

Avoiding and Managing Implant Complications
Careful planning and placement, followed by proper maintenance, can help providers and patients avoid implant complications.
PURCHASE COURSE
This course was published in the August 2019 issue and expires August 2022. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the August 2019 issue and expires August 2022. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Explain the role of meticulous treatment planning and thorough assessment of patients and potential surgical sites when performing dental implant therapy.
- Discuss risk factors for implant complications, as well as strategies that can help providers and patients avoid or manage complications.
- Describe how periodontal disease can increase the risk of peri-implantitis and potentially compromise the long-term success of implant treatment.
Dental implants cannot be placed, restored and forgotten. They require maintenance and daily oral hygiene measures similar to that of the teeth they replace.1 Some consumer-facing advertising has distorted the reality of implant dentistry, however, leading many to believe implants are a panacea for oral health issues that can be delivered in one or two appointments. Unfortunately, implant complications can lead to peri-implantitis and eventual failure.
In implant therapy, meticulous planning, careful placement, and ongoing maintenance can help providers and patients achieve successful long-term outcomes. Because patient compliance with maintenance appointments and self-care is crucial to implant success, it is important for patients to understand that systemic and/or environmental conditions may predispose them to treatment complications from the start.
Often, while the execution of implant placement and restoration may take place over relatively few visits, true long-term implant success requires careful and thorough planning and an assessment of both the patient and potential implant site. Site- and patient-specific factors influence implant success and should be managed proactively as part of a multidisciplinary team. Providing patients with a comprehensive road map of their treatment, including the long-term maintenance of the final restorations, will result in lasting esthetic and functional outcomes with minimal implant complications.
SITE-RELATED RISK FACTORS
Tooth loss can significantly contribute to hard and soft tissue deficiencies prior to implant placement,2 but the cause of tooth loss can affect the future prognosis of the implant. If teeth were lost secondary to periodontitis, implants placed in that patient are at a higher risk of developing peri-implantitis. The exact onset and progression of peri-implantitis are not quite understood. Experimental studies found that once the implant’s mucosal seal is damaged, biofilm formation can result in severe inflammation and tissue destruction. Peri-implantitis lesions are dominated in proportion, number and density by neutrophils, plasma cells and other immune cells. Their inflammatory fronts are twice as large as those seen in periodontitis, with similar species of red complex bacteria, yet greater and more accelerated patterns of bone loss.3
The 2017 World Workshop on the Classification of Periodontal and Peri-implant Diseases and Conditions, jointly presented by the American Academy of Periodontology and the European Federation of Periodontology, recognized a history of periodontitis as a strong risk factor for future peri-implant disease.3 While the 10-year implant survival rate for patients with treated periodontitis exceeded 90%, the rate of implant complications requiring antibiotic or surgical intervention increased with severity of disease.1 Therefore, a patient who has experienced periodontitis should always be managed as such, and — even with treatment — should not return to a maintenance and evaluation schedule similar to that of healthy patients.
Patients with residual pocketing are also at increased risk for compromised peri-implant conditions, including increased peri-implant probing depths (≥ 5mm), bone loss and bleeding on probing.4 While patients prioritize timely implant placement, they should understand that ≥ 6 mm of periodontal pocketing can lead to implant complications. Periodontal treatment should be completed prior to, or at time of, implant placement in these cases. Patients with advanced periodontal destruction seeking full-mouth extractions for implant-assisted rehabilitation are particularly worrisome. These individuals may believe that extractions “cure them” of disease, but a periodontitis patient is a “periodontitis patient for life.” Thorough periodontal and restorative assessments, including overall diagnoses and tooth-specific prognoses, are critical.
Many patients treated and strictly maintained with what was formerly known as generalized aggressive periodontitis were able to retain teeth for five to 19 years, with an annual tooth loss rate of 0.09 to 0.27 in specialty and general practices, respectively.5,6 However, when implants were placed in patients with a history of treated periodontitis, there was a fivefold increased risk of implant failure and 14-fold risk of peri-implantitis compared to non-periodontitis patients.7
A seemingly hopeless dentition therefore requires a strong multidisciplinary workup to avoid catastrophic biologic and prosthetic failures. Forming a global prognosis that includes tooth-, arch- and patient-related factors also aids in the prosthetic retreatment of implant failures. When a true reconstructive approach is followed, the original implant systems, locations and angulations can accommodate changes to the implant-borne prosthesis, even in patients with significant bone and attachment loss. Removable prostheses supported and stabilized by any remaining implants or teeth can restore esthetics and function in the most compromised of circumstances.8
Similar to periodontitis, the presence of plaque serves as the strongest indicator for peri-implant disease.3 Proper self-care and routine professional maintenance are essential throughout healing and after delivery of the final restoration(s). Studies have shown a progression of implant disease without supportive therapy and proper oral hygiene.9,10 Use of an extra-soft toothbrush or end-tufted brush to debride the adjacent teeth and/or healing abutment can help minimize plaque formation during healing. It will also instill oral hygiene practices early on.

Other factors contribute to implant complications, and the surgical and restorative teams should take steps during treatment planning and delivery to avoid or minimize problems. For example, residual cement on cemented implant restorations may be associated with peri-implant mucositis and peri-implantitis.3 Greater excess cement was noted with earlier crown delivery (i.e., fewer than four weeks of soft tissue healing) and deeper, subgingival margins.11,12 Korsch et al13 found that permanent cement promoted bacterial dysbiosis, and upon its removal, improved peri-implant tissue health was noted. With these variables in mind, proper three-dimensional (3D) implant placement can reduce the need for compromised margins and cementation.
PATIENT-RELATED RISK FACTORS
In addition to these local risk factors, patients’ overall health affects treatment response. While implants can improve the quality of life for medically compromised patients, appropriate management of their systemic diseases can ensure safe implant placement and better long-term outcomes. A thorough review of medical history and medical consultations are critical to adequately assessing and stratifying risk for patients planning to replace teeth with dental implants.
Stable glycemic control is an increasingly important concept in patients with diabetes. Compared to normoglycemic individuals, patients with dental implants are at 3.4 times greater risk of peri-implantitis if they demonstrate hyperglycemia and elevated HbA1c levels.14 Bone-related disorders, such as osteoporosis and osteopenia, have shown no significant difference in survival rates (95% to 96%) or clinical and radiographic parameters compared to healthy controls.15 Additionally, certain medications — such as selective serotonin reuptake inhibitors and proton pump inhibitors — are associated with increased implant failure rates.16
Cigarette smoking can be devastating to the implant apparatus. The incidence of peri-implantitis is almost double (37%) that of nonsmokers.17 There is a dose-dependent, 3.1- to 4.7-fold increased risk of peri-implant disease in smokers.18 While smoking cessation may reduce the risk of periodontitis over time,19 there is less evidence regarding the impact of smoking cessation on peri-implantitis and implant failure. In patients who smoke, the initial design of implant-assisted rehabilitations should also be adaptable to the loss of one or multiple implants to minimize total prosthetic failure, especially in patients unable or unwilling to quit smoking.
ESTHETIC-RELATED RISK FACTORS
Esthetic risk factors also drive treatment and patient interests. A malpositioned implant, thin tissue phenotype, deficient facial plate and/or significant bony defect can increase the risk and frequency of mucosal recession.20,21 This is especially concerning for replacement of maxillary incisors, canines or first premolars, which make up the esthetic zone. Trying to minimize recession through control of these risk factors intraoperatively can lead to improved esthetic outcomes and patient satisfaction. Immediate implant placement takes advantage of native ridge dimensions, reduces treatment time and number of appointments, and has demonstrated survival rates similar to delayed implant protocols.22 The buccal plate in the anterior maxilla is usually less than 1 mm thick, though 2 mm is favored for long-term maintenance of ridge thickness.23 Therefore, grafting the implant-socket gap and along the external aspect of the buccal plate can increase buccal ridge width by 2 mm at time of implant uncovery for immediate implants, which also provides soft tissue stability.24,25 Thin phenotypes have been significantly associated with marginal bone loss in a short-term follow-up of platform-switched implants.26 Phenotype modification from thin to thick via connective tissue grafting maintained bone levels, the facial mucosal margin, and interproximal papillae for two years after surgery.27
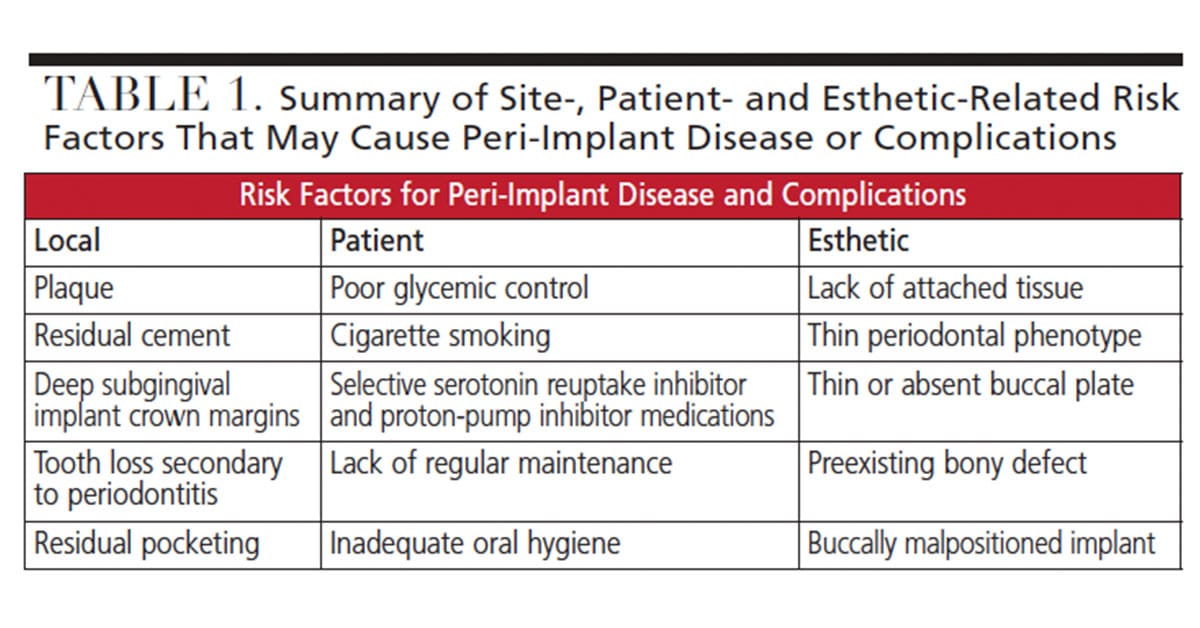
Advising patients prior to implant placement of the possible need for additional bone grafting at time of implant placement, or for future soft tissue grafting, outlines the difficulties that may be encountered throughout treatment and provides realistic patient expectations. In some cases, even with the use of 3D imaging, these decisions can only be made at the time of surgery. As grafting procedures require further time and expense, their need — even if considered unlikely — should be discussed with the patient in the initial treatment plan. Taken together, the site-, patient- and esthetic-related risk factors are summarized in Table 1.
ROLE OF INFORMED CONSENT
Care should be taken by dental practitioners to discuss overall rates of implant complications, such as peri-implantitis. Individual site- and patient-related risk factors should be highlighted for patients at the start of treatment. In order to do this properly, dentists must thoroughly review medical/dental histories and perform a comprehensive oral examination, including assessment of the periodontal condition and determination of the underlying process that caused tooth loss. Informed consent should be presented to the patient through visual aids and/or closed-loop discussions.
An informed consent document can be customized to reflect the individual risks of each patient. For example, in the consent for a heavy smoker with no interest in quitting, an additional statement might include: “I understand that because of past and current smoking habits I am at increased risk of treatment complications, including, but not limited to, implant failure and gum or bone loss around the implant. I understand that I am responsible for paying any additional fees associated with treatment required to address these increased risks.”
A similar statement could be utilized to highlight contributory medical conditions or medications that predispose the patient to serious complications, such as increased bleeding, that may require hospitalization. While this does not relieve the provider of all medicolegal issues, it should improve patient understanding of the need for further dental or medical intervention. Additionally, reinforcing the importance of regular maintenance with written consent emphasizes its importance to the long-term health of the implant(s). With proper treatment planning, clinicians should anticipate complications and inform patients of their degree of likelihood prior to the initiation of treatment.
CASE REPORT
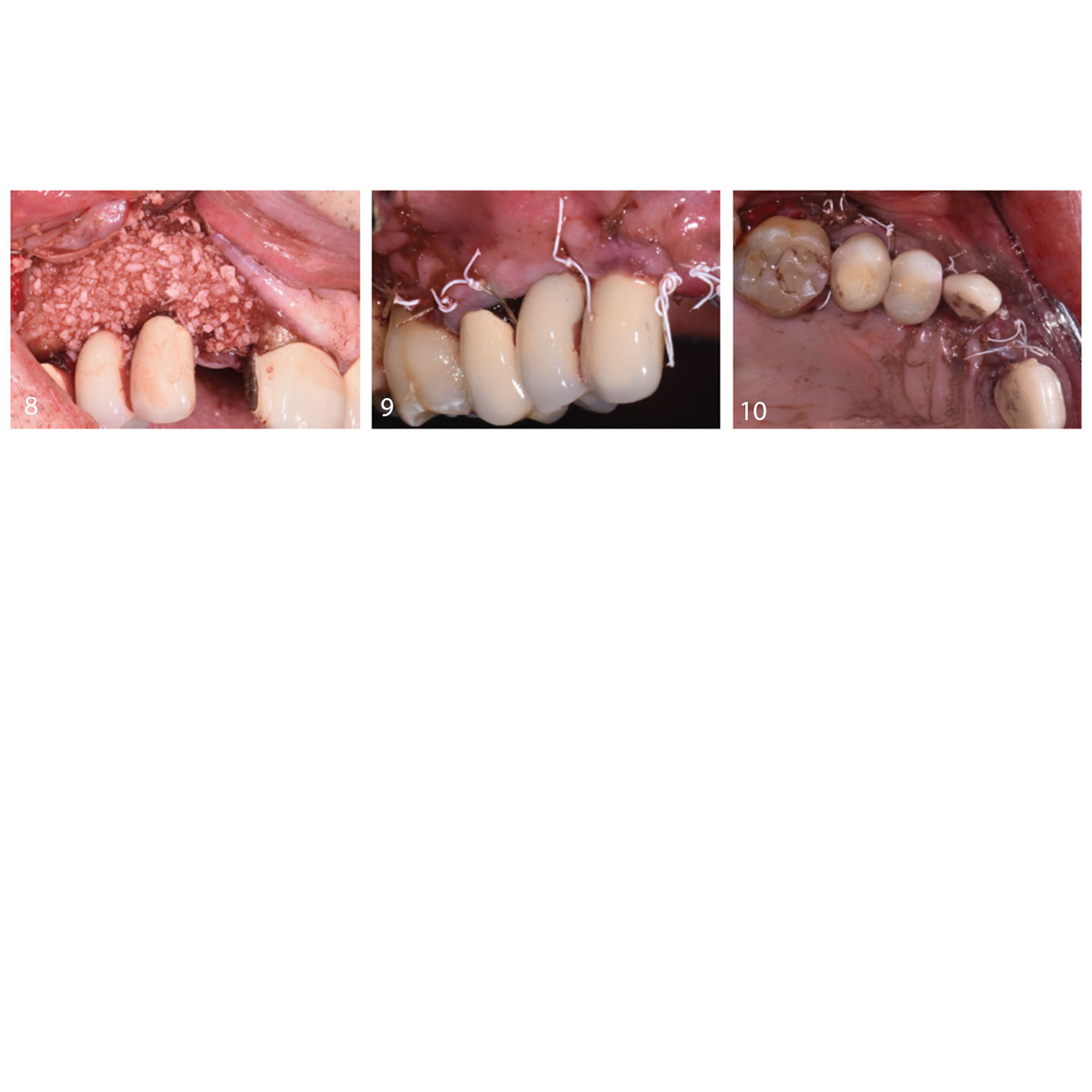
The following case considers many of these risk factors in practice and the steps taken to correct and prevent implant complications. A 66-year-old male presented to the graduate periodontics clinic at the University of Texas Health San Antonio School of Dentistry interested in implant therapy to replace missing and non-restorable teeth (Figure 1 through Figure 10). The patient had a previous history of myocardial infarctions managed with daily 81-mg aspirin and fish oil supplements.

The following surgical plan provides a treatment modality for each risk factor or problem noted in the initial patient evaluation. Each procedure was discussed prior to surgery. Consents that also described the patient’s unique risk for increased bleeding during the perioperative period due to medications were obtained. Procedures were performed using IV conscious sedation. The treatment plan included:
- Immediate implant placement for a non-restorable anterior tooth
- Bone grafting at time of implant placement to increase facial plate thickness
- Implant flap debridement and osseous recontouring to eliminate the peri-implant defect with moderate pocketing and bleeding
- Buccal contour augmentation to augment any hard tissue deficiencies
- Connective tissue grafting to thicken his periodontal phenotype
Implants #5 and 6 were placed more than 10 years ago. A 6 mm pocket depth with bleeding at #6-M and a periapical radiolucency were apparent at implant #6 at the time of initial exam. Tooth #7 was determined to have a vertical root fracture and was deemed non-restorable. Black discoloration of tooth #4 was due to treatment with silver diamine fluoride.
On the day of surgery, care was initially taken to prepare a partial thickness dissection at implants #5 and 6. A thin facial plate and thin periodontal phenotype can be appreciated clinically. The buccal malpositioning of implant #6 presented an esthetic concern and contributed to the hard tissue deficiency in the right anterior maxilla. Tooth #7 was extracted with a minimally traumatic technique. After socket degranulation, a 4-mm-deep interproximal defect was noted between implant #6 and tooth #7. A fenestration was noted at the facial plate of site #7 that was 1.5 mm wide and 1.5 mm high.

Based upon the palatal position for the planned implant at #7, the short root of the extracted tooth allowing for apical stability of the implant fixture, and the need for grafting at other implants in this sextant, a decision was made to proceed with an immediate dental implant at site #7. A bone level, tapered 3.3-mm-wide and 10-mm-long implant was placed per the manufacturer’s protocol. In this case, restoratively driven placement and emergence profile development for an anterior restoration made placement 3 to 4 mm apical to the future free gingival margin ideal. The implant was also positioned ≥ 1.5 mm mesiodistal from the adjacent teeth and ≥2 mm palatal from the facial plate. At this time, implants #5 and 6 were thoroughly debrided using titanium hand scalers and saline. All sharp bony peaks were smoothed to create a favorable architecture.
Periosteal releasing incisions were prepared to allow for primary closure of the augmented sites. Full-thickness mucoperiosteal flaps were elevated to allow buccal bony exposure at implants #5 and 6. The deficient facial plate at #5 to 7 was augmented with lateral onlay grafting using mineralized freeze-dried bone allograft. The goal was to correct the hard tissue deficiency and increase facial plate thickness prior to the implant restoration. The release needed for tension-free primary closure can result in coronal transposition of alveolar mucosa at augmented sites. A connective tissue graft should be considered at the time of implant uncovery to enhance tissue thickness, especially in patients with thin phenotypes. The restorative dentist delivered a maxillary Essix retainer to replace missing #7, and crown margins at #8 were further smoothed.
SUMMARY AND CONCLUSIONS
Whether for one implant or full-mouth, implant-assisted rehabilitation, each patient should be evaluated to determine the factors that may increase his or her risk for treatment complications. Patients should be properly informed about their treatment and its overall risks. Informed consent requires that patients understand the surgical and restorative goals, risks and benefits of therapy, how their individual risk factors might affect long-term success, and the potential need for additional treatment, should it arise.
The etiology of peri-implantitis may be multifactorial due to the variety of potential risk factors that can contribute to peri-implant disease at site- and patient-related levels. However, with early intervention, excellent oral hygiene and regular maintenance, clinicians and patients can work together to manage the disease process. Implant complications can be managed successfully when challenges are anticipated and a detailed treatment plan is presented after the initial patient evaluation.
REFERENCES
- Roccuzzo M, Bonino L, Dalmasso P, Aglietta M. Long-term results of a three arms prospective cohort study on implants in periodontally compromised patients: 10-year data around sandblasted and acid-etched (SLA) surface. Clin Oral Implants Res. 2014;25:1105–1112.
- Hämmerle CH, Tarnow D. The etiology of hard- and soft-tissue deficiencies at dental implants: a narrative review. J Periodontol. 2018;89(Suppl 1):S291–S303.
- Schwarz F, Derks J, Monje A, Wang HL. Peri-implantitis. J Periodontol. 2018;89(Suppl 1):S267–S290.
- Cho-Yan Lee J, Mattheos N, Nixon KC, Ivanovski S. Residual periodontal pockets are a risk indicator for peri-implantitis in patients treated for periodontitis. Clin Oral Implants Res. 2012;23:325–333.
- Nibali L, Farias BC, Vajgel A, Tu YK, Donos N. Tooth loss in aggressive periodontitis: a systematic review. J Dent Res. 2013;92:868–875.
- Dopico J, Nibali L, Donos N. Disease progression in aggressive periodontitis patients. A retrospective study. J Clin Periodontol. 2016;43:531–537.
- Swierkot K, Lottholz P, Flores-de-Jacoby L, Mengel R. Mucositis, peri-implantitis, implant success, and survival of implants in patients with treated generalized aggressive periodontitis: 3- to 16-year results of a prospective long-term cohort study. J Periodontol. 2012;83:1213–1225.
- Loke W, Coomes AM, Eskow A, Vierra M, Mealey BL, Huynh-Ba G. Formulating a global prognosis and treatment plan for the periodontally compromised patient: a reconstructive vs. an adaptive approach. Compend Contin Educ Dent. 2014;35:668–670,672–673,676–677
- Ferreira SD, Silva GL, Cortelli JR, Costa JE, Costa FO. Prevalence and risk variables for peri-implant disease in Brazilian subjects. J Clin Periodontol. 2006;33:929–935.
- Costa FO, Takenaka-Martinez S, Cota LO, Ferreira SD, Silva GL, Costa JE. Peri-implant disease in subjects with and without preventive maintenance: a 5-year follow-up. J Clin Periodontol. 2012;39:173–181.
- Staubli N, Walter C, Schmidt JC, Weiger R, Zitzmann NU. Excess cement and the risk of peri-implant disease — a systematic review. Clin Oral Implants Res. 2017;28:1278–1290.
- Linkevicius T, Vindasiute E, Puisys A, Linkeviciene L, Maslova N, Puriene A. The influence of the cementation margin position on the amount of undetected cement. A prospective clinical study. Clin Oral Implants Res. 2013;24:71–76.
- Korsch M, Marten SM, Walther W, Vital M, Pieper DH, Dötsch A. Impact of dental cement on the peri‐implant biofilm — microbial comparison of two different cements in an in vivo observational study. Clin Implant Dent Relat Res. 2018;20:806–813.
- Monje A, Catena A, Borgnakke WS. Association between diabetes mellitus/hyperglycaemia and peri-implant diseases: systematic review and meta-analysis. J Clin Periodontol. 2017;44:636–648.
- Temmerman A, Rasmusson L, Kübler A, Thor A, Merheb J, Quirynen M. A prospective, controlled, multicenter study to evaluate the clinical outcome of implant treatment in women with osteoporosis/ osteopenia: 5-year results. J Dent Res. 2019;98:84–90.
- Chappuis V, Avila‐Ortiz G, Araújo MG, Monje A. Medication‐related dental implant failure: systematic review and meta‐analysis. Clin Oral Impl Res. 2018;29(Suppl 16):55–68.
- Atieh MA, Alsabeeha NH, Faggion CM Jr, Duncan WJ. The frequency of peri‐implant diseases: a systematic review and meta‐analysis. J Periodontol. 2013;84:1586–1598.
- Heitz-Mayfield LJ, Huynh-Ba G. History of treated periodontitis and smoking as risk for implant therapy. Int J Oral Maxillofac Implants. 2009;24:39–68.
- ALHarthi SS, Natto ZS, Midle JB, Gyurko R, O’Neill R, Steffensen B. Association between time since quitting smoking and periodontitis in former smokers in the National Health and Nutrition Examination Surveys (NHANES) 2009 to 2012. J Periodontol. 2019;90:16–25.
- Chen S, Buser D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla: as systematic review. Int J Oral Maxillofac Implants. 2014;29(Suppl):186–215.
- Kan JY, Rungcharassaeng K, Sciar A, Lozada J. Effects of the facial osseous defect morphology on gingival dynamics after immediate tooth replacement and guided bone regeneration: 1-year results. J Oral Maxillofac Surg. 2007;65(7 Suppl 1):13–19.
- Hämmerle CH, Chen ST, Wilson TG Jr. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int J Oral Maxillofac Implants. 2004;19:S26–S28.
- Huynh-Ba G, Pjetursson BE, Sanz M, Cecchinato D, Ferrus J, Lindhe J, Lang NP. Analysis of the socket bone wall dimensions in the upper maxilla in relation to immediate implant placement. Clin Oral Impl Res. 2010;21:27–42.
- DeGroot BS, Villar CC, Mealey BL, Mills MP, Prihoda TJ, Huynh-Ba G. Osseous healing around immediate implants placed using contour augmentation: a prospective case series. Int J Periodontics Restorative Dent. 2017;37:883–891.
- Buser D, Chappuis V, Kuchler U, et al. Long-term stability of early implant placement with contour augmentation. J Dent Res. 2013;92:S176–S182.
- Linkevicius T, Puisys A, Steigmann M, Vindasiute E, Linkeviciene L. Influence of vertical soft tissue thickness on crestal bone changes around implants with platform switching: a comparative clinical study. Clin Implant Dent Relat Res. 2015;17:1228–1236.
- Kan J, Rungcharassaeng K, Morimoto T, Lozada J. Facial gingival tissue stability after connective tissue graft with single immediate tooth replacement in the esthetic zone: consecutive case report. J Oral Maxillofac Surg. 2009;67:40–48.
From Decisions in Dentistry. July/August 2019;5(7):24–28.

