

The Concept of Biologic Width in Restorative Dentistry
Crown lengthening surgery can help to create enough biologic width for teeth with subgingival caries, inadequate crown length, or tooth fracture.
Frequently, the general dentist faces a dilemma about whether a carious tooth can be restored to function or if extraction is warranted. A healthy periodontium with a sound dentition is a prerequisite for a favorable long-term prognosis. The American Academy of Periodontology’s (AAP) Glossary of Periodontal Terms defines clinical crown lengthening as a surgical procedure that aims at exposing sound tooth structure for restorative purposes via apical repositioning of the gingival tissue, with or without removal of alveolar bone. This is a prescription procedure designed to achieve better function and improve the predictability of restorative treatment and maintenance care.
Indications for crown lengthening from a restorative standpoint include ensuring the necessary tooth length for successful restoration, access (eg, removal of subgingival caries), finishing tooth preparation, and impression making. The procedure also provides stable gingival margins around the tooth and can likely prevent irritational gingival inflammation. This Perio Update will discuss the concept of biological width (also known as a supracrestal tissue attachment, as per the AAP Classification Workshop 2017).
Attributed to D. Walter Cohen, DDS, while lecturing at Walter Reed Army Medical Center in 1962, the term biologic width has been used in dentistry for nearly 60 years. Gargiulo et al1 and Vacek2 et al further describe the gingival dimension and dentogingival junction relationship in humans, providing average tissue measurements in millimeters (Figure 1). The dentogingival junction average measurements are still used today as helpful guidelines when discussing the biologic width concept.
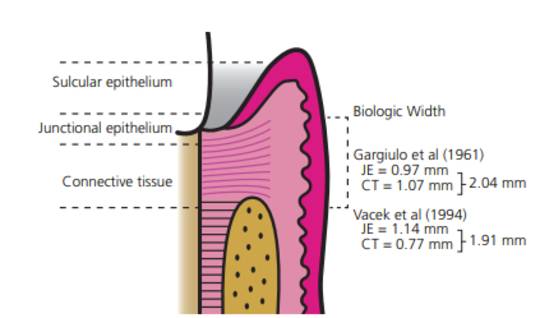
and Vacek et al.2 JE: junctional epithelium attachment; CT: connective tissue
attachment.
Biologic width represents the sum of the epithelial and connective tissue measurements. As depicted in Figure 1, the biologic width is considered to be 2.04 mm (based on the mean measurement of the epithelial attachment of 0.97 mm, and a connective tissue attachment of 1.07 mm), and the mean measurement of the sulcus depth of 0.69.1,3 The new periodontal classification guidelines replaced the term biologic width with supracrestal tissue attachment, consisting of junctional epithelium and supracrestal connective tissue.
It is generally accepted that maintaining the integrity of an average 3 mm biologic width reduces the risk of periodontal attachment loss.4,5 Subgingival restorative margins induce the periodontal inflammation resulting from biologic width violation. Use of crown lengthening surgery can establish a satisfactory biologic width for teeth with subgingival caries, inadequate crown length or tooth fracture; it can also address esthetic concerns.
References
- Gargiulo AW, Wentz FM, Orban B. Dimensions and relations of the dentogingival junction in humans. J Periodontol. 1961;32:261–267.
- Vacek JS, Gher ME, Assad DA, Richardson AC, Giambarresi LI. The dimensions of the human dentogingival junction. Int J Periodontics Restorative Dent. 1994;14:154–165.
- Nugala B, Kumar BS, Sahitya S, Krishna PM. Biologic width and its importance in periodontal and restorative dentistry. J Conserv Dent. 2012;15:12–17.
- Fugazzotto PA. The Role of Crown-Lengthening Therapy. In: Fugazzotto PA. Periodontal–Restorative Interrelationships: Ensuring Clinical Success. Hoboken, NJ: John Wiley and Sons, Inc; 2011:31–87.
- Robbins JW. Esthetic gingival recontouring — a plea for honesty. Quintessence Int. 2000;31:553–556.
This information originally appeared in Goel A, Mott DA, Wilkerson C, Ellzey AT. Concepts and considerations for surgical crown lengthening. Decisions in Dentistry. 2021;7(1):36–39.
