

Why Dental Hygienists Belong on the Endodontic Team
As endodontists face rising demand and growing burnout, integrating dental hygienists as co-therapists offers a smart solution to enhance care, improve efficiency, and reduce stress.
Endodontics is a dental specialty that specializes in the diagnosis, prevention, and treatment of diseases and injuries affecting the dental pulp and surrounding root tissues.1,2 The dental pulp, located inside the tooth, contains blood vessels, nerves, and connective tissue essential for tooth health.1 The most common endodontic procedure is root canal therapy, which involves removing inflamed or infected pulp, cleaning, disinfecting, shaping the root canal system, and sealing it to prevent reinfection.1–3 Endodontists specialize in treating the dental pulp and managing complex cases involving tooth pain, infections, and dental trauma.1,3 Additionally, they perform apicoectomies, which remove the tooth’s root tip and then seals it to treat persistent infections.1,2 Endodontists also specialize in dental trauma, including treating fractured, dislodged, or avulsed teeth to preserve function and esthetics.2 Endodontic care plays a critical role in saving natural teeth, which is vital for maintaining oral health, ensuring proper chewing function, and preserving the esthetics and integrity of the overall dental structure.
Diagnosing endodontic conditions requires a thorough and systematic approach.4 Endodontists must integrate detailed inquiry, diagnostic testing, and critical reasoning to ensure an accurate diagnosis and create an effective treatment plan.4 Unfortunately, there is nationwide shortage of endodontists and those currently practicing face a high rate of burnout due to increased desire by older adults to maintain their natural dentition as well as persistent dental workforce shortages.5 The shortage of endodontists is attributed to the specialized education required after dental school, the limited number of spots in specialty programs, and the significant financial burden associated with the cost of dental education.5 To alleviate the stress caused by the shortage and high burnout rates, measures must be taken to address and reduce the shortage.
Incorporating Dental Hygienists
The use of co-therapists in the endodontic setting could help reduce burnout address dental workforce shortages. Dental hygienists, with their comprehensive education in basic, clinical, and behavioral sciences, are well-suited for this role.6 While dental hygienists most often work in general dentistry practices, they are also employed by specialists such as periodontists, prosthodontists, and orthodontists. However, there is currently limited evidence of a widespread shortage of hygienists in specialty practices — particularly among endodontists.7,8 This gap in data highlights a valuable opportunity for further research into employment trends in dental specialty settings.
Because dental hygienists have extensive training and experience in various areas that are essential across all dental fields, including patient assessment, thorough documentation, patient treatment, exposure control protocols, and patient management,6 they are ideal candidates to provide co-therapy in endodontic offices. For instance, addressing dental anxiety is a significant part of successful patient management. The endodontic setting is particularly susceptible to dental anxiety among patients as many fear root canal therapy due to perceived pain and uncertainty about outcomes.9,11–14 Anxious patients may overestimate pain levels, requiring additional chairside time dedicated to stress reduction.9,14 This extended time can increase stress for both the patient and the dental provider.9 Given that successful endodontic treatment depends on precise instrumentation and meticulous disinfection of the root canal system, effectively managing patient anxiety becomes a critical aspect of care, one that dental hygienists are well versed in providing.14
Providing endodontists with the ability to delegate clinical tasks is another benefit of adding dental hygienists to the endodontic team. With dental hygienists performing assessments and providing care within their legal scope and expertise, endodontists are free to concentrate on the specialized clinical services they are trained in. This can lead to more effective patient treatment and higher satisfaction. Additionally, this approach can help reduce burnout for both the endodontist and dental hygienist by offering the hygienist more diverse responsibilities. Given the shortage of endodontists in certain regions and the growing demand for services, studies have shown an increase in rushed appointments, which in turn has led to procedural errors.5,15–19 Endodontists also treat many emergency patients, which can elevate stress levels and complicate scheduling. Delegating tasks to a dental hygienist would likely minimize errors and provide more time for patient care. Many procedures commonly performed by endodontists are within a dental hygienist’s scope of practice but may vary between states.20–22
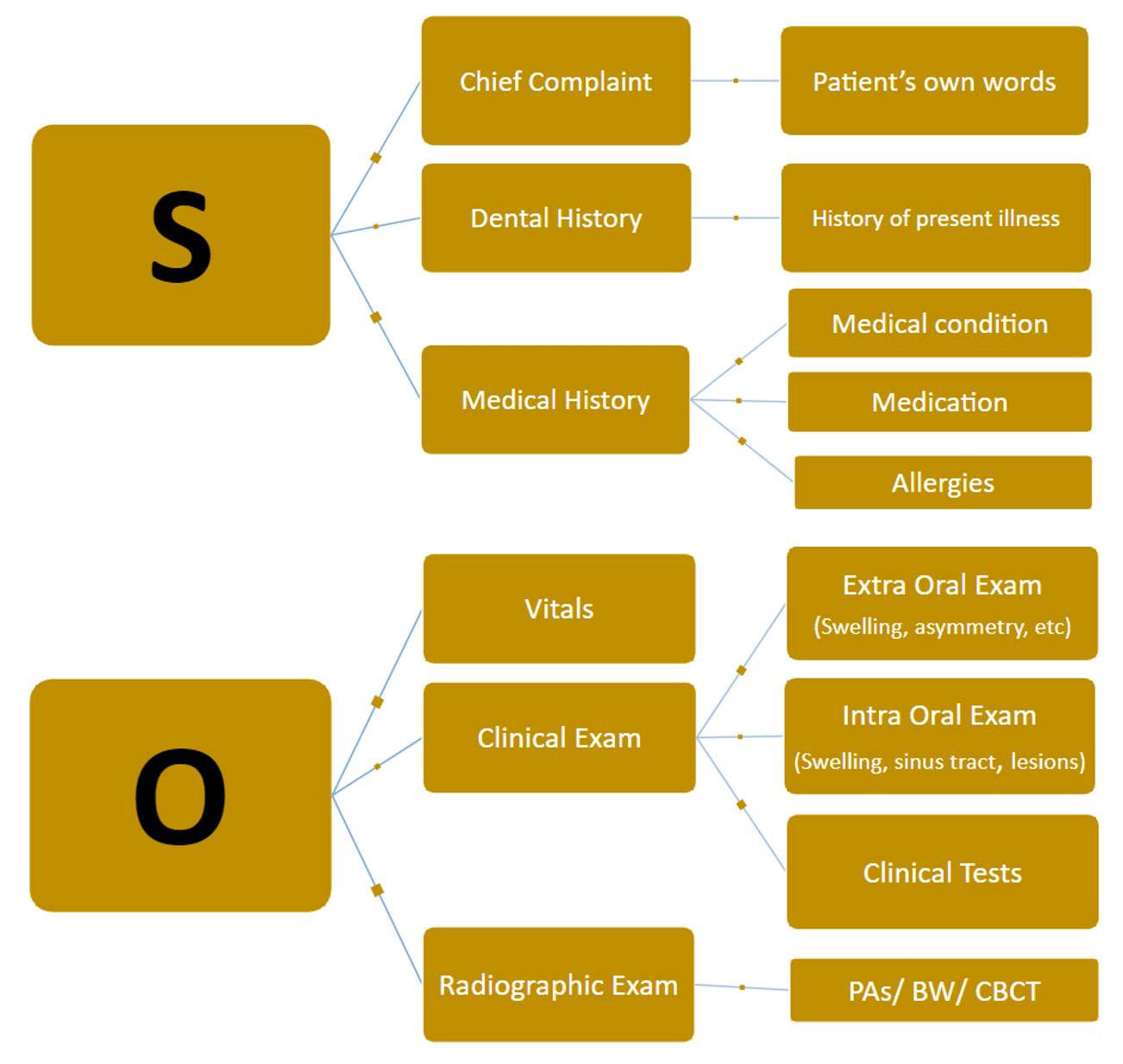
Dental hygienists are highly qualified to assist endodontists in their diagnoses. They are trained to obtain medical and dental histories, ask relevant follow-up questions, assess and evaluate a patient’s vital signs, take quality and diagnostic radiographs, perform diagnostic tests, help interpret results, explain the importance of procedures, and answer personal questions that need to be addressed. Dental hygienists are qualified to perform these tasks due to their education in health history, radiology, pathology, pharmacology, and motivational interviewing.6 They can also perform head and neck exams; evaluate hard and soft tissues for potential lesions, swellings, and pathology; and highlight potential caries to the endodontist, saving them time while also improving patient satisfaction. While some of these tasks can be performed by dental assistants, dental hygienists already possess the necessary education and experience, reducing the need for additional training. Dental hygienists learn about various dental specialties within their educational experience.
Clinical Testing
By conducting thermal tests, dental hygienists can aid in a pulpal diagnosis. The severity of the pulpal condition is suggested by the response to thermal tests (Figure 1).23 When conducting the thermal test, dental hygienists should document the appropriate responses to aid the endodontist in determining the appropriate diagnosis. The results of this test alone do not provide enough information for the endodontist to make a diagnosis, as there are both subjective and objective components to consider (Figure 2).23 Dental hygienists can also help come up with a periapical diagnosis by performing percussion, palpation, and bite tests.6 These tests, combined with radiographic examinations, are essential for a comprehensive endodontic diagnosis conducted by the endodontist.24 Additionally, they are able to probe and check for mobility of the affected tooth to evaluate clinical attachment loss, the condition of the gingiva, and potential perio-endo lesions.
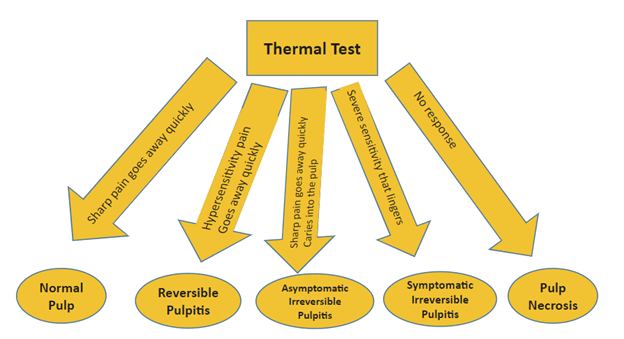
Although dental hygienists cannot diagnose conditions based on these responses, they are able to prepare the patient for potential treatment. For example, if the patient’s response suggests irreversible pulpitis or pulp necrosis, the dental hygienist can educate the patient that root canal therapy may be indicated by the endodontist.23 After the endodontist determines a diagnosis and prognosis, the dental hygienist can explain the findings to the patient and answer any questions. The dental hygienist can also aid in obtaining informed consent from the patient. Utilizing the dental hygienist to gather initial assessments, record findings, and communicate with the patient will save considerable time for the endodontist. Additionally, dental hygienists develop a strong rapport and connection with their patients, thus building the trust some patients need to cooperate with the proposed treatment plan. Although direct research on patient trust specifically related to dental hygienists is limited, existing literature highlights the critical role of trust in dental care and emphasizes that dental hygienists contribute significantly to building this trust through effective communication, empowerment of patients, and patient-centered care.6,25,26 The consistency and reliability of patients attending regular appointments with dental hygienists, combined with effective communication and professional guidance, help to build strong connections and trust between dental hygienists and patients.
After a diagnosis is made by the endodontist, dental hygienists can administer local anesthesia in the 49 states where it is permitted. This is important, as infected teeth often require additional time to achieve adequate anesthesia due to infection and inflammation.2,27,28 Dental hygienists can also provide post-operative instructions. With their training in pharmacology, dental hygienists can provide guidance on the use of antimicrobial rinses, medication instructions, and steps to take in the event of adverse reactions. Dental hygienists can also conduct follow-up calls to address potential complications after treatment or answer patient questions. Similarly, they can assist with routine follow-up appointments to monitor healing progress and support the success of the treatment. After surgical procedures, dental hygienists can aid in removing sutures, providing instructions to promote wound healing, and taking post-operative photos or X-rays.
Conclusion
Dental hygienists are ideal co-therapists for endodontic practices due to their expertise in patient assessment, thorough documentation, treatment, exposure control protocols, and patient management. Delegating tasks to hygienists can enhance patient care, reduce burnout for both endodontists and hygienists, and ultimately improve office morale and cost-efficiency. Endodontist offices would greatly benefit from the inclusion of a dental hygienist within their team.
References
- Carrotte PV. An introduction to endodontics. BDJ Team. 2021;8:31–34.
- Pinto KP, Barbosa AFA, Silva EJNL, Santos APP, Sassone LM. What is the microbial profile in persistent endodontic infections? A scoping review. J Endod. 2023;49:786–798.
- Bennett GW. Multi-material polyjet printing for more lifelike endodontic practice teeth. J Dent Educ. 2023;87 Suppl 3:1852–1853.
- Poly A, Hupp D, Lowry J, Schweitzer JL. An innovative interactive scenario-based approach to teaching endodontic diagnosis. J Dent Educ. 2024;1–3.
- TDIC Risk Management Staff. Haste, pressure and staffing shortages contribute to costly mistakes. J Calif Dent Assoc. 2023;51:1–2.
- Swigart DJ, Gurenlian JR, Rogo EJ. Dental hygiene diagnosis: A qualitative descriptive study of dental hygienists. Can J Dent Hyg. 2020;54:113–123.
- United States Bureau of Labor Statistics. Occupational Employment and Wage Statistics. Available at bls.gov/oes/current/naics4_621200.htm#00-0000. Accessed June 24, 2025.
- Gutmann ME, Gutmann JL. The dental hygienist as a co-therapist in the endodontic practice. J Endod. 1999;25:272–274.
- Alroomy R, Kim D, Hochberg R, Chubak J, Rosenberg P, Malek M. Factors Influencing pain and anxiety before endodontic treatment: A cross-sectional study amongst American individuals. Eur Endod J. 2020;5:199–204.
- Peretz B, Moshonov J. Dental anxiety among patients undergoing endodontic treatment. J Endod. 1998;24:435–437.
- Alghofaily M, Alsalleeh F. Levels of anxiety and fear related to non-surgical root canal treatment performed by endodontic residents and endodontists. Front Dent Med. 2022;3:1–11.
- Dou L, Vanschaayk MM, Zhang Y, Fu X, Ji P, Yang D. The prevalence of dental anxiety and its association with pain and other variables among adult patients with irreversible pulpitis. BMC Oral Health. 2018;18:101.
- White AM, Giblin L, Boyd LD. The prevalence of dental anxiety in dental practice settings. J Dent Hyg. 2017;91:30–4.
- Ahmed S, Sharma P, Mahaprasad A, Patel A, Chohan H, Murugesan S. Assessing the influence of patient anxiety on the efficacy of endodontic procedures. J Pharm Bioallied Sci. 2024;16(Suppl 3):S2685–2687.
- El-Kishawi M, Khalaf K. An update on root canal preparation techniques and how to avoid procedural errors in endodontics. Open Dent J. Available at https://opendentistryjournal.com/VOLUME/15/PAGE/318/FULLTEXT. Accessed June 24, 2025.
- Alrahabi M, Zafar MS, Adanir N. Aspects of clinical malpractice in endodontics. Eur J Dent. 2019;13:450–458.
- Scarlatescu SA, Gheorghiu I, Nicola G, Al Aloul AO, Perlea P. Frequent procedural errors and structural complications on endodontically treated teeth. Ro J Stomatol. 2021;67:101–106.
- Bhuva B, Ikram O. Complications in endodontics. Prim Dent J. 2020;9:52–58.
- Bamini L, Sherwood A, Arias A, Subramani SK, Bhargavi P. Influence of tooth factors and procedural errors on the incidence and severity of post-endodontic pain: a prospective clinical study. Dent J (Basel). 2020;8:73.
- American Dental Hygienists’ Association. Dental hygiene practice act overview: Permitted functions and supervision levels by state. Available at adha.org/wp-content/uploads/2024/09/Practice-Act-Overview-9-2024.pdf. Accessed June 24, 2025.
- American Dental Hygienists’ Association. Professional roles of an RDH. Available at adha.org/education-resources/become-a-dental-hygienist/dental-hygiene-programs/professional-roles-of-an-rdh. Accessed June 24, 2025.
- American Dental Education Association. ADEA compendium of curriculum guidelines. Available at adea.org/docs/default-source/uploadedfiles/uploadedfiles/adea/site-pages/compendiumofcurriculumguidelinesforallieddentaleducationprograms.pdf?sfvrsn=32912efe_1&id=45178. Accessed June 24, 2025.
- American Association of Endodontists. Endodontics: Colleagues for Excellence. Available at aae.org/specialty/publications-research/endodontics-colleagues-excellence/. Accessed June 24, 2025.
- Boreak N. Effectiveness of artificial intelligence applications designed for endodontic diagnosis, decision-making, and prediction of prognosis: A systematic review. Contemp Dent Pract. 2020;21:926–934.
- John D, Raveendranadhan S. Trust between dental professionals and patients: A scoping review. Patient Educ Couns. 2023;109(Supplement):51.
- Moore R. Trusting the dentist — expecting a leap of faith vs a well-defined strategy for anxious patients. Dent J (Basel). 2022;10:66.
- Drum M, Reader A, Nusstein J, Fowler S. Successful pulpal anesthesia for symptomatic irreversible pulpitis. J Am Dent Assoc. 2017;148:267–271.
- Gupta A, Wadhwa J, Aggarwal V, et al. Anesthetic efficacy of supplemental intraligamentary injection in human mandibular teeth with irreversible pulpitis: a systematic review and meta-analysis. J Dent Anesth Pain Med. 2022;22:1–10.
