
 akinbostanci / iStock / Getty Images Plus
akinbostanci / iStock / Getty Images Plus
Supporting Positive Implant Outcomes
While implant therapy offers a high rate of success, it is not without potential pitfalls. This Perio Update will review the key points to hit while in the treatment planning phase to ensure the success of implant therapy.
Oral reconstruction and rehabilitation using dental implants in patients with partial and complete edentulism have become extremely common in clinical practice. At the same time, patient expectations about the outcomes of implant therapy have also risen. Deeb et al1 report that 49% of patients who had a consultation expected dental implants to last more than 20 years. While high implant success and survival rates have been noted, the prevalence of peri-implantitis was reported to range from 1% to 47%.2,3 In addition, the progression of peri-implantitis follows a nonlinear, accelerating pattern, and the onset of bone loss was usually within 3 years of function among the affected implants.4 Accordingly, clinicians need to realize there is a wide gap between patient expectations and epidemiologic data. In light of the fact that more than 50% of patients say a dentist is their most significant source of information on implants, clinicians need to present realistic outcomes of implant-supported restorative therapy.1 Therefore, recognizing risk factors, developing a proper treatment plan, and providing adequate maintenance care at general dental offices are necessary to minimize complications and improve outcomes.
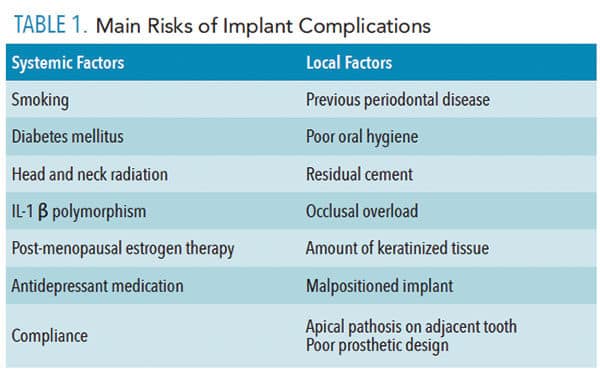
Because most implant complications are multifactorial, it is difficult to identify one specific factor in the clinical setting that can lead to implant failure. Thus, the treatment plan for dental implants must be comprehensive and include a multidisciplinary approach. Each clinician must obtain a complete medical history, followed by extraoral and intraoral examinations—including the assessment of the periodontal and periapical status of existing teeth. Risk of implant failure can be classified into two main groups: systemic conditions and local factors (Table 1).5–7 The diagnosis phase helps clinicians and patients identify many preexisting determinants that could negatively affect the outcome. If any potential causative factors affecting long-term implant success are recognized at this phase, further investigation and discussion of each risk factor is needed.
IMPLANT TREATMENT PHASE
Prior to implant placement, all presenting intraoral pathologic conditions should be treated. These include the treatment of periodontal diseases, endodontic lesions, and caries. Patient compliance with plaque control should be monitored during the initial phase before moving to implant therapy. Once any inflammatory disease has been addressed, an individualized restorative treatment plan should be developed. Three-dimensional (3D) radiographic evaluation using cone-beam computed tomography with a radiographic marker, along with a diagnostic wax-up, are essential steps in this process (Figure 1). These 3D images allow clinicians to assess vital anatomical structures, such as the inferior alveolar nerve, mental foramen, lingual concavity of the posterior mandible, incisive canal, shape and pathological changes of the maxillary sinus, and the endodontic status of adjacent teeth. Implant simulation software is used to evaluate the local anatomical structures and improve clinicians’ understanding of possible future implant positions (Figure 2).

In Case 1 (Figure 3 and Figure 4), the surgeon accurately predicted the alveolar ridge width was inadequate for implant placement based on the restorative plan, and that simultaneous bone augmentation was needed at the time of implant placement. Following an appropriate healing period, provisional and definitive restorations were delivered (Figure 5). Envisioning the outcome before treatment is provided—referred to as “top down” treatment planning—is vital to the success of therapy. Malpositioned implants, especially those placed too buccally, might have higher susceptibility for peri-implant complications. Monje et al8 found in his survey study that most of the experienced implantologists agreed that prevalence of peri-implantitis was higher in malpositioned implants. However, more controlled studies are needed to confirm this outcome. Good communication and a team approach are necessary to achieve functional and esthetic outcomes in implant dentistry.

REFERENCES
- Deeb G, Wheeler, B, Jones M, Carrico C, Laskin D, Deeb JG. Public and patient knowledge about dental implants. J Oral Maxillofac Surg. 2017;75:1387–1391.
- Derks J, Tomasi C. Peri-implant health and disease. A systematic review of current epidemiology. J Clin Periodontol. 2015;42 (Suppl 16):S158–S171.
- Buser D, Janner S, Wittneben JG, Brägger U, Ramseier CA, Salvi GE. 10-year survival and success rates of 511 titanium implants with a sandblasted and acid-etched surface: a retrospective study in 303 partially edentulous patients. Clin Implant Dent Relat Res. 2012;14:839–851.
- Derks J, Schaller D, Håkansson J, Wennström JL,Tomasi C, Berglundhl T. Peri-implantitis — onset and pattern of progression. J Clin Periodontol. 2016;43:383–388.
- Moy PK, Medina D, Shetty V, Aghaloo TL. Dental implant failure rates and associated risk factors. Int J Oral Maxillofac Implants. 2005;20:569–577.
- Peri-implant mucositis and peri-implantitis: a current understanding of their diagnoses and clinical implications. J Periodontol. 2013;84:436–443.
- Renvert S, Quirynen M. Risk indicators for peri-implantitis. A narrative review. Clin Oral Implants Res. 2015;26 (Suppl 11):15–44
- Monje A, Galindo-Moreno P, Tözüm TF, Suárez-López del Amo F, Wang HL. Into the paradigm of local factors as contributors for peri-implant disease: short communication. Int J Oral Maxillofac Implants. 2016;31:288–292.
This information originally appeared in Hamada Y, Hill K, Chang J, John V. Addressing risks of implant complications. Decisions in Dentistry. 2017;3(10):14–21.
