

The Impact of Digital Workflows on Implant Treatment
Explore the role of digital technologies in implant therapy, from precise data collection to virtual planning, optimizing clinical outcomes and enhancing patient care.
Implant therapy is considered an integral part of dental treatment for many patients. Since the introduction of implant therapy almost 30 years ago, the field has changed significantly. One change that reshaped the clinical approach to implant treatment planning and therapy was the introduction of digital technologies and workflows. Due to their advantages in accurate diagnosis, treatment planning, and executing implant procedures, digital technologies are becoming more widely utilized. Elements of a digital workflow include data collection, computer aided design/computer aided manufacturing (CAD/CAM), and implant placement (Figure 1).
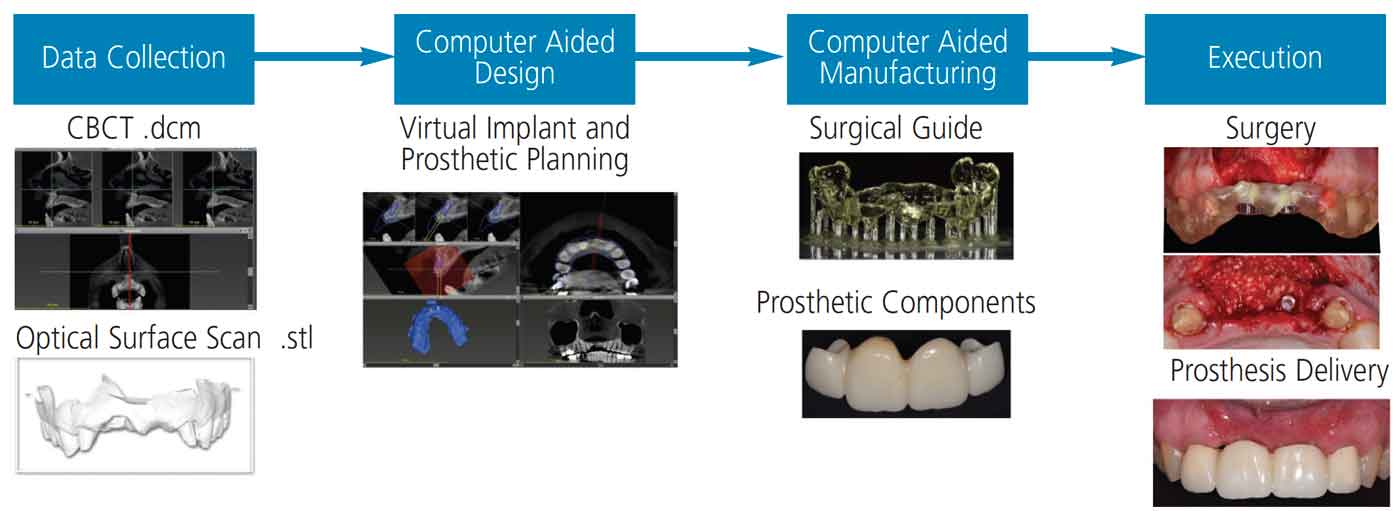
The first step in the digital workflow is data collection using digital imaging, such as cone beam computed tomography (CBCT) and optical surface scanning, which includes intraoral scanning and extraoral model scanning. Intraoral or extraoral optical surface scans allow the dentist to accurately represent both teeth and soft tissue as a digital Standard Tessellation Language (STL) file. The STL file is transported to a virtual implant planning software, where the CAD process begins. The STL file is registered and merged with the Digital Imaging and Communications in Medicine (DICOM or .dcm) files obtained from the CBCT imaging. Next, implant position is planned according to appropriate anatomical and prosthetic principles. Additionally, the same software can design the prostheses, surgical templates and respective sleeves. Use of CAM processes as the final step involves subtractive or additive technology to fabricate surgical templates and implant-supported restorations.1
Accuracy of static computer assisted implant surgeries (sCAIS) is defined as deviations between the planned and fixed implant.2 Studies have shown that all sCAIS show some degree of imprecision resulting in deviations between actual and virtual implant positions.3 This can be attributed to errors in the digital workflow: data collection, transfer or processing, CAD (or virtual) implant treatment planning, CAM, and surgical execution. During data collection, accuracy of the CBCT can be affected by features of the machine, radiation exposure, software used to view DICOM data, patient movement, and artifacts from restorations.4 When comparing conventional models with optical scans, in vivo data is lacking due to difficulty in obtaining a standardized protocol for model recording and reproduction. However, from the available limited data clinicians have made suggestions for achieving predictable clinical outcomes.5
When designing the virtual implant position, clinicians should keep in mind anatomical positions of adjacent teeth or implants and vital structures, such as the inferior alveolar nerve, mental nerve, maxillary sinus, and nasal floor. Once the implant position is planned according to the appropriate anatomical and prosthetic considerations, the clinician can start designing the surgical template with the following considerations: type of support (bone, mucosa, tooth, or fixture), sleeve-to-bone height, drilling distance, and the number of teeth used as support in a tooth-supported template.
References
- Arunyanak SP, Harris BT, Grant GT, Morton D, Lin WS. Digital approach to planning computer-guided surgery and immediate provisionalization in a partially edentulous patient. J Prosthet Dent. 2016;116:8–14.
- Van Assche N, Vercruyssen M, Coucke W, Teughels W, Jacobs R, Quirynen M. Accuracy of computer-aided implant placement. Clin Oral Implants Res. 2012;23(Suppl 6):112–123.
- Tahmaseb A, Wu V, Wismeijer D, Coucke W, Evans C. The accuracy of static computer-aided implant surgery: a systematic review and meta-analysis. Clin Oral Implants Res. 2018;29(Suppl 16):416–435.
- Halperin-Sternfeld M, Machtei EE, Horwitz J. Diagnostic accuracy of cone beam computed tomography for dimensional linear measurements in the mandible. Int J Oral Maxillofac Implants. 2014;29:593–599.
- Flügge T, van der Meer WJ, Gonzalez BG, et al. The accuracy of different dental impression techniques for implant-supported dental prostheses: a systematic review and meta-analysis. Clin Oral Implants Res. 2018;29(Suppl 16):374–392.
This information originally appeared in Alqallaf H, Su FY, Goel A, Lin WS. Utilizing a digital workflow for implant treatment planning. Decisions in Dentistry. 2021;7(5)12-14,16-17.
