

Saliva Is a Diagnostic Powerhouse
Salivary diagnostics and oral microbiome research are rapidly expanding, positioning saliva as a powerful, noninvasive tool for disease detection and systemic health monitoring.
PURCHASE COURSE
This course was published in the October/November 2025 issue and expires November 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the October/November 2025 issue and expires November 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 430
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the biological composition of saliva and its role as a diagnostic fluid.
- Discuss current advancements in salivary diagnostics and oral microbiome research.
- Identify the challenges and limitations preventing widespread clinical adoption of salivary testing.
In 2024, nearly 300 studies on salivary diagnostics and more than 600 on the oral microbiome appeared on PubMed, showcasing an extraordinary two- to six-fold increase since 2014. This surge in research is more than just a numerical trend, it marks a pivotal shift in the understanding of health — the mouth is not merely a conduit for food and speech, but also serves as a crucial window into the body’s overall well-being. Researchers are tapping into the potential of saliva and oral microbes as accessible, noninvasive biomarkers, unlocking revolutionary possibilities in disease detection and prevention. This shift has the potential to transform how health is addressed, making early diagnosis and health monitoring more attainable than ever before.
One catalyst behind this piqued interest may be the COVID-19 pandemic. The demand for rapid, cost-effective viral detection placed saliva as a credible diagnostic fluid.1 The abundance of data collected during this period enabled numerous studies, some linking the oral microbiome to SARS-CoV-2 complications, and others showing saliva’s comparable sensitivity to traditional nasopharyngeal tests for viral detection.1–3 Additionally, up to 30% of the salivary proteome overlaps with the plasma proteome, underscoring saliva’s potential as a noninvasive means for disease detection.4
Building on these discoveries, diagnostic technology has rapidly advanced, offering promising, convenient, and cost-effective solutions. The field has progressed significantly in a short time, reinforcing its potential for future clinical applications. However, clinical criteria for widespread adoption remain underdeveloped and logistical challenges hinder integration to chairside settings.5 As interest in salivary diagnostics grows, assessing its promise as a new resource is crucial while maintaining a critical perspective.
Understanding Saliva and Its Components
Saliva is a multifaceted bodily fluid essential for maintaining oral health. It plays vital roles in antimicrobial defense, digestion, wound healing, pH regulation, tooth protection, debris removal, taste, and smell.6,7 Experiments in mice show that mixing saliva with blood accelerates wound healing due to the presence of growth factors.6,8 Saliva also acts as a first defense against harmful substances, triggering reflexive spitting.6
Saliva can be defined in two forms: salivary fluid (an exocrine secretion) and total saliva, which includes gingival crevicular fluid, mucosal transudate, nasal and pharyngeal secretions, oral bacteria, food debris, desquamated epithelial cells, and medication byproducts. Its composition of 99% water and 1% electrolytes, proteins, lipids, glucose, and RNA, varies with hydration, posture, medications, and circadian rhythms.8 The major salivary glands —parotid, sublingual, and submandibular — produce about 1 to 1.5 liters of saliva daily, but evaporation and mucosal absorption reduces total output to roughly 0.6 liters.6 An 8% decrease in bodily water content can nearly halt salivary flow as the body attempts to conserve fluids.8 Thus, salivary flow and composition depend largely on individual circumstances.
Beyond its chemical makeup, saliva harbors more than 700 organic bacterial species, making the oral microbiome the second largest in the human body after the gut.9 A single milliliter of saliva contains approximately 108 microbial cells, influencing immune responses and metabolic processes. While a universally accepted definition of a “healthy” oral microbiome has yet to be established, a stable, balanced microbial environment generally indicates health. Dysbiosis, an imbalance favoring pathogens, often signals disease.10 Monitoring microbial composition and identifying problematic bacteria could therefore aid in disease prevention.
Lately, research has focused on microbial function rather than mere presence, leading to more specific treatments targeting dysbiosis. This evolving perspective addresses the notion that different species may perform similar functions in disease states.10 Saliva and the oral microbiome interact bidirectionally, as saliva provides an attachment medium for bacteria, while bacteria influence physiological, metabolic, and immune responses.9 While saliva’s antibacterial properties alone cannot eliminate pathogens, they help regulate harmful bacteria when paired with proper oral hygiene.6
The ability to isolate and analyze salivary biomarkers has fueled interest in saliva as a diagnostic tool. Studies have explored its potential in detecting systemic diseases, oral conditions, nutritional status, and even cancer. However, challenges remain in the widespread adoption of salivary diagnostics. Skepticism persists due to a lack of comprehensive databases and standardized protocols. While some view salivary testing as a groundbreaking step, others remain cautious about its reliability. Until salivary diagnostics can produce consistent, reproducible, accurate, and clinically validated results, its role in healthcare will continue to be a subject of debate.
Benefits of Salivary Testing
Saliva offers a practical, noninvasive, and attractive alternative to blood testing. Its accessibility and ease of collection make it a convenient diagnostic medium, especially in dental settings.6 Many individuals visit the dentist biannually, providing an opportunity for routine health monitoring through saliva collection. Key areas of salivary diagnostics include salivaomics, salivary exosomes, and saliva liquid biopsy, with applications in early disease detection and cancer screening.4,7 In short, salivaomics examines the molecular components of saliva using bulk sampling, salivary exosomes (small, membrane-bound vesicles that carry cell-specific information) and liquid biopsy techniques that detect tumor-derived biomarkers.4
The effectiveness of salivary diagnostics largely depends on how biomarkers initially reach saliva. Molecules enter saliva via vascular exchange, intracellular diffusion, and transudation from blood vessels into salivary gland cells.11–13 Additionally, compromised gingival tissues can allow permeation of molecules into the oral cavity. Some biomarkers originate in the oral cavity itself, being absorbed into the bloodstream and then reintroduced into saliva via salivary glands.11,12
Although biomarker concentrations in saliva are lower than in blood, ultra-sensitive technologies have the ability to improve detection.14 Salivary levels of common inflammatory markers, such as C-reactive protein (CRP), tumor necrosis factor-alpha, interleukin-6, and interferon-gamma, have demonstrated correlated levels with serum.13 Additionally, elevated salivary urea has been found in those with chronic renal insufficiency, and individuals with high nitrate diets have shown to possess more nitrate-reducing oral bacteria, playing a role in blood pressure regulation via nitric oxide production.8,15
Combining bacterial identification with salivary molecule detection is an additional layer that may improve diagnostic accuracy. Periodontitis, for example, is strongly associated with the presence of the red complex bacterial consortium and is linked to elevated levels of systemic inflammatory markers, including immunoglobulins and CRP.14,16,17 Similarly, oral microbiome alterations have been linked to oral cancer, gingivitis, dental caries, and oral malodor.10,15,18 These diseases stem from microbial imbalances that enable pathogens to proliferate, disrupt healing, and release harmful byproducts.15 Detecting these markers through salivary testing would allow for disease risk assessment and enable personalized prevention plans.
Beyond oral diseases, systemic diseases increasingly show associations with oral health. The oral cavity is not an isolated system, allowing bacteria and other molecules the opportunity to enter systemic circulation through respiratory and digestive routes. Oral pathogens have been found in the bloodstream of individuals with systemic conditions, and studies link oral dysbiosis to systemic disease progression and severity.15,19 Even transient bacterial exposure can trigger inflammation, stimulate osteoclasts, and interfere with coagulation due to effects of their byproducts.18 Correlations have been established with cystic fibrosis, autoimmune diseases, Alzheimer disease, cardiovascular disease, diabetes, preterm birth, and various cancers.10,19 A recent study linked elevated levels of Prevotella intermedia, an oral bacterium, to cognitive decline progression in dementia patients.20
While these relationships remain correlative rather than causative, they underscore the interconnected nature of human health and support a whole-body approach to medicine. It would be negligent to overlook the oral-systemic connection, as many systemic conditions manifest in the oral cavity, including hormonal changes, autoimmune flares, and viral infections.21 Notably, human immunodeficiency virus/acquired immune deficiency syndrome are often first detected through oral symptoms.22
Challenges and Limitations
While some biomarkers originate in the oral cavity, allowing for reliable measurement, many do not. Proving that salivary biomarker levels accurately reflect plasma concentrations remains a challenge. For instance, despite the correlation between blood and salivary glucose levels, saliva has proven unreliable for monitoring blood glucose.8 Similarly, saliva’s ability to assess nutritional status has yielded inconclusive results, with some dietary markers aligning with plasma levels but lacking sufficient reliability for standalone use.23 Among 27 tested salivary cytokines, only three significantly correlated with plasma levels, and only 15% to 33% of plasma levels of melatonin appeared in the saliva.6,13
Several factors further complicate salivary diagnostics. Time of day, collection site, food intake, mastication, and whether the sample is from stimulated or unstimulated saliva all contribute to clarity and variability.1,4 High-abundance salivary proteins may obscure diagnostically relevant low-abundance proteins, requiring complex preprocessing steps.17 Additionally, the dynamic environment of the oral cavity complicates standardization across individuals. Beyond the variability in saliva samples, biological barriers limit which molecules reach the oral cavity. Most biomarker molecules must cross epithelial linings, evade enzymatic breakdown, and penetrate the phospholipid bilayer of membranes before entering salivary fluid.12 Protease and ribonuclease inhibitors are required to preserve samples, assuming molecules have withstood enzymatic degradation at the time of collection.4 Salivary exosomes may offer a solution by encapsulating biomarkers within a lipid bilayer, but this approach requires further validation.4,7
The oral microbiome adds complexity, as its composition varies by individual, lifestyle, and collection site.5,9,15 Much of the current understanding of the oral microbiome and disease is derived from animal models, and, although more longitudinal studies on humans are being conducted, interindividual variability further complicates standardization.18
Even if a representative sample is obtained from saliva, the lack of standardized collection and processing protocols poses hurdles. With salivary diagnostics still in its nascent stages, there is no universally accepted method for sample collection, processing, or analysis. This variability makes it difficult to compare findings across studies with confidence.
Economic considerations further hinder widespread adoption in dental settings. Equipment costs and lab fees for processing and analyzing the collected data are considerations. Development of the necessary technology may be reaching advanced stages, but it still requires an investment until per-test costs are reduced and reimbursement models are established.
Current Technology and Future Directions
Advancements in sequencing and detection technologies have enhanced the feasibility of salivary diagnostics. However, laboratories will need to collaborate with industry partners in order to translate research into clinical practice. As interest grows, increased funding will also be crucial to furthering the field. Initiatives are already in place, with a National Institute of Dental and Craniofacial Research-supported research consortium compiling a list of whole saliva proteins that overlap with plasma proteins and National Institutes of Health programs such as the Extracellular RNA Communication Consortium and Rapid Accelerated Diagnostic exploring salivary biomarker databases.4,7,13
Salivary proteome and transcriptome databases now catalog more than 1,000 proteins and 180 mRNAs common in healthy individuals. These growing databases provide crucial baseline profiles for distinguishing between health and disease. One study even demonstrated that the salivary transcriptome outperformed the serum transcriptome in diagnosing oral cancer.14 Although the salivary databases at present focus on oral diseases, their expansion could facilitate systemic disease diagnostics.
Salivary exosomes are emerging as a promising tool, offering a rich source of information from systemic circulation.7 A new technology, EFIRM, developed at the University of California, Los Angeles, School of Dentistry, allows for direct, on-site biomarker detection within salivary exosomes. This quick, efficient, and cost-effective method is an instrumental step toward salivary diagnostics, reducing reliance on time-consuming, costly, and often unreliable polymerase chain reaction techniques.4,5,7 Further, point-of-care diagnostics, including “lab-on-a-chip” technology, aim to condense laboratory analyses into a single, portable device.24,25 Refining these devices to create cost-effective designs would significantly improve the hurdles preventing clinicians from its incorporation into practice, especially if mass produced.
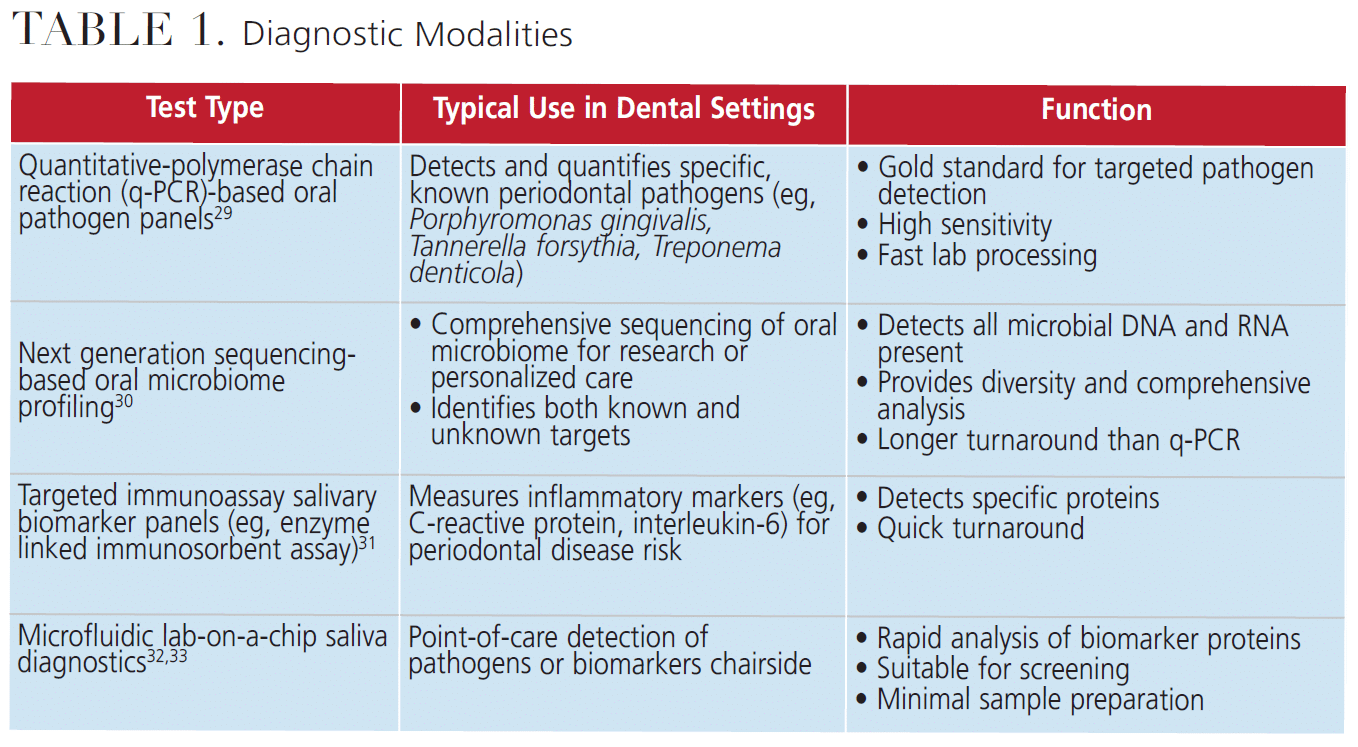
In addition to diagnostics, the potential of therapeutic agents to restore microbial balance is being explored. Probiotics, prebiotics, and peptides may be useful adjuncts to target certain oral conditions, such as caries, gingivitis, and oral malodor. However, more research is needed before microbiome-targeted therapies can be safely implemented.21,26,27 Next-generation sequencing techniques are advancing the study of the oral microbiome, detecting organisms beyond exclusively bacteria and expanding the understanding of microbial interactions.15,18 Still, further research is needed before microbiome-targeted therapies can be reliably implemented. Table 1 lists various methods, both established and emerging, used for microscopic analysis of salivary samples.29-33
Ensuring bioavailability must also be considered with oral therapeutics. Many supplements degrade before reaching their target, making effective delivery systems essential. Bioadhesive drug delivery systems, such as microspheres for prolonged gastric retention, are being developed to enhance absorption, but hurdles still remain.28
Conclusion
As technology continues to advance and databases expand, salivary diagnostics is becoming increasingly viable for clinical use. As this field develops, standardized protocols and ultrasensitive detection methods will need to be developed to fully harness saliva’s potential as a diagnostic tool. Gaining a deeper understanding of the connection between oral and systemic health could pave the way for more personalized medicine, thereby reducing side effects and improving treatment outcomes.21 Although the potential of salivary diagnostics is promising, further research is necessary to completely unlock its capabilities.
Despite the current advances, salivary testing remains uncommon in everyday dental settings. The additional costs and chairside time inevitably accompanying these tests bring barriers to the chairside use of salivary diagnostics, especially with the skepticism on efficacy and uncertainties regarding reimbursement. Until salivary diagnostics gains more credibility and standardization, its adoption into clinical use will likely be slow and prolonged, even in the face of promising technological development.
References
- Oliveira Neto NF de, Caixeta RAV, Zerbinati RM, et al. The emergence of saliva as a diagnostic and prognostic tool for viral infections. Viruses. 2024;16:1759.
- Sampson V, Kamona N, Sampson A. Could there be a link between oral hygiene and the severity of SARS-CoV-2 infections? Br Dent J. 2020;228:971-975.
- Atieh MA, Guirguis M, Alsabeeha NHM, Cannon RD. The diagnostic accuracy of saliva testing for SARS-CoV-2: A systematic review and meta-analysis. Oral Dis. 2022;28 Suppl 2:2347-2361.
- Nonaka T, Wong DTW. Saliva diagnostics: Salivaomics, saliva exosomics, and saliva liquid biopsy. J Am Dent Assoc. 2023;154:696-704.
- Kaczor-Urbanowicz KE, Martin Carreras-Presas C, Aro K, Tu M, Garcia-Godoy F, Wong DT. Saliva diagnostics: Current views and directions. Exp Biol Med (Maywood). 2017;242:459-472.
- Dawes C, Pedersen AML, Villa A, et al. The functions of human saliva: A review sponsored by the World Workshop on Oral Medicine VI. Arch Oral Biol. 2015;60:863-874.
- Nonaka T, Wong DTW. Saliva diagnostics. Annual Rev Anal Chem. 2022;15:107-121. doi:10.1146/annurev-anchem-061020-123959
- de Almeida PDV, Grégio AMT, Machado MAN, de Lima AAS, Azevedo LR. Saliva composition and functions: a comprehensive review. J Contemp Dent Pract. 2008;9(3):72-80.
- Deo PN, Deshmukh R. Oral microbiome: Unveiling the fundamentals. J Oral Maxillofac Pathol. 2019;23:122-128.
- Willis JR, Gabaldón T. The human oral microbiome in health and disease: from sequences to ecosystems. Microorganisms. 2020;8:308.
- Naumova EA, Dierkes T, Sprang J, Arnold WH. The oral mucosal surface and blood vessels. Head Face Med. 2013;9:8.
- Malamud D. Saliva as a diagnostic fluid. Dent Clin North Am. 2011;55:159-178.
- Desai GS, Mathews ST. Saliva as a non-invasive diagnostic tool for inflammation and insulin-resistance. World J Diabetes. 2014;5:730-738.
- Wong DT, Segal A, Wong DT. Salivary diagnostics: enhancing disease detection and making medicine better. Eur J Dent Educ. 2008;12:22-29.
- Rajasekaran JJ, Krishnamurthy HK, Bosco J, et al. Oral microbiome: a review of its impact on oral and systemic health. Microorganisms. 202412:1797.
- Mehrotra N, Singh S. Periodontitis. In: StatPearls. Treasure Island, Florida: StatPearls Publishing; 2025.
- Wang Q, Yu Q, Lin Q, Duan Y. Emerging salivary biomarkers by mass spectrometry. Clin Chim Acta. 2015;438:214-221.
- Baker JL, Mark Welch JL, Kauffman KM, McLean JS, He X. The oral microbiome: diversity, biogeography and human health. Nat Rev Microbiol. 2024;22:89-104.
- Peng X, Cheng L, You Y, et al. Oral microbiota in human systematic diseases. Int J Oral Sci. 2022;14:14.
- L’Heureux JE, Corbett A, Ballard C, et al. Oral microbiome and nitric oxide biomarkers in older people with mild cognitive impairment and APOE4 genotype. PNAS Nexus. 2025;4:543.
- Zarco MF, Vess TJ, Ginsburg GS. The oral microbiome in health and disease and the potential impact on personalized dental medicine. Oral Dis. 2012;18:109-120.
- Lomelí-Martínez SM, González-Hernández LA, Ruiz-Anaya A de J, et al. Oralmanifestations associated with HIV/AIDS patients. Medicina (Kaunas). 2022;58:1214.
- Logan D, Wallace SM, Woodside JV, McKenna G. The potential of salivary biomarkers of nutritional status and dietary intake: a systematic review. J Dent. 2021;115:103840.
- Arshavsky-Graham S, Segal E. Lab-on-a-chip devices for point-of-care medical diagnostics. In: Bahnemann J, Grünberger A, eds. Microfluidics in Biotechnology. Cham, Switzerland: Springer International Publishing; 2020:247-265.
- Özyurt C, Uludağ İ, İnce B, Sezgintürk MK. Lab-on-a-chip systems for cancer biomarker diagnosis. J Pharm Biomed Anal. 2023;226:115266.
- Inchingolo F, Inchingolo AM, Malcangi G, et al. The benefits of probiotics on oral health: systematic review of the literature. Pharmaceuticals (Basel). 2023;16:1313.
- Shirbhate U, Bajaj P, Chandak M, et al. Clinical implications of probiotics in oral and periodontal health: a comprehensive review. Cureus. 2023;15:51177.
- Alqahtani MS, Kazi M, Alsenaidy MA, Ahmad MZ. Advances in oral drug delivery. Front Pharmacol. 2021;12:618411.
- Van Der Weijden F, Rijnen M, Valkenburg C. Comparison of three qPCR-based commercial tests for detection of periodontal pathogens. Sci Rep. 2021;11:6141.
- Zhang Y, Qi Y, Lo ECM, McGrath C, Mei ML, Dai R. Using next‐generation sequencing to detect oral microbiome change following periodontal interventions: A systematic review. Oral Diseases. 2021;27:1073-1089.
- Zhang Y, Kang N, Xue F, et al. Evaluation of salivary biomarkers for the diagnosis of periodontitis. BMC Oral Health. 2021;21:266.
- Herr AE, Hatch AV, Throckmorton DJ, et al. Microfluidic immunoassays as rapid saliva-based clinical diagnostics. Proc Natl Acad Sci USA. 2007;104:5268-5273.
- Zhang Y, Liu Y. Advances in integrated digital microfluidic platforms for point-of-care diagnosis: a review. Sens Diagn. 2022;1:648-672.
From Decisions in Dentistry. October/November 2025;11(5):36-39.

