med. 2024;137:304-306.
- Shen R, Chen S, Shen J, Lv L, Wei T. Association between missing teeth number and all-cause and cardiovascular mortality: NHANES 1999-2004 and 2009-2014. J Periodontol. 2024;95:571-581.
- Reyes L, Herrera D, Kozarov E, Rolda S, Progulske-Fox A. Periodontal bacterial invasion and infection: contribution to atherosclerotic pathology. J Periodontol. 2013;84:S30-50.
- Cortelli JR, Cortelli SC, Jordan S, Haraszthy VI, Zambon JJ. Prevalence of periodontal pathogens in Brazilians with aggressive or chronic periodontitis. J Clin Periodontol. 2005;32:860-866.
- Nakano K, Nemoto H, Nomura R, et al. Detection of oral bacteria in cardiovascular specimens. Oral Microbiol Immunol. 2009;24:64-68.
- Rafferty B, Jonsson D, Kalachikov S, et al. Impact of monocytic cells on recovery of uncultivable bacteria from atherosclerotic lesions. J Intern Med. 2011;270:273-280.
- Kozarov EV, Dorn BR, Shelburne CE, Dunn WA, Jr., Progulske-Fox A. Human atherosclerotic plaque contains viable invasive Actinobacillus actinomycetemcomitans and Porphyromonas gingivalis. Arterioscler Thromb Vasc Biol. 2005;25:e17-18.
- Matthews JB, Wright HJ, Roberts A, Cooper PR, Chapple IL. Hyperactivity and reactivity of peripheral blood neutrophils in chronic periodontitis. Clin Exp Immunol. 2007;147:255-264.
- Sokos D, Laine ML, Nicu EA, et al. Periodontitis and platelets status: a systematic review with meta-analysis and trial sequential analysis. J Periodontol Res. 2025 Mar 11.
- Tiensripojamarn N, Lertpimonchai A, Tavedhikul K, et al. Periodontitis is associated with cardiovascular diseases: A 13-year study. J Clin Periodontol. 2021;48:348-356.
- Larvin H, Kang J, Aggarwal VR, Pavitt S, Wu J. Risk of incident cardiovascular disease in people with periodontal disease: A systematic review and meta-analysis. Clin Exp Dent Res. 2021;7:109-122.
- Petrenya N, Hopstock LA, Holde GE, Oscarson N, Jonsson B. Relationship between periodontitis and risk of cardiovascular disease: Insights from the Tromso Study. J Periodontol. 2022;93:1353-1365.
- Fazal I, Shetty B, Yadalam U, Khan SF, Nambiar M. Effectiveness of periodontal intervention on the levels of N-terminal pro-brain natriuretic peptide in chronic periodontitis patients. J Circ Biomark. 2022;11:48-56.
- Holmlund A, Lampa E, Lind L. Poor response to periodontal treatment may predict future cardiovascular disease. J Dent Res. 2017;96:768-773.
- de Oliveira C, Watt R, Hamer M. Toothbrushing, inflammation, and risk of cardiovascular disease: results from Scottish Health Survey. BMJ. 2010;340:c2451.
- Park SY, Kim SH, Kang SH, et al. Improvemed oral hygiene care attenuates the cardiovascular risk of oral health disease: a population-based study from Korea. Eur Heart J. 2019;40:1138-1145.
- Philip N, Tamimi F, Al-Sheebani A et al. The effect of self-reported flossing behavior on cardiovascular disease events and mortality. J Am Dent Assoc. 2025;156:17-26.
- Murakami S, Mealey BL, Mariotti A, Chapple ILC. Dental plaque-induced gingival conditions. J Periodontol. 2018;89 Suppl 1:S17-S27.
- Trackman PC, Kantarci A. Molecular and clinical aspects of drug-induced gingival overgrowth. J Dent Res. 2015;94:540-46.
- Mainas G, Santamaria P, Zoheir N, et al. Association between calcium-channel blockers and gingival enlargement: A case-control study. J Dent. 2024;149:105315.
- Morikawa S, Nasu M, Miyashita Y, Nakagawa T. Treatment of calcium channel blocker-induced gingival overgrowth without modifying medication. BMI Case Rep. 2021;14:1.
- Hupp WS. Cardiovascular diseases. In: Patton LL, Glick M, eds. The ADA Practical Guide to Patients with Medical Conditions. 2nd ed. Hoboken, New Jersey: John Wiley & Sons, Inc; 2016:25-42.
- Chahine J, Khoudary MN, Nasr S. Anticoagulation use prior to common dental procedures: a systematic review. Cardiol Res Pract. 2019:2019:9308631.
- Manfredi M, Dave B, Percudani D, et al. World workshop on oral medicine VII: Direct anticoagulant agents management for invasive oral procedures: A systematic review and meta-analysis. Oral Dis. 2019;25(Suppl 1):157-1s73.
From Decisions in Dentistry. October/November 2025;11(5):40-45.

