

Revitalizing Oral Health: A Case Study of Severe Periodontitis Management
Discover the interprofessional journey undertaken to treat severe periodontitis and associated systemic conditions in a 24-year-old woman.
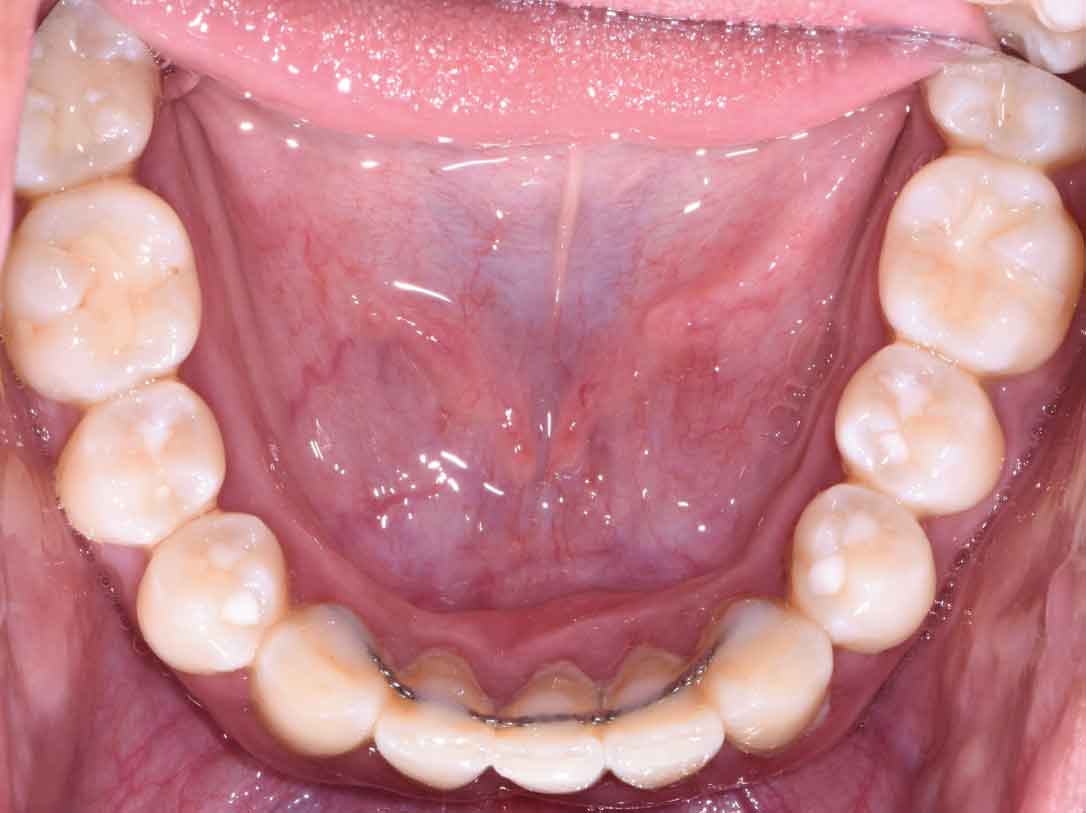
The following case outlines the interprofessional steps taken to treat severe periodontitis and its associated systemic conditions. A 24-year old Hispanic woman presented to the graduate periodontics clinic at the University of Texas Health San Antonio School of Dentistry interested in comprehensive periodontal care (Figure 1 through Figure 10). She had uncontrolled type 2 diabetes and morbid obesity, yet no other comorbidities.


Her periodontal tissues were generally pink-red and loosely attached, with heavy plaque, calculus, and debris noted throughout. She also presented with severe horizontal bone loss and vertical intrabony defects, multiple endo-periodontal lesions, furcation invasions, and secondary occlusal trauma. Probing depths ranged from 3 to 10 mm, with moderate bleeding on probing and suppuration; clinical attachment levels ranged from 1 to 11 mm. According to the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions, she was classified as having periodontitis, Stage IV, generalized, Grade C.1


After a thorough patient evaluation and review of various techniques and materials, a comprehensive treatment plan was developed, and consent was obtained. Nonsurgical and surgical procedures were performed using intravenous conscious sedation. The treatment plan included:
- Medical consultation to improve glycemic control.
- Full-mouth scaling and root planing, with extractions of periodontally hopeless teeth #10 and 15. She was prescribed amoxicillin 500 mg and metronidazole 500 mg every 8 hours for eight days during the perioperative period.
- Reevaluation of clinical parameters and further assessment of oral hygiene compliance was completed 12 weeks after initial therapy.
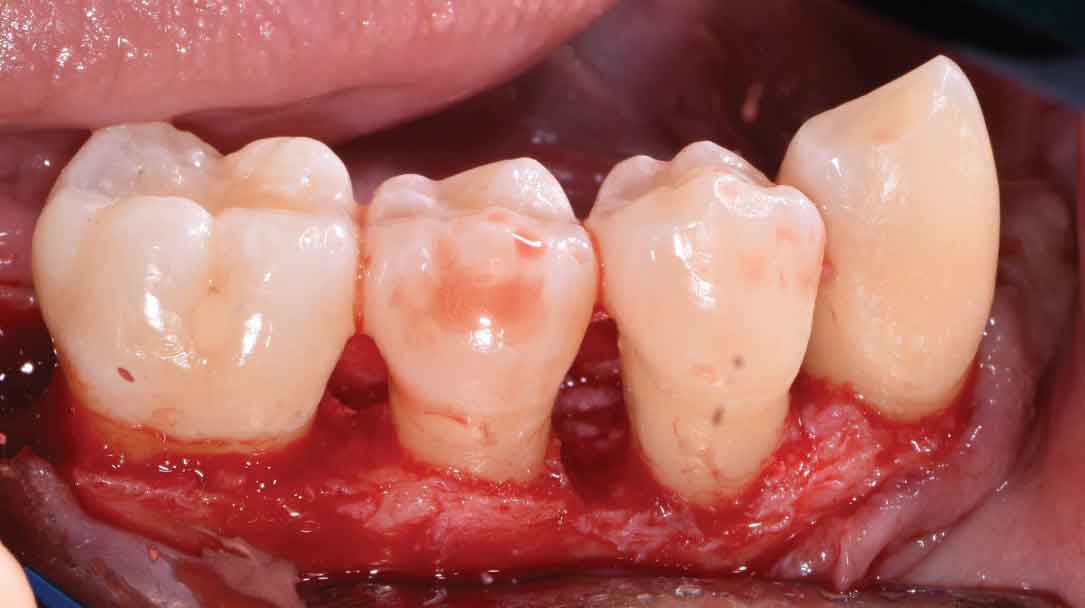
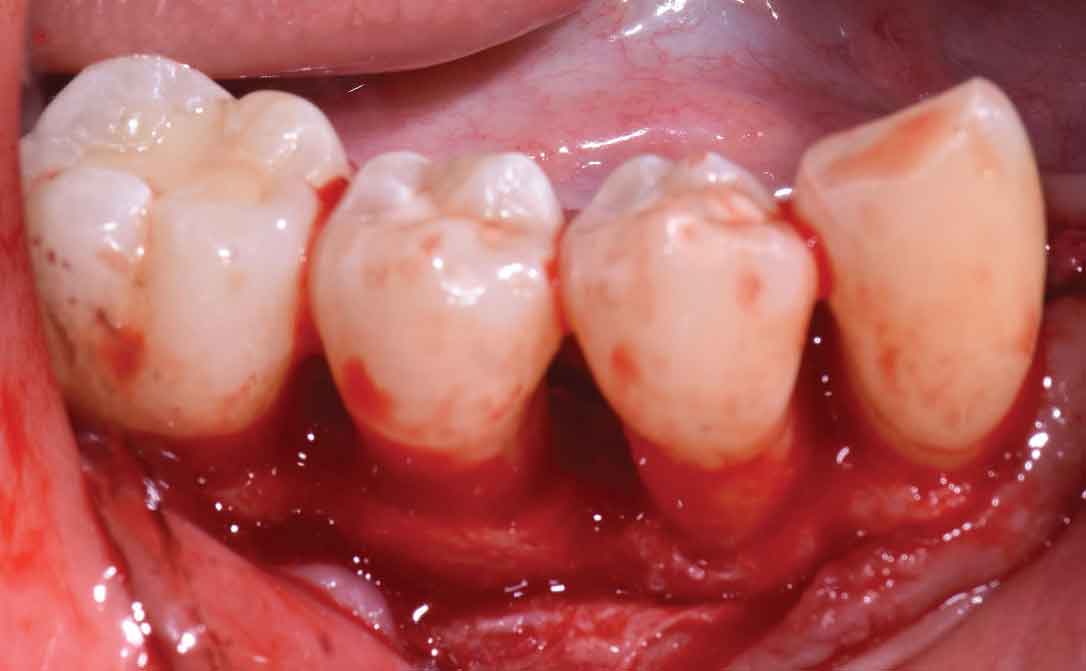
- Open flap debridement, with apically positioned flaps of the upper right, upper left, lower left, and lower right quadrants, and extractions of periodontally hopeless teeth #2, 4, 5, 19, 23, 24, 25 and 31 to arrest disease progression.
- Maxillary and mandibular interim removable dental prostheses to replace missing teeth, and a long-term provisional crown on #3 to stabilize her occlusion.
- Periodontal maintenance every three months, transitioning to a longer recall period based on stability and oral hygiene compliance.

The patient was first referred to her physician for proper management of her type 2 diabetes due to diabetes-related symptoms and a casual blood glucose reading of 333 mg/dL at her initial exam. With nutritional counseling, weight loss, and medication adherence, her HbA1c decreased from 12.7% to 6.5% over 6 months. The patient continued care with her physician every 3 months.
Full-mouth scaling and root planing and extractions of teeth #10 and 15 were completed at one appointment under an eight-day antibiotic regimen to maximize the clinical efficacy of nonsurgical therapy. Site #10 was not simultaneously augmented for future implant placement due to limited patient finances, a lack of ridge height, and a chief goal of stabilizing her aggressive periodontal breakdown. While oral hygiene measures were reviewed in-depth, they were reinforced 6 weeks after initial therapy owing to continued poor plaque control. Periodontal reevaluation was performed after 12 weeks, at which time she presented with definite improvements in her self-care and clinical parameters.

Surgical therapy was initiated to better visualize and debride the root surfaces, assess and modify the bony architecture, improve access for oral hygiene and maintenance, reduce pocketing and inflammation, gain clinical attachment, and slow/arrest disease progression. Open flap debridement with apically positioned flaps was performed in all four quadrants, with osseous recontouring as indicated. Periodontal regeneration was not attempted due to limited patient finances. The remaining periodontally hopeless teeth were extracted, with immediate delivery of maxillary and mandibular Essix retainers for esthetics. Interim removable dental prostheses and a long-term provisional crown #3 were later fabricated to stabilize her occlusion before proceeding with definitive removable appliances.

The patient continued in a supportive periodontal maintenance program every 3 months. Oral hygiene techniques were reviewed, and a prescription fluoride dentifrice was provided to reduce the incidence of root caries and sensitivity. Almost 2 years later, she presented with probing depths of 2 to 3 mm, with nonbleeding 4-mm pocketing in select posterior teeth. Her HbA1C values were routinely < 7%. Despite her initial presentation, she maintained most of her otherwise terminal dentition and renewed her quality of life.
The impact of periodontal medicine can truly be life-changing. Diabetes mellitus, cardiovascular disease, obesity, and other inflammatory disorders can accelerate periodontal disease progression and diminish therapeutic response. As the links between periodontitis and systemic disease become more apparent, it is important to be mindful that association does not imply causation. An interprofessional approach to managing systemic conditions as part of periodontal care can improve clinical outcomes and patients’ overall well-being.
Reference
- Caton JG, Armitage G, Berglundh T, et al. A new classification scheme for periodontal and peri-implant diseases and conditions — introduction and key changes from the 1999 classification. J Clin Periodontol. 2018;45(Suppl 20):S1–S8.
This information originally appeared in Saltz A. Periodontal medicine: from teeth to total body health. Decisions in Dentistry. 2021;7(3):25–31.
