

Unlocking the Regenerative Power of Platelet-Rich Fibrin
This platelet concentrate is transforming dental wound healing and tissue regeneration with its autologous growth factors and simplified application.
PURCHASE COURSE
This course was published in the March/April 2025 issue and expires April 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the March/April 2025 issue and expires April 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 310
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the biological properties of platelet-rich fibrin (PRF) and its role in promoting wound healing, tissue regeneration, and bone formation in dental procedures.
- Identify the clinical applications of PRF in dentistry.
- Discuss the advantages of PRF over traditional platelet concentrates like PRP and PRGF.
In recent years, regenerative medicine has made a remarkable impact, showing its potential across different fields, including dentistry. Platelet-rich fibrin (PRF), a platelet concentrate derived from the patient’s own blood, has gained significant attention for its wound healing and tissue regeneration properties. This article explores the benefits, applications, and evolving role of PRF in modern dentistry.
PRF is an autologous concentration of platelets in a fibrin matrix.1 The process entails a simplified method in which a patient’s blood is centrifuged at specific speeds, leading to the formation of PRF clot which is rich in natural platelets, growth factors, and leukocytes. Unlike platelet-rich plasma (PRP), PRF does not require biochemical handling and is therefore simple to prepare and apply.
The initial concept behind creating platelet concentrates was to collect concentrated platelets and natural growth factors in plasma solutions, which could then be applied to surgical sites to enhance local healing.2 This technique, introduced in the late 1990s, became known as PRP.3 PRP consists mostly of platelets that release growth factors to actively start the wound healing process and enhance cell adhesion, proliferation, and migration.4 Around the same time, another platelet concentrate was introduced that used anticoagulants called platelet-rich growth factor (PRGF).5
However, there are several limitations to using PRP and PRGF. Their preparation requires additional coagulation factors such as bovine thrombin or CaCl2. The process also involves two separate centrifugation stages to concentrate platelets without including leukocytes, which sometimes can take up to an hour. The resulting liquid nature of PRP complicates handling, limiting its applications, as it needs to be used with other biomaterials to improve handling. Additionally, PRP has a very short growth factor release profile, hindering its potential for bone regeneration.6 These challenges have led to the creation of a second-generation platelet concentrate, PRF, which is made entirely from autologous sources.7
Biological Rationale
PRF’s underlying strength lies in its naturally formed concentration mixture of growth factors including platelet-derived growth factor (PDGF), transforming growth factor beta (TGF-b), vascular endothelial growth factor (VEGF), and various cytokines.8 These growth factors play a pivotal role in tissue healing and regeneration by stimulation normal cell proliferation, migration, and differentiation.
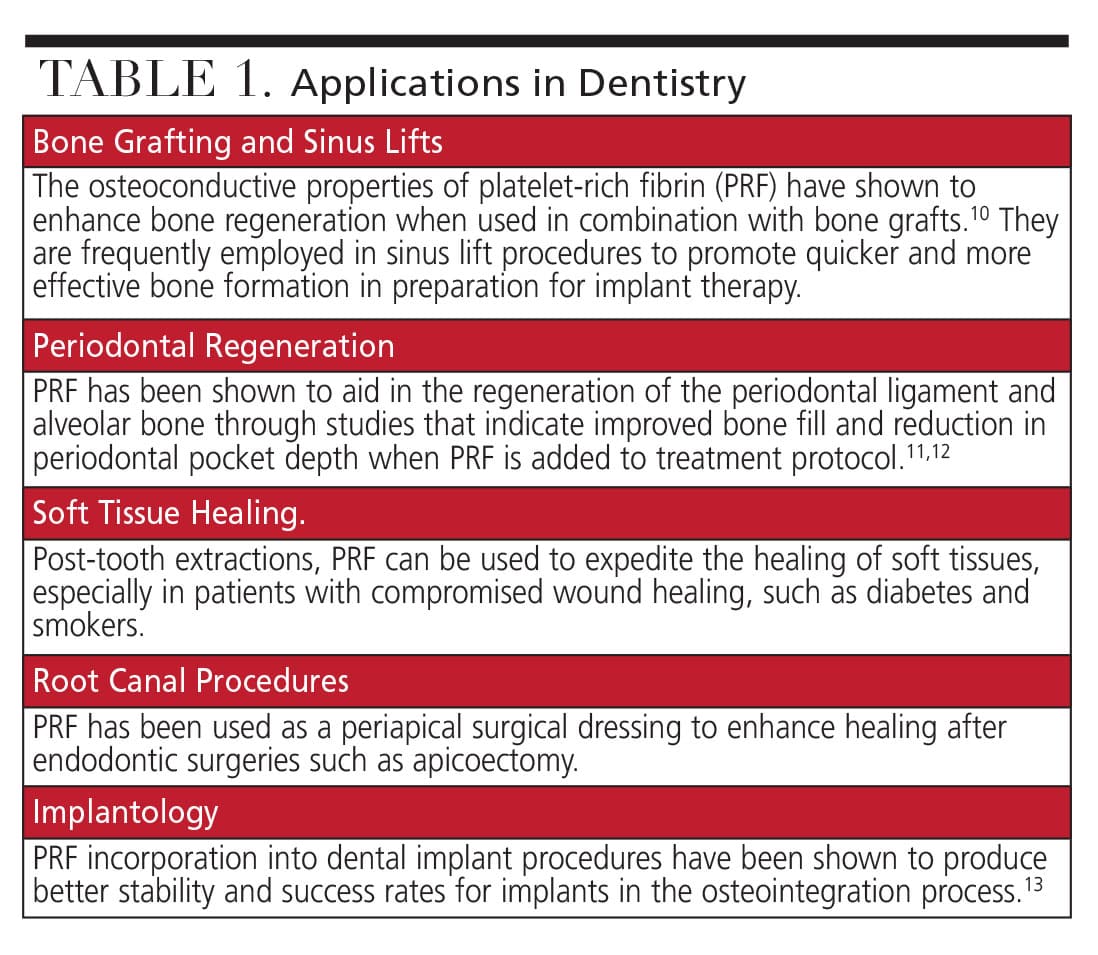
Physiologically, after an injury is made, wound healing occurs in four overlapping phases: initial hemostasis, the inflammatory phase, the proliferative phase, and the remodeling phase. Platelets manage hemostasis by blocking blood vessels and promoting fibrin clot formation. During the inflammatory phase, white blood cells and platelets release cellular products that start the healing process. Applying PRF to a wound site enhances healing due to the concentrated growth factors in PRF, which facilitate cell migration, proliferation, and differentiation.9 Table 1 shows the applications in dentistry.10-13
Sinus Lift Procedures
The versatility of PRF to promote bone healing with regards to sinus augmentation has been documented in recent years both as a sole material but also in combination with other biomaterials. Traditionally, sinus lift procedures, as described by Boyne and James in 1980, involved access to the sinus via a lateral window.14 The use of graft materials, including autogenous bone, allografts, xenografts, and combinations of the various materials, have been well studied as part of the traditional sinus lift.15
The use of PRF in a sinus lift procedure represents a different modality to maxillary sinus grafting. When used in combination with grafting material or independently, PRF can provide a reservoir for growth factors to act directly on osteoblasts, fibroblasts, and endothelial cells.16 This interaction can lead to tissue regeneration, potential to recruit circulating stems cells, and the ability to promote wound closure using epithelial tissues.
A recent systematic review found that nine out of 13 controlled studies reported positive results for PRF in soft tissue regeneration and wound healing. Histomorphometry assessments have shown that new bone formation with the combination of PRF and biomaterials ranges from 17% to 45%, compared to 13% to 33% with biomaterials alone.17 Meta-analysis indicated a 1.98% increase in new bone formation with the addition of PRF to biomaterials, though these findings were not statistically significant and exhibited moderate heterogeneity across studies. Regarding residual biomaterial, pooled analysis demonstrated a statistically significant reduction of 4.60% when PRF was used.
Dental Extraction Procedures
PRF significantly accelerates both soft and hard tissue healing. The high concentration of platelets and growth factors stimulates cell proliferation, differentiation, and extracellular matrix formation essential for wound healing. Studies indicate that PRF enhances tissue regeneration and accelerates the healing process, leading to quicker recovery times and improved patient comfort.18 One of the primary benefits of PRF in dental extractions is its ability to reduce post-operative pain, swelling, and the risk of complications such as dry sockets. By forming a protective barrier over the wound, PRF maintains the integrity of the blood clot, which is critical for proper healing, and protects the extraction site from bacterial invasion and external irritants.19 PRF is particularly beneficial in cases requiring bone regeneration, such as in patients undergoing bone grafting procedures.
The growth factors in PRF enhance the production of new bone cells, accelerating bone regeneration and ensuring proper healing of the extraction site. This is crucial for maintaining the structural integrity and functionality of the jawbone, especially in preparation for dental implants. PRF also aids in graft stabilization, providing a scaffold for new bone growth and improving the outcomes of grafting procedures.18
Periodontal Defects
PRF has been particularly effective in the treatment of periodontal intrabony defects. When applied to these defects, PRF enhances bone regeneration and supports the healing of the periodontal ligament and cementum. Meta-analyses demonstrate that using PRF alone or in combination with other regenerative materials significantly improves clinical outcomes compared to traditional treatments.20
PRF significantly enhances periodontal tissue regeneration by releasing key growth factors such as PDGF and TGF-β. These growth factors stimulate the proliferation and differentiation of cells essential for tissue repair, including fibroblasts and osteoblasts. A 2023 systematic review and network meta-analysis found that the use of PRF in periodontal intrabony defects significantly improves clinical parameters such as probing depth, clinical attachment level, and bone fill compared to other treatments.21
Additionally, a recently randomized controlled trial highlighted that the adjunctive use of collagen membrane with PRF in the treatment of periodontal intrabony defects resulted in significantly better clinical outcomes than PRF alone.22 These studies have supported the evidence that PRF enhances bone regeneration and supports the healing of the periodontal ligament and cementum. This is crucial in ensuring the long-term stability and functionality of the periodontium. Therefore, when possible, the use of PRF in periodontal intrabony defects may result in significant improvements in clinical outcomes compared to traditional methods.
Endodontic Therapy
PRF has been effectively used in conjunction with other materials for root canal treatments, leading to improved clinical outcomes. For example, PRF combined with calcium hydroxide has shown enhanced results in promoting periapical healing. Additionally, PRF can be used as a scaffold for regenerative endodontic procedures, supporting the regeneration of pulp-dentin complex in immature teeth with necrotic pulps.23
Traditional methods, like apexification, have aimed to stimulate the formation of a calcific barrier at the root apex. However, newer techniques involving biological materials such as PRF and demineralized bone matrix (DMBM) are emerging as promising alternatives. In a case report on an 18-year-old man who presented with a fractured upper central incisor with an open apex from previous trauma, apexification was performed using DMBM and PRF along with mineral trioxide aggregate (MTA) as an apical barrier. After removal of necrotic pulp tissue, irrigating with sodium hypochlorite, and placing a calcium hydroxide medicament, a mixture of DMBM and PRF was placed into the canal to form an apical barrier, followed by MTA placement and final restoration. During the subsequent follow up visits, radiographic evidence indicated bone healing and complete apical closure after 3 months.24
In surgical endodontic procedures, such as apicoectomy, the application of PRF has enhanced healing of the surgical site. PRF serves as a matrix that supports new tissue growth and helps seal the surgical site, which reduces the risk of post-surgical complications and improves overall healing outcomes. In a recent case report, PRF was used in conjunction with an apicoectomy for treatment of a radicular cyst, resulting in an accelerated healing rate.25
Implant Dentistry
One of the primary benefits of PRF in implant dentistry is its ability to enhance osseointegration.26 PRF provides a scaffold for new bone growth and delivers essential growth factors that stimulate osteoblast activity. Studies have demonstrated that the application of PRF around dental implants can significantly increase bone-to-implant contact, thereby improving the stability and integration of the implant into the surrounding bone.
PRF has also been shown to accelerate soft tissue healing around dental implants. The fibrin matrix in PRF acts as a scaffold for cell migration and proliferation, promoting the formation of new blood vessels and connective tissue. This results in faster wound healing and improved gingival health, which is crucial for the long-term success of dental implants.27
Advantages of Platelet-Rich Fibrin
PRF offers a wide array of benefits in the practice of dentistry, including but not limited to:
- PRF’s natural biological structure includes PDGF, TGF-b, and VEGF which accelerate wound healing, support the formation of new blood vessels (angiogenesis), and stimulate the proliferation of osteoblasts and fibroblasts.28
- The fibrin matrix of PRF enhances tissue regeneration by providing a natural scaffold that supports cell migration and proliferation.28
- Recent studies have shown that PRF has inherent antimicrobial properties that reduce post-operative infections.29
- The use of PRF is a minimally invasive procedure utilizing the patient’s blood, thus eliminating the risk of allergic reactions and disease transmission.19
- The preparation of PRF is straight forward with appropriate training, minimal cost to both the practitioner and patient, and versatile in its dental applications.
- As an alternative to using costly biomaterial for regeneration, PRF utilizes a patient’s own autologous nature.
Conclusion
In summary, this review highlights the extensive application of PRF in various dental clinical settings. Despite being relatively unfamiliar to many clinicians, the accumulated evidence over the years supports PRF’s effectiveness in enhancing tissue regeneration. PRF is a valuable addition to the dental regenerative toolbox. PRF combined with regenerative therapy has shown significant promise for periodontal repair of intrabony and furcation defects, as well as soft tissue root coverage for gingival recessions.
Additionally, literature suggests that PRF can reduce infection post-tooth extraction and potentially minimize dimensional changes following tooth loss. The versatility of PRF in clinical applications is evident in its use for various bone grafting procedures, including socket preservation, ridge augmentation, and sinus lifts. Studies have shown that PRF not only enhances the integration of graft materials but also stabilizes them, ensuring better retention and effectiveness. However, more research is needed to determine its efficacy in bone defect regeneration, including guided bone regenerative procedures and sinus elevation. Despite this, its ease of use, low cost, and autologous nature make it a valuable biomaterial for further exploration in dental surgery.
References
- Coury AJ. Expediting the transition from replacement medicine to tissue engineering. Regen Biomater. 2016;3:111-113.
- Anfossi G, Trovati M, Mularoni E, Massucco P, Calcamuggi G, Emanuelli G. Influence of propranolol on platelet aggregation and thromboxane B2 production from plateletrich plasma and whole blood. Prostaglandins Leukot Essent Fatty Acids. 1989;36:1-7.
- Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85:638-646.
- Marx RE. Platelet-rich plasma: evidence to support its use. J Oral Maxillofac Surg. 2004;62:489-496.
- Anitua E, Prado R, Troya M, et al. Implementation of a more physiological plasma rich in growth factor (PRGF) protocol: Anticoagulant removal and reduction in activator concentration. Platelets. 2016;27:459-466.
- Kobayashi E, Flückiger L, Fujioka-Kobayashi M, et al. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin Oral Investig. 2016;20:2353-2360.
- Saluja H, Dehane V, Mahindra U. Platelet-rich fibrin: A second generation platelet concentrate and a new friend of oral and maxillofacial surgeons. Ann Maxillofac Surg. 2011;1:53-57.
- Dohan DM, Choukroun J, Diss A, et al. Platelet-rich fibrin (PRF): a secondgeneration platelet concentrate. Part I: technological concepts and evolution. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:e37-e44.
- Fan Y, Perez K, Dym H. Clinical uses of platelet-rich fibrin in oral and maxillofacial surgery. Dent Clin North Am. 2020;64:291-303.
- Del Fabbro M, Karanxha L, Panda S, et al. Autologous platelet concentrates for treating periodontal infrabony defects. Cochrane Database Syst Rev. 2018;11:CD011423.
- Shah R, Triveni MG, Thomas R, Mehta DS. An update on the protocols and biologic actions of platelet rich fibrin in dentistry. Eur J Prosthodont Restor Dent. 2017;25:64-72.
- Jagtap A, Mangalekar SB, Kamble P. Clinical evaluation of coronally advanced flap with or without advance-platelet rich fibrin membrane in the treatment of miller’s class-ii localized gingival recession: a clinical study. Cureus. 2023;15:e34919.
- Alhussaini AHA. Effect of platelet-rich fibrin and bone morphogenetic protein on dental implant stability. J Craniofac Surg. 2019;30:1492-1496.
- Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg. 1980;38:613-616.
- Al-Moraissi EA, Alkhutari AS, Abotaleb B, Altairi NH, Del Fabbro M. Do osteoconductive bone substitutes result in similar bone regeneration for maxillary sinus augmentation when compared to osteogenic and osteoinductive bone grafts? A systematic review and frequentist network meta-analysis. Int J Oral Maxillofac Surg. 2020;49:107-120.
- Miron RJ, Zucchelli G, Pikos MA, et al. Use of platelet-rich fibrin in regenerative dentistry: a systematic review. Clin Oral Investig. 2017;21:1913-1927.
- Ortega-Mejia H, Estrugo-Devesa A, Saka-Herrán C, Ayuso-Montero R, López-López J, Velasco-Ortega E. Platelet-rich plasma in maxillary sinus augmentation: systematic review. Materials (Basel). 2020;13:622.
- Lahham C, Ta’a MA, Lahham E, Michael S, Zarif W. The effect of recurrent application of concentrated platelet-rich fibrin inside the extraction socket on the hard and soft tissues. a randomized controlled trial. BMC Oral Health. 2023;23:677.
- Berton F, Costantinides F, Stacchi C, Corradini A, Di Lenarda A, Di Lenarda R. Is LPRF an effective hemostatic agent in single tooth extractions? A cohort study on VKA and DOAC patients. Clin Oral Investig. 2023;27:2865-2874.
- Silva FFVE, Chauca-Bajaña L, Caponio VCA, et al. Regeneration of periodontal intrabony defects using platelet-rich fibrin (PRF): a systematic review and network meta-analysis. Odontology. 2024;112:1047-1068.
- Miron RJ, Moraschini V, Fujioka-Kobayashi M, et al. Use of platelet-rich fibrin for the treatment of periodontal intrabony defects: a systematic review and meta-analysis. Clin Oral Investig. 2021;25:2461-2478.
- Mubarak R, Adel-Khattab D, Abdel-Ghaffar KA, Gamal AY. Adjunctive effect of collagen membrane coverage to L-PRF in the treatment of periodontal intrabony defects: a randomized controlled clinical trial with biochemical assessment. BMC Oral Health. 2023;23:631.
- Kaur G, Thomas AR, Samson RS, et al. Efficacy of electronic apex locators in comparison with intraoral radiographs in working length determination- a systematic review and meta-analysis. BMC Oral Health. 2024;24:532.
- Sinha Y, Tilokani A, Pradhan PK, Majee N, Wandile B. Advanced management of open apex utilizing platelet-rich fibrin and bone graft as apical barriers with mineral trioxide aggregate (mta) obturation: a detailed case report. Cureus. 2024;16:e60883.
- Tewari S, Dhiman M, Bhagavatheeswaran S, Thakur V, Tewari S. Management of isolated labial mucosal fenestration by endodontic microsurgery along with platelet-rich fibrin and connective tissue graft: a series of four cases. Clin Adv Periodontics. 2022;12:194-203.
- Ivanovski S, Lee RSB, Fernandez-Medina T, Pinto N, Andrade C, Quirynen M. Impact of autologous platelet concentrates on the osseointegration of dental implants. Periodontol 2000. 2025;97:271-286.
- Strauss FJ, Stähli A, Gruber R. The use of platelet-rich fibrin to enhance the outcomes of implant therapy: A systematic review. Clin Oral Implants Res. 2018;29 Suppl 18:6-19.
- Strauss FJ, Nasirzade J, Kargarpoor Z, Stähli A, Gruber R. Effect of platelet-rich fibrin on cell proliferation, migration, differentiation, inflammation, and osteoclastogenesis: a systematic review of in vitro studies. Clin Oral Investig. 2020;24:569-584.
- Moraschini V, Miron RJ, Mourão CFAB, et al. Antimicrobial effect of platelet-rich fibrin: A systematic review of in vitro evidence-based studies. Periodontol 2000. 2024;94:131-142.
From Decisions in Dentistry. March/April 2025;11(2):40-45.

