

Failure of Mini Implants: A Case Report
This case report highlights the complications and ultimate failure of using mini implants to replace a single mandibular first molar.
Following is a case report of the failure of two mini implants used to replace a single mandibular first molar. The failure resulted in surgical removal of both implants, osseous grafting, and, eventually, replacement with a conventionally sized implant.
CASE REPORT
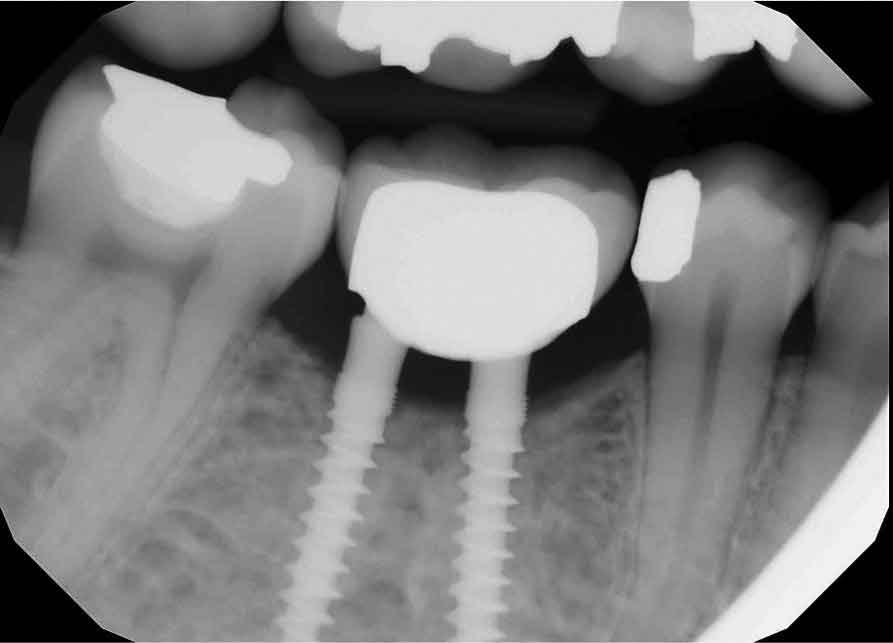
The patient, a 35-year-old woman, presented to a general dentist in April 2010 for routine examination and dental prophylaxis. Records from that office indicated no history of periodontal diseases, but probing depths were not recorded. Missing teeth included all third molars and the mandibular right first molar (#30; Figure 1). It was noted that tooth #30 had been extracted 10 years prior due to an irreparable tooth fracture. Her medical history was insignificant: no medications, no allergies, no systemic disease, and no history of hospitalization except for childbirth.

In January 2014, the general dentist suggested replacing edentulous site #30 with an implant. To avoid surgery, mini implants were recommended and placed without mucoperiosteal flap reflection. The implants and single molar restoration at 6 months post-placement (June 2014) are seen in Figure 2.
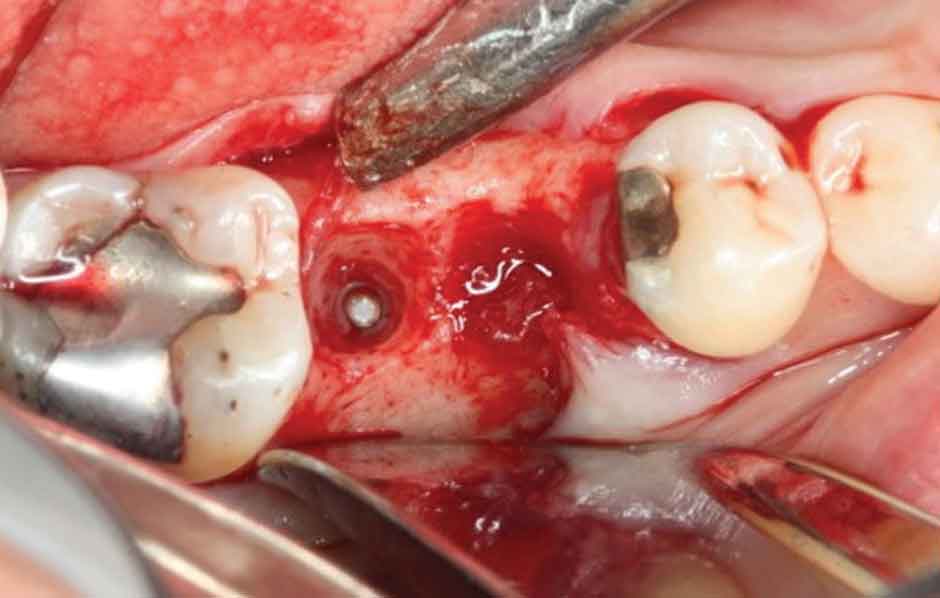
The patient was seen on emergency having been referred to a periodontist in May 2015 with a chief complaint of “severe” jaw pain associated with the mini implant site. The examination revealed the implant fixture exhibited Grade II mobility, and the buccal marginal crown extension overlapped the attached gingiva, essentially creating an “engineered” Grade III furcation involvement. While there was little clinical inflammation (Figures 3 and 4), the exam revealed a diminished width of keratinized and attached gingiva at the buccal aspect of the prosthesis; that is, the mucogingival junction was nearly even with the extended crown margin (Figure 3). Based on the patient’s complaint of pain and Grade II prosthesis mobility, a diagnosis of fractured implant(s) was made and it was decided to remove both implants.


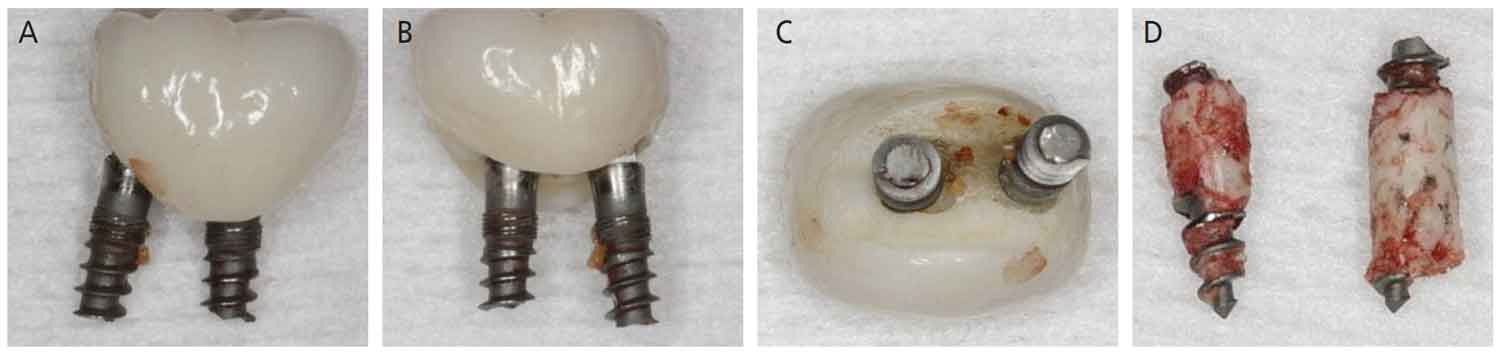
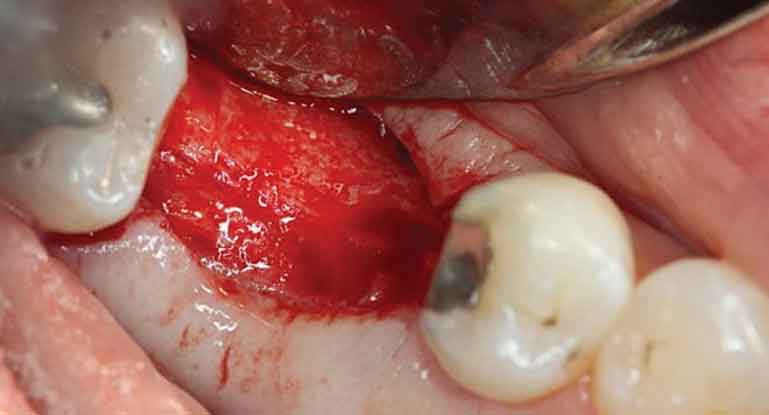
The surgery was accomplished in late May 2015 and consisted of removing both implants and superstructure as a single unit by gentle use of a #217 extraction forceps. Once removed, resorption of the alveolar ridge to the lingual was noted (Figure 4). A full-thickness mucoperiosteal flap was reflected, allowing visualization of the remaining apical portions of both implants at roughly 5 and 6 mm (mesial and distal implants, respectively) below the bony crest (Figure 5). The apical portion of each implant was osseointegrated, necessitating removal by use of a trephine bur (Figures 6A through 6D). Upon retrieval of the fractured implants, it was determined both had dimensions of 2.4×12 mm. The osseous defects were grafted with particulate cancellous bone allograft and covered with pericardium membrane. Next, the surgical site was closed with 4.0 vicryl sutures.
apical portion of the distal implant still within
bone prior to removal using a 3-mm-diameter
trephine bur.
In November 2015, at 6 months post-osseous grafting, the surgical site was reentered, revealing a well-formed alveolar ridge, with little evidence of resorption in the buccal-lingual dimension (Figure 7). Subsequently, a 4.8×10 mm tissue level, wide neck endosseous implant was positioned, a healing cap placed, and the flap closed with interrupted vicryl sutures.


After 9 months of healing, the implant was ready for restoration and the patient was referred to her general dentist. A single crown was cemented in August 2016. During a routine follow-up appointment in September 2020, a periapical radiograph showed good bone stabilization and no discernable changes in osseous contour or crestal level since 2016 (Figure 8 and Figure 9).
The next installment of Perio Update will feature a discussion of this case.
This information originally appeared in Beaini NE, Cobb CM. Avoiding complications with mini implants. Decisions in Dentistry. 2021;7(7):31–34.
