

A Multidisciplinary Approach to Salvaging an Implant in the Esthetic Zone
A dental implant with midfacial recession in the esthetic zone was successfully preserved using a hybrid abutment and a modified coronally advanced tunnel with a connective tissue graft. This case highlights the importance of correct three-dimensional implant placement, digital dentistry solutions, and an interdisciplinary approach to achieving functional and esthetic success.
In this case report, a dental implant was saved that had developed a midfacial recession in the esthetic zone. The decision to save the implant was based on the following:
- Implant was in a restorable position.
- Implant was healthy.
- No radiographic bone loss was present interproximally or on the facial aspect of the existing implant.
- Implant was placed at the correct 3D position.
Existing abutment could be used as a base to form a new hybrid (metal-zirconia abutment).
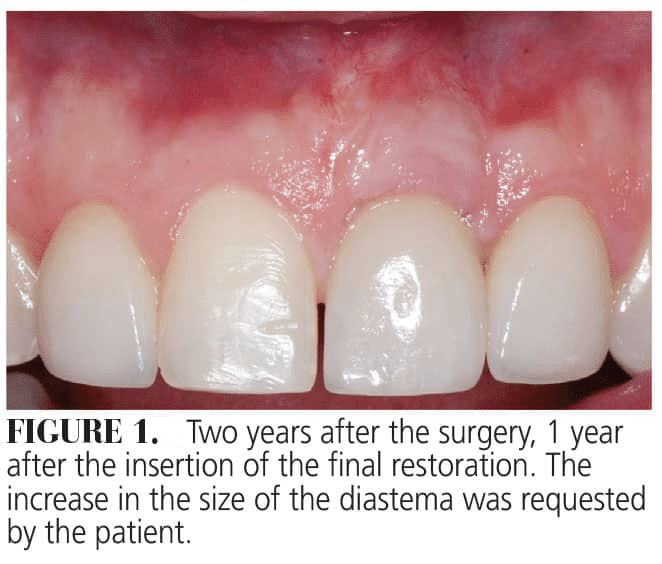
The soft tissue deficiency in both the horizontal and vertical direction was corrected with a modified coronally advanced tunnel and connective tissue graft (CTG). One year after treatment, the gingival margin was at the same level and color as the adjacent central incisor. Patient A requested that the diastema be enlarged; this was completed (Figure 1). Furthermore, the increase in the tissue thickness on the buccal aspect of the implant was sufficient to mask the gray hue from the implant/abutment and also allowed for a correct emergence profile of the implant-supported crown. The CTG was harvested from the tuberosity.
Advantages of this technique include an easy harvesting method and the presence of a low fatty tissue in the graft while providing a supply of rich connective tissue.1-3 The CTG may act as a biological filler, improving the adaptation and stability of the flap to the root during early wound repair.4 As a result, the gingival phenotype becomes thicker and the potential of achieving complete root coverage is higher. However, it is still unclear how much the composition of the graft influences the outcomes of mucogingival surgery. Limited evidence suggests that CTG impacts soft tissue thickness and keratinized tissue width while having no effect on the amount of root coverage.5,6 One of the drawbacks of the connective tissue harvested from the tuberosity is the possibility of an unesthetic hyperplastic response in cases with a thick phenotype or when esthetics is a concern.7
 The three-dimensional implant position is critical for saving an implant. If the implant is placed in a nonrestorable position, surgical procedures cannot correct the esthetic problems. The implant placement in the correct apico-coronal position is critical for the resultant restoration to be functional and esthetic. The biological width around the implant should be 3 to 4 mm in apico-coronal direction, accounting for 2 mm of junctional epithelium and 1 to 2 mm of connective tissue attachment.8 In this case, the implant platform was about 3 mm from the gingival margin.
The three-dimensional implant position is critical for saving an implant. If the implant is placed in a nonrestorable position, surgical procedures cannot correct the esthetic problems. The implant placement in the correct apico-coronal position is critical for the resultant restoration to be functional and esthetic. The biological width around the implant should be 3 to 4 mm in apico-coronal direction, accounting for 2 mm of junctional epithelium and 1 to 2 mm of connective tissue attachment.8 In this case, the implant platform was about 3 mm from the gingival margin.
Digital dentistry provided a solution to the lack of the implant component parts in this case. A hybrid abutment was created by scanning the original abutment and then fabricating a new retrofit abutment with the proper alignment to accept a new restoration. The original abutment was used as a hybrid abutment base on which the zirconia mesostructure was bonded in the laboratory with multilink abutment cement. The postsurgical replacement of the temporary crown played a critical role in the conditioning of the soft tissue — not only on the buccal aspect but also interproximal, facilitating the growth of the interdental papillae.
This case study showed the possibility of correcting a severe horizontal and vertical soft tissue deficiency and achieving a highly esthetic result and patient satisfaction. This case illustrates the advantages of using an interdisciplinary approach using three different disciplines (periodontal-orthodontic-restorative) to properly diagnose and treat this patient, resulting in a positive outcome, both functionally and esthetically.
References
- Zuhr O, Baumer D, Hurzeler M. The addition of soft tissue replacement grafts in plastic periodontal and implant surgery: critical elements in design and execution. J Clin Periodontol. 2014;41(Suppl 15):S123-142.
- Roccuzzo M, Dalmasso P, Pittoni D, Roccuzzo A. Treatment of buccal soft tissue dehiscence around single implant: 5-year results from a prospective study. Clin Oral Investig. 2019;23:1977-1983.
- Sanz-Martin I, Rojo E, Maldonado E, Stroppa G, Nart J, Sanz M. Structural and histological differences between connective tissue grafts harvested from the lateral palatal mucosa or from the tuberosity area. Clin Oral Investig. 2019;23:957-964.
- Cairo F, Cortellini P, Pilloni A, et al. Clinical efficacy of coronally advanced flap with or without connective tissue graft for the treatment of multiple adjacent gingival recessions in the aesthetic area: a randomized controlled clinical trial. J Clin Periodontol. 2016;43:849-856.
- Amin PN, Bissada NF, Ricchetti PA, Silva APB, Demko CA. Tuberosity versus palatal donor sites for soft tissue grafting: A split-mouth clinical study. Quintessence Int. 2018;49:589-598.
- Rojo E, Stroppa G, Sanz-Martin I, Gonzalez-Martin O, Alemany AS, Nart J. Soft tissue volume gain around dental implants using autogenous subepithelial connective tissue grafts harvested from the lateral palate or tuberosity area. A randomized controlled clinical study. J Clin Periodontol. 2018;45:495-503.
- Tavelli L, Bacootchi S, Greenwell H, Wang H Is a sorf tissue graft harvested from the maxillary tuberosity the approach of choice in an isolated site? J Periodontol. 2019;90:821-825.
- Berglundh T, Lindhe J. Dimension of the periimplant mucosa. Biological width revisited. J Clin Periodontol. 1996;23:971-973.
This information originally appeared in Boeriu S, Hottel TL, Chirla C, Chirla P. Recession defects on a maxillary single tooth implant. Decisions in Dentistry. March 2024;10(2):16-19.
