

The Evolution of Full-Arch Implant Rehabilitation
Advances in materials, digital workflows, and immediate loading protocols have transformed full-arch implant therapy into a precise, efficient, and highly esthetic treatment option.
The journey of dental implants began in the 1950s when Per-Ingvar Brånemark, MD, PhD, made a groundbreaking discovery: osseointegration.1 This process — the direct attachment of bone to an inert, alloplastic material without any intervening fibrous connective tissue — became the foundational principle of modern implantology.2 By the 1980s, Adell et al3 demonstrated that full-arch fixed implant prostheses were possible using six to eight implants, though this often required bone grafting. The field took a significant leap forward in 1998 when Paulo Malo, DDS, PhD, pioneered the All-on-4™ concept. This innovative approach allowed full-arch fixed prostheses to be supported by four strategically placed implants, with the posterior implants tilted up to 30° to maximize bone engagement while avoiding critical anatomical structures.
Numerous clinical studies have since validated the effectiveness of the All-on-4 technique in eliminating the need for bone grafting, reducing treatment time, and enabling immediate loading of provisional prostheses.4-7 As practitioners gained experience, they began adapting this concept to create “All-on-X” variations, where “X” represents the specific number of implants needed for enhanced stability in high-load scenarios. Regardless of the variation, successful implementation requires a minimum of four implants with proper distribution across the dental arch.
Full-arch implant rehabilitation, particularly using All-on-X concepts, frequently incorporates immediate loading protocols that dramatically reduce treatment timelines while enhancing patient satisfaction. These protocols allow clinicians to place implants — whether straight or tilted — in positions that maximize available bone and achieve the primary stability necessary for immediate provisional restorations while achieving proper anterior-posterior relationship.8,9
The ability to provide immediate provisional restorations has transformed the field of full-arch implant rehabilitation, offering patients immediate function and esthetics. This approach has gained widespread acceptance among patients due to several key advantages: reduced or eliminated need for bone grafting, significantly shorter treatment times, and markedly improved function and esthetics compared to traditional multi-stage surgical approaches that rely on removable interim prostheses.
Considerations for Full-Arch Implant Rehabilitation

A critical decision in full-arch rehabilitation is whether to extract the patient’s remaining teeth or preserve them. This choice requires careful consideration based on individual patient factors. Patients’ complete medical and dental history, both past and present, along with their daily oral hygiene practices, play vital roles in predicting the long-term prognosis and success of treatment. An additional consideration is the interdisciplinary collaboration between a prosthodontist and periodontist and/or oral surgeon to best manage the prosthetic and surgical components of the case. Ultimately, the sustainability of any dental treatment depends on the patient’s ability to maintain it over time.
Before recommending full-arch rehabilitation, clinicians should thoroughly assess several critical factors.
Dental History Factors
- Periodontal status and oral hygiene
- When evaluating patients for full-arch rehabilitation, their periodontal status and oral hygiene habits are crucial determinants. Severe periodontal diseases often indicate a poor long-term prognosis for natural teeth, potentially favoring full-arch prosthetic solutions. However, clinicians must identify the underlying cause of the periodontal disease.10
- Studies demonstrate that patients with advanced periodontal conditions face significantly higher risks of tooth loss and reduced implant success due to increased microbial burden and inflammatory responses.11-13
- Past, current, and future caries risk
- Multiple recurrent carious lesions and a history of failing restorations increase the likelihood of needing future restorative interventions, potential tooth loss, and possible implant-supported rehabilitation failure.10
- Conditions causing xerostomia, such as head and neck radiation or polypharmacy, automatically place patients in a high caries risk category. With remaining natural teeth likely requiring ongoing treatment, many patients opt proactively for complete extraction followed by implants to avoid future caries complications.
- Existing restorations and endodontic status
- Multiple failing restorations and endodontically treated teeth may suggest full-arch rehabilitation as a more sustainable long-term solution, though the causes of restoration failure must be thoroughly assessed. Conversely, well-maintained restorations accompanied by good oral hygiene may indicate that preserving natural teeth would benefit the patient.
- Occlusion and function
- Severe occlusal wear, collapsed vertical dimension, and parafunctional habits like bruxism may necessitate full-arch implant prostheses for predictable outcomes. However, these same factors might lead clinicians to recommend delayed implant loading rather than immediate loading protocols.
- Bone support and volume
- Severe ridge resorption or inadequate bone volume can challenge implant placement and may require grafting procedures. Some patients prefer to avoid the additional costs and extended healing time associated with grafting, making tilted implant approaches for full-arch prostheses an attractive alternative.14,15
Medical History Factors
- Systemic conditions affecting implant healing and success
- Uncontrolled diabetes (HbA1c > 8%) impairs healing and increases implant failure risk, while research indicates that well-controlled diabetes does not significantly affect implant outcomes.10,16
- Osteoporosis and medications to treat it, such as bisphosphonates and denosumab, increase osteonecrosis risk, requiring careful risk-benefit analysis before implant placement.17
- Autoimmune diseases (eg, rheumatoid arthritis, lupus, Sjögren syndrome) may compromise healing abilities. Xerostomia may affect both implants and natural teeth.18-20
- Cancer history, particularly head and neck radiation therapy, increases osteoradionecrosis risk and requires special consideration.
- Medications
- Immunosuppressants and corticosteroids may delay healing and increase infection risk, while anticoagulants can elevate bleeding risk during extractions and implant surgery.21,22
- Lifestyle
- Heavy smokers (> 10 cigarettes daily) face increased risks of implant failure and periodontal disease.23 For patients unable to reduce or quit smoking, treatment may favor preserving natural teeth or considering nonimplant prosthetic options.12
- Alcohol or drug use may indicate potential compliance and hygiene challenges.24-26
Financial and Psychological Factors
- Cost is a significant factor, as full-arch rehabilitation for either natural teeth or implants represents a substantial financial investment that may be prohibitive for some patients.
- Additionally, patient expectations and compliance largely determine treatment prognosis. For patients unwilling or unable to maintain proper oral hygiene, full-arch rehabilitation may not be the optimal solution.
Long-term Outcomes
Full-arch implant prostheses demonstrate impressive long-term survival rates ranging from 90% to 98% over 10 to 15 years, though complications increase over time.5,27-30 Biological complications include peri-implant mucositis (occurring in 30% to 50% of cases), peri-implantitis (10% to 20% of cases at 10 years), and marginal bone loss.31,32 Risk factors for these complications include poor oral hygiene, periodontal disease history, smoking, and diabetes.33
Prosthetic success varies, with most failures stemming from technical complications like screw loosening or fractures rather than implant failure.34-37 Patient satisfaction typically exceeds 90% due to improved function, esthetics, and phonetics, though common complaints include prosthesis bulkiness, food impaction, and speech difficulties, especially during the transition from natural dentition.38-40
Routine maintenance visits with a dentist becomes crucial in long-term maintenance of these protheses. Although the frequency of maintenance visits and follow-ups may depend on each clinician, it is recommended to have patients come for maintenance visits at a minimum of every 6 months to evaluate hygiene, occlusion, and any problems the patient may be experiencing.41 Removal of prostheses may be required if there is inability to clean or prosthetic complications emerge. Replacement of prosthetic screws may be necessary if wear of the screw is noted at maintenance visits. My maintenance protocol for full-arch prostheses is to have the patients return every 3 to 4 months for the first year and then re-evaluate the patient’s hygiene performance and health of the implants and prostheses. From there, it may warrant the patient to remain on the frequent maintenance protocol, or they may be placed on a biannual interval.
![]() Innovations in Materials and Technologies
Innovations in Materials and Technologies

Prosthetic materials for full-arch fixed implant prostheses have evolved significantly from acrylic and metal-acrylic options to include reinforced composites, polyether ether ketone, monolithic zirconia, and titanium bars with zirconia overlays. These advanced materials offer enhanced durability and esthetics. Zirconia particularly stands out for its superior strength, wear, and fracture resistance, and lifelike translucency when porcelain is added. Its highly polishable surface improves patient maintenance capabilities compared to acrylic alternatives. Both monolithic zirconia and titanium-zirconia hybrid designs reduce the required prosthetic space compared to traditional metal-acrylic prostheses.
Digital technology has revolutionized prosthetic and surgical planning for full-arch rehabilitation. Cone-beam computed tomography (CBCT) scans merged with intraoral scans create highly accurate three-dimensional models that allow clinicians to identify anatomical features to avoid, plan optimal implant placement based on prosthetic requirements, and anticipate potential grafting needs. These merged scans enable guided surgery planning using computer-aided design and manufacturing technology, helping predict and avoid surgical and prosthetic complications.
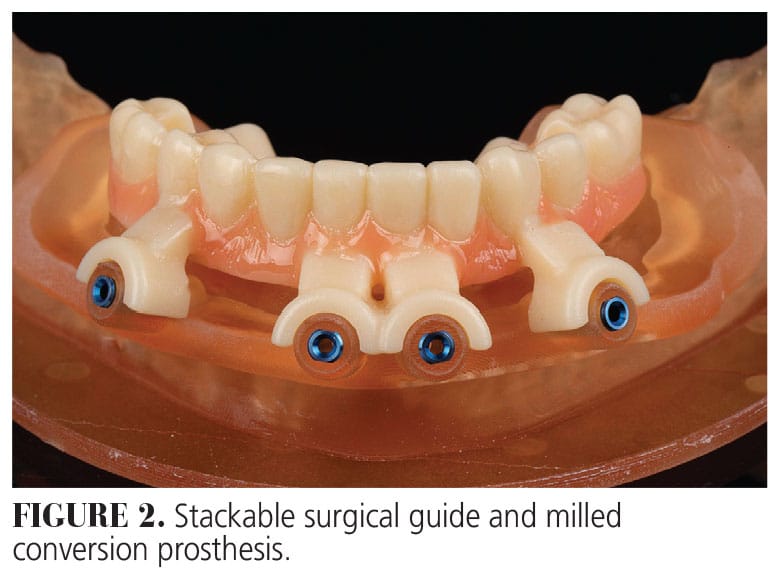
 Various technologies and techniques are available for full-arch rehabilitation, including trough guides from ideal denture set-ups (Figure 1), stackable guides with prefabricated conversion prostheses (Figure 2), photogrammetry, and scan gauges.42 Historical challenges in transitioning from the implant healing phase to final prosthesis have been addressed by newer digital methods that allow efficient progression in just a few appointments. These advanced approaches include photogrammetry, scan bodies with reverse scan techniques, and scan gauges, though they require intraoral scanners and specific digital systems. While initial costs and learning curves present barriers to adoption, these techniques become highly predictable once mastered.
Various technologies and techniques are available for full-arch rehabilitation, including trough guides from ideal denture set-ups (Figure 1), stackable guides with prefabricated conversion prostheses (Figure 2), photogrammetry, and scan gauges.42 Historical challenges in transitioning from the implant healing phase to final prosthesis have been addressed by newer digital methods that allow efficient progression in just a few appointments. These advanced approaches include photogrammetry, scan bodies with reverse scan techniques, and scan gauges, though they require intraoral scanners and specific digital systems. While initial costs and learning curves present barriers to adoption, these techniques become highly predictable once mastered.
Case Report
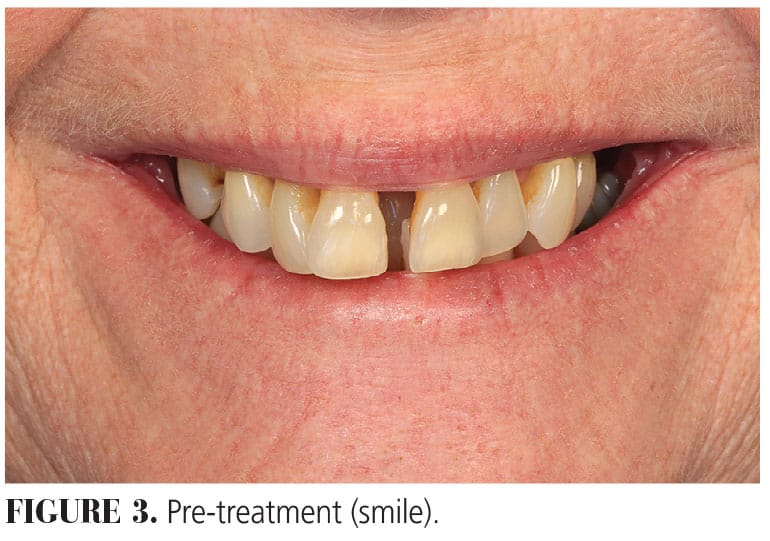
A 55-year-old woman presented with the chief complaint that “I want fixed implant options. I don’t want any removable options unless it’s a temporary. I already met with an oral surgeon” (Figures 3 and 4). No significant medical history was noted. Clinical exam revealed advanced periodontal disease with generalized Grade III mobility. Asymptomatic periapical lesion was present on #30. Supraeruption of the mandibular anterior teeth were noted. Her existing vertical dimension of occlusion was acceptable. She had a moderate smile line.
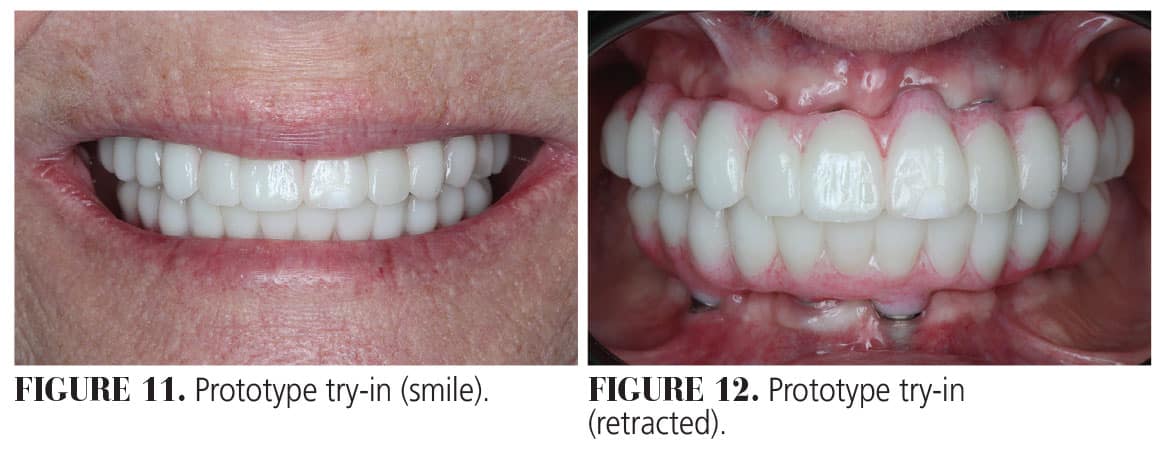
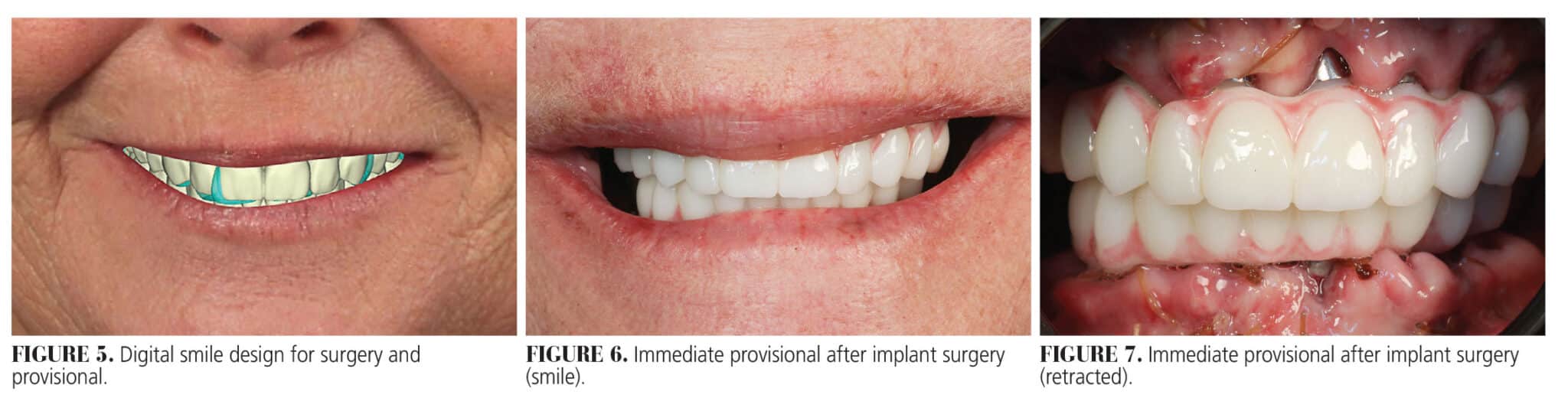
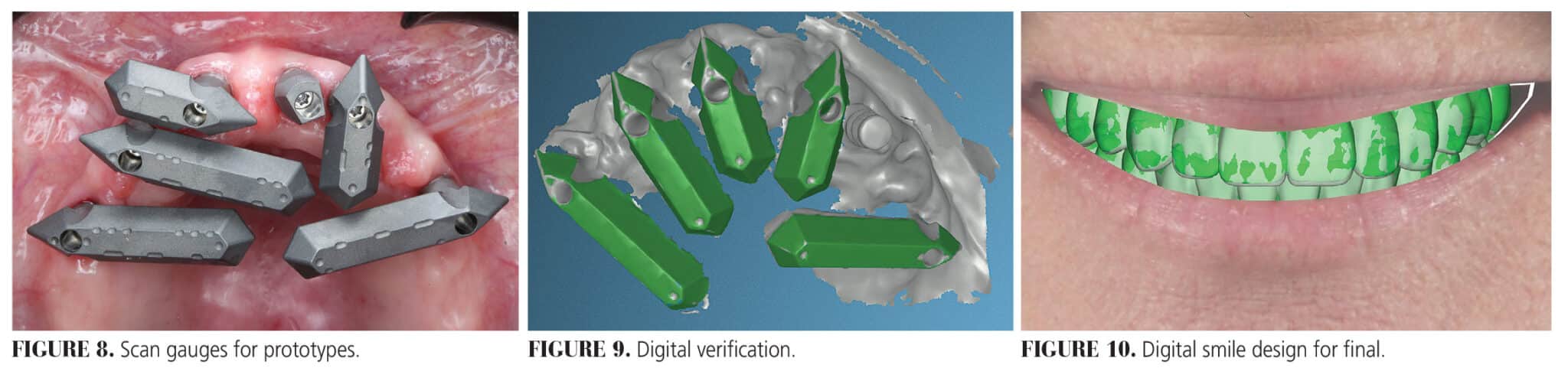
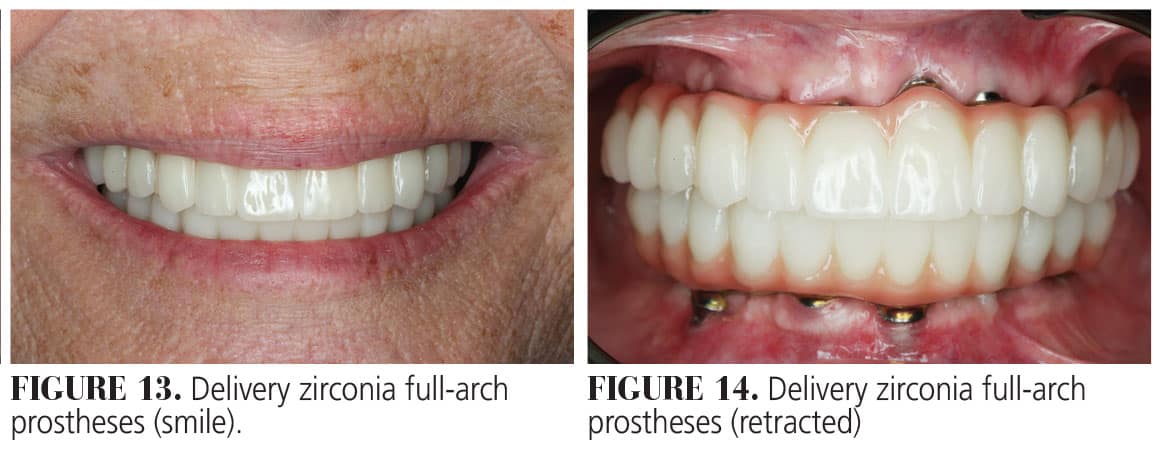
Treatment options of crown and bridge on implants and full-arch implant prostheses were discussed. The patient accepted proceeding with dual-arch full-arch implant prostheses. Utilizing a fully digital workflow, photographs were made and sent for digital smile design (Figure 5). Once the design was approved, a stereolithography file of the digital smile design was merged with an intraoral scan and CBCT imaging to plan for implant surgery. Six maxillary implants and four mandibular implants were placed by an oral and maxillofacial surgeon. Immediately following the surgery, appropriate multiunit abutments were placed and scan gauges were scanned. These scans were merged with the digital smile design to fabricate immediate provisional hybrid prostheses. Provisionals were printed using a ceramic-hybrid resin and placed the next day following immediate load protocol (Figures 6 and 7). After implant healing for 3 months, provisionals were removed, and scan gauges were placed and scanned to proceed with fabrication of prototypes and zirconia full-arch implant prostheses (Figure 8). Scans were verified chairside (Figure 9, page 13). Design changes were made to the provisionals (Figure 10) and prototypes were fabricated for try-in (Figures 11 and 12). After prototype approval, new scans of the prototypes were made and screw-retained maxillary and mandibular titanium bar with zirconia overlays were fabricated and inserted (Figures 13 and 14). Oral hygiene was reinforced and maintenance protocols established. An occlusal device was fabricated. She reported very high satisfaction with the treatment rendered.
Conclusion
Full-arch rehabilitation has evolved dramatically from osseointegration discovery to today’s digitally-driven workflows. Deciding between preserving natural teeth or proceeding with implant rehabilitation requires comprehensive assessment of dental history, medical factors, financial constraints, and patient expectations. Despite impressive long-term survival rates of 90% to 98% over 10 to 15 years, clinicians must remain vigilant about potential complications including peri-implant disease and technical failures. Advanced materials like zirconia have significantly improved durability and esthetics, while digital technologies have revolutionized treatment planning and execution through CBCT imaging, intraoral scanning, and guided surgery protocols. The integration of prosthetically-driven planning, immediate loading, and refined surgical techniques continues to elevate the standard of care in full-arch rehabilitation. Treatment decisions remain highly individualized, requiring careful consideration of functional outcomes, esthetic goals, and patient preferences. Ongoing innovation promises even greater precision and predictability, ultimately enhancing our ability to restore not just oral function, but also confidence and quality of life for our patients.
References
- Brånemark PI, Adell R, Breine U, Hansson BO, Lindström J, Ohlsson A. Intra-osseous anchorage of dental prostheses. I. experimental studies. Scand J Plast Reconstr Surg. 1969;3:81-100.
- The glossary of prosthodontic terms: ninth edition. 2017;117:e1-e105.
- Adell R, Eriksson B, Lekholm U, Brånemark PI, Jemt T. Long-term follow-up study of osseointegrated implants in the treatment of totally edentulous jaws. Int J Oral Maxillofac Implants.1990;5:347-359.
- Papaspyridakos P, Chen CJ, Chuang SK, Weber HP. Implant loading protocols for edentulous patients with fixed prostheses: a systematic review and meta-analysis. Int J Oral Maxillofac Implants. 2014;29(Suppl):256-270.
- Pjetursson BE, Thoma D, Jung R, Zwahlen M, Zembic A. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin Oral Implants Res. 2012;23(Suppl 6):22-38.
- Del Fabbro M, Ceresoli V. The fate of marginal bone around axial vs. tilted implants: a systematic review. Eur J Oral Implantol. 2014;7(Suppl 2):S171-189.
- Del Fabbro M, Pozzi A, Romeo D, de Araújo Nobre M, Agliardi E. Outcomes of fixed full-arch rehabilitations supported by tilted and axially placed implants: a systematic review and meta-analysis. Int J Oral Maxillofac Implants.2022;37:1003-1025.
- Seok WH, Yun PY, Chang NH, Kim YK. Tilted implants for implant-supported fixed hybrid prostheses: retrospective review. J Korean Assoc Oral Maxillofac Surg. 2023;49:278-286.
- Kim YK. Prosthesis-implant arch area ratio (PIAAR) – a new geometric paradigm, replacing the current ‘a-p spread’ of a cantilever in full-arch implant prosthesis: a proof-of-concept experiment. J Prosthodont. 2023;32:227-233.
- Marchand F, Raskin A, Dionnes-Hornes A, et al. Dental implants and diabetes: conditions for success. Diabetes Metab. 2012;38:14-19.
- Tonetti MS, Chapple IL, Jepsen S, Sanz M. Primary and secondary prevention of periodontal and peri-implant diseases: Introduction to, and objectives of the 11th European Workshop on Periodontology consensus conference. J Clin Periodontol. 2015;42 Suppl 16:S1-4.
- Porter JA, von Fraunhofer JA. Success or failure of dental implants? A literature review with treatment considerations. Gen Dent. 2005;53:423-432.
- Chrcanovic BR, Albrektsson T, Wennerberg A. Periodontally compromised vs. periodontally healthy patients and dental implants: a systematic review and meta-analysis. J Dent. 2014;42:1509-1527.
- Esposito M, Grusovin MG, Felice P, Karatzopoulos G, Worthington HV, Coulthard P. The efficacy of horizontal and vertical bone augmentation procedures for dental implants — a Cochrane systematic review. Eur J Oral Implantol. 2009;2:167-184.
- Esposito M, Grusovin MG, Polyzos IP, Felice P, Worthington HV. Timing of implant placement after tooth extraction: immediate, immediate-delayed or delayed implants? A Cochrane systematic review. Eur J Oral Implantol. 2010;3:189-205.
- Chrcanovic BR, Albrektsson T, Wennerberg A. Diabetes and oral implant failure: a systematic review. J Dent Res. 2014;93:859-867.
- Otto S, Pautke C, Van den Wyngaert T, Niepel D, Schiødt M. Medication-related osteonecrosis of the jaw: Prevention, diagnosis and management in patients with cancer and bone metastases. Cancer Treat Rev. 2018;69:177-187.
- Duttenhoefer F, Fuessinger MA, Beckmann Y, Schmelzeisen R, Groetz KA, Boeker M. Dental implants in immunocompromised patients: a systematic review and meta-analysis. Int J Implant Dent. 2019;5:43.
- Zheng F, Annamma LM, Harikrishnan SS, Lee DJ. Systemic factors affecting prognosis in restorative and prosthetic dentistry: a review. Dent Clin North Am. 2024;68:751-765.
- Ergun S, Katz J, Cifter ED, Koray M, Esen BA, Tanyeri H. Implant-supported oral rehabilitation of a patient with systemic lupus erythematosus: case report and review of the literature. Quintessence Int. 2010;41:863-867.
- Plemons JM, Al-Hashimi I, Marek CL. Managing xerostomia and salivary gland hypofunction: executive summary of a report from the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2014;145:867-73.
- Brennan MT, Wynn RL, Miller CS. Aspirin and bleeding in dentistry: an update and recommendations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:316-323.
- Bain CA, Moy PK. The association between the failure of dental implants and cigarette smoking. Int J Oral Maxillofac Implants. 1993;8:609-615.
- Rossow I. Illicit drug use and oral health. Addiction. 2021;116:3235-3242.
- Teoh L, Moses G, McCullough MJ. Oral manifestations of illicit drug use. Aust Dent J. 2019;64:213-222.
- Baghaie H, Kisely S, Forbes M, Sawyer E, Siskind DJ. A systematic review and meta-analysis of the association between poor oral health and substance abuse. Addiction. 2017;112:765-779.
- Gallucci GO, Benic GI, Eckert SE, et al. Consensus statements and clinical recommendations for implant loading protocols. Int J Oral Maxillofac Implants. 2014;29 Suppl:287-290.
- Malo P, de Araújo Nobre M, Lopes A, Moss SM, Molina GJ. A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up. J Am Dent Assoc. 2011;142:310-320.
- Maló P, de Araújo Nobre M, Lopes A, Ferro A, Botto J. The All-on-4 treatment concept for the rehabilitation of the completely edentulous mandible: A longitudinal study with 10 to 18 years of follow-up. Clin Implant Dent Relat Res. 2019;21:565-577.
- La Monaca G, Pranno N, Annibali S, Di Carlo S, Pompa G, Cristalli MP. Immediate flapless full-arch rehabilitation of edentulous jaws on 4 or 6 implants according to the prosthetic-driven planning and guided implant surgery: A retrospective study on clinical and radiographic outcomes up to 10 years of follow-up. Clin Implant Dent Relat Res. 2022;2):831-844.
- Atieh MA, Alsabeeha NH, Faggion CM, Jr., Duncan WJ. The frequency of peri-implant diseases: a systematic review and meta-analysis. J Periodontol. 2013;84:1586-1598.
- Derks J, Schaller D, Håkansson J, Wennström JL, Tomasi C, Berglundh T. Peri-implantitis – onset and pattern of progression. J Clin Periodontol. 2016;43:383-388.
- Renvert S, Polyzois I. Risk indicators for peri-implant mucositis: a systematic literature review. J Clin Periodontol. 2015;42 Suppl 16:S172-186.
- Gonzalez-Gonzalez I, deLlanos-Lanchares H, Brizuela-Velasco A, et al. Complications of fixed full-arch implant-supported metal-ceramic prostheses. Int J Environ Res Public Health. 2020;17:4250.
- Altarawneh S, Limmer B, Reside GJ, Cooper L. Dual jaw treatment of edentulism using implant-supported monolithic zirconia fixed prostheses. J Esthet Restor Dent. 2015;27:63-70.
- Papaspyridakos P, Chen CJ, Chuang SK, Weber HP, Gallucci GO. A systematic review of biologic and technical complications with fixed implant rehabilitations for edentulous patients. Int J Oral Maxillofac Implants. 2012;27:102-110.
- Papaspyridakos P, Bordin TB, Kim YJ, et al. Technical complications and prosthesis survival rates with implant-supported fixed complete dental prostheses: a retrospective study with 1- to 12-year follow-up. J Prosthodont. 2020;29:3-11.
- Gonçalves GSY, de Magalhães KMF, Rocha EP, Dos Santos PH, Assunção WG. Oral health-related quality of life and satisfaction in edentulous patients rehabilitated with implant-supported full dentures all-on-four concept: a systematic review. Clin Oral Investig. 2022;26:83-94.
- Oh SH, Kim Y, Park JY, Jung YJ, Kim SK, Park SY. Comparison of fixed implant-supported prostheses, removable implant-supported prostheses, and complete dentures: patient satisfaction and oral health-related quality of life. Clin Oral Implants Res. 2016;27:e31-7.
- MA EL, Elgamal M, Mohammed Askar O, Youssef Al-Tonbary G. Patient satisfaction and oral health-related quality of life (OHRQoL) of conventional denture, fixed prosthesis and milled bar overdenture for All-on-4 implant rehabilitation. A crossover study. Clin Oral Implants Res. 2019;30:1107-1117.
- Lanzetti J, Crupi A, Gibello U, et al. How often should implant-supported full-arch dental prostheses be removed for supportive peri-implant care to maintain peri-implant health? A systematic review. Int J Oral Implantol. 2024;17:45-57.
- Cappare P, Sannino G, Minoli M, Montemezzi P, Ferrini F. Conventional versus digital impressions for full arch screw-retained maxillary rehabilitations: a randomized clinical trial. Int J Environ Res Public Health. 2019;16:829.
From Decisions in Dentistry. May/June 2025;11(3):10-15.
