

Managing Patients With Autoimmune Diseases
The following strategies will help clinicians identify and treat this clinically diverse patient population.
The following strategies will help clinicians identify and treat this clinically diverse patient population
PURCHASE COURSE
This course was published in the October 2017 issue and expires October 2020. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
There are more than 100 types of autoimmune disorders,1 and more than 50 million people are affected in the United States alone.1,2 Autoimmune diseases affect women 75% more than men and are among the top 10 causes of death for women under 65.1 Autoimmune diseases cluster in families.1 For many individuals, diagnosis may take years, often leading to frustration, misdiagnosis and depression. Dental professionals play a critical role in helping to identify undiagnosed individuals. The diseases themselves and related medication management not only adversely affect general and oral health, they also impact quality of life. With the goal of helping providers safely manage patients with autoimmune diseases, this paper will highlight key concepts of autoimmunity and present a risk assessment model for use by oral health professionals.
This course was published in the October 2017 issue and expires October 2020. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Explain the incidence and pathophysiology of autoimmune diseases.
- Describe the systemic and oral manifestations of autoimmune disorders.
- Discuss practice management considerations when caring for this patient population.
The human immune system exhibits self-tolerance, which is the ability to recognize the difference between “self” and “foreign” antigens. When innate mechanisms that normally prevent the immune system from attacking self-antigens fail, activated T cells and antibodies begin to attack the individual’s own tissues, a process known as autoimmunity. Conditions associated with autoimmunity are collectively called autoimmune diseases.3–5
Antibodies that cause autoimmunity — known as autoantibodies — bind to self-antigens and form complexes that are deposited in tissues, organs or blood vessels. Deposition of these bound antibodies accounts for the tissue destruction, inflammation and systemic complications observed with autoimmune diseases. Autoantibodies also cause disease by inhibiting receptor function, as in myasthenia gravis, in which acetylcholine receptors are inhibited and neuromuscular transmission fails, causing paralysis of the muscles of the head and neck. In hyperthyroidism, autoantibodies directly stimulate receptors on thyroid cells that would normally be hormonally stimulated.2–4
Development of autoimmunity typically depends on two factors. First, an individual inherits genes that increase susceptibility and contribute to failure of self-tolerance. Second, one or more environmental triggers initiate activation of autoantibodies; these may include infection, fever or severe trauma. An infection triggers a local immune response that releases cytokines and chemical stimulators that activate self-reactive T cells, producing an immune attack against self-antigens. Injured tissues release antigens that are not normally seen by the immune system, and this can also initiate an autoimmune reaction.3,4 Emerging evidence demonstrates that infections either precede or coincide with disease onset, reflecting a seasonal pattern with specific infectious agents.6 For example, flares in systemic lupus erythematosus have been observed with infections with Epstein-Barr virus in winter, and type 1 diabetes mellitus onset has been shown to be preceded by infection with coxsackievirus in late summer.6 Other identified environmental triggers include low levels of vitamin D, exposure to UV radiation and fluctuations in melatonin.6,7
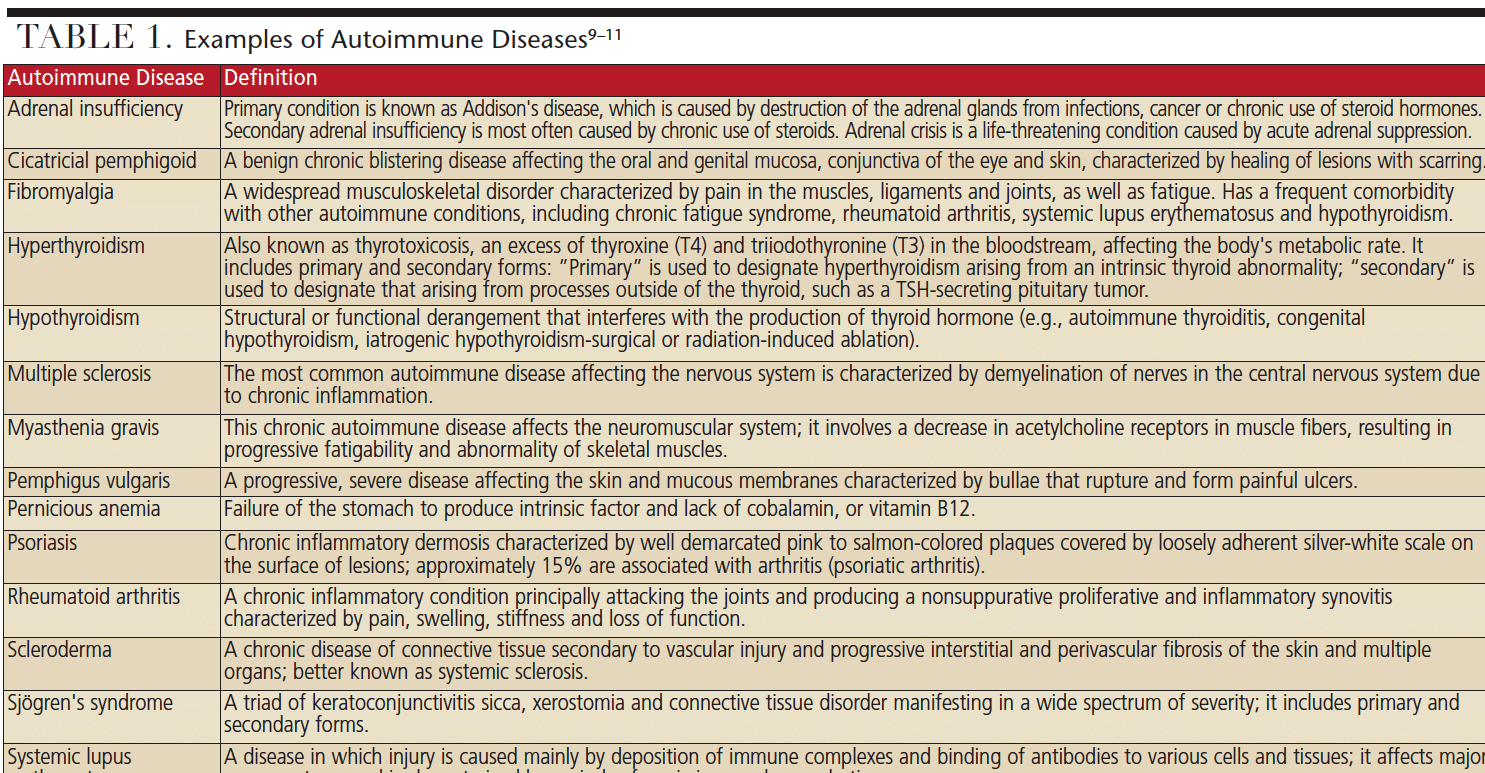
One of the common characteristics of autoimmune disease is that individuals often exhibit cluster disorders and will present with more than one autoimmune disease.8 Because autoantibodies can travel throughout the body, patients usually experience multisystem organ involvement that may not be easily explained or diagnosed. Among this patient population, signs and symptoms of multisystem organ involvement are nondescript, and often present as fatigue, joint pain, muscle aches, sleep disorders and anemia. Patients experience psychiatric difficulties, most commonly depression and frustration, as a consequence of consultations with multiple providers without receiving a definitive diagnoses or treatment recommendations. The result is that patients live with diminished quality of life and ongoing health challenges, including compromised oral health. Examples of autoimmune diseases appear in Table 1.9–11
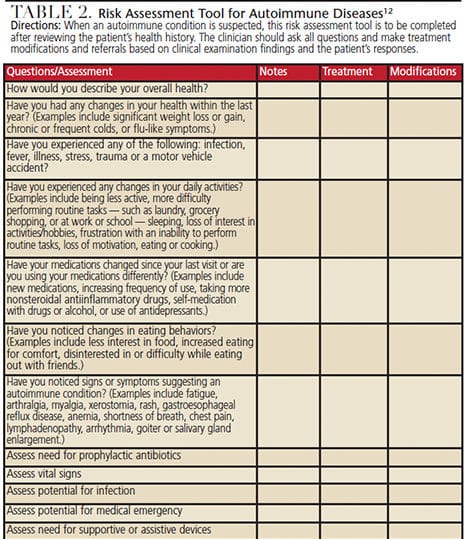
RISK ASSESSMENT AND CLINICAL CONSIDERATIONS
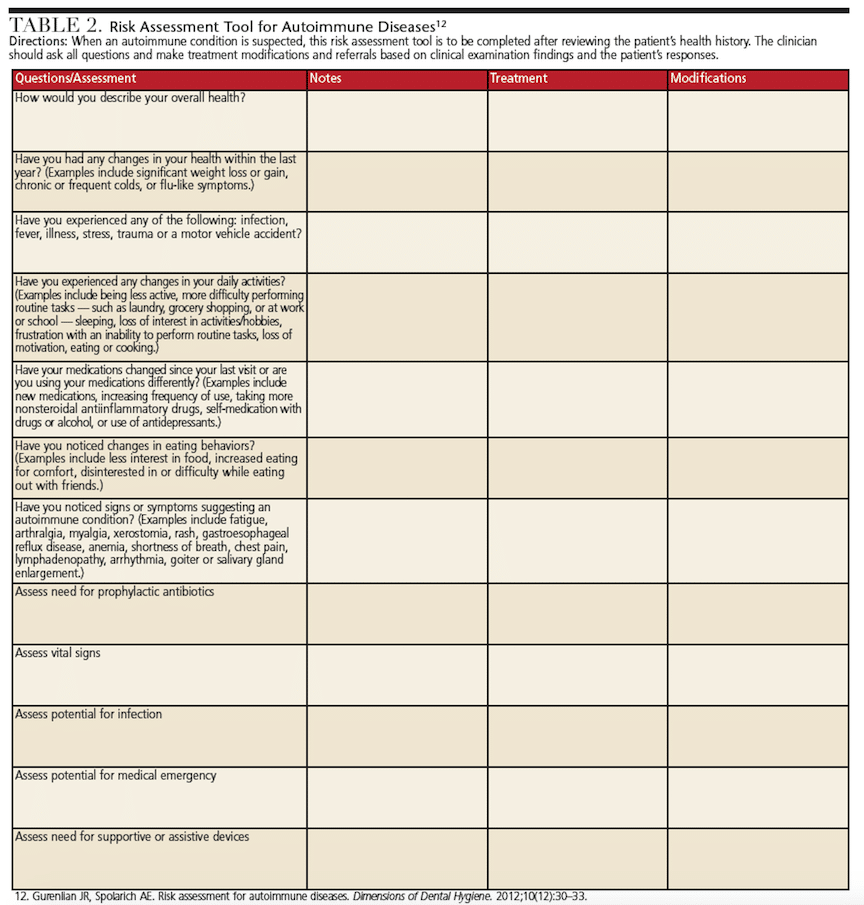
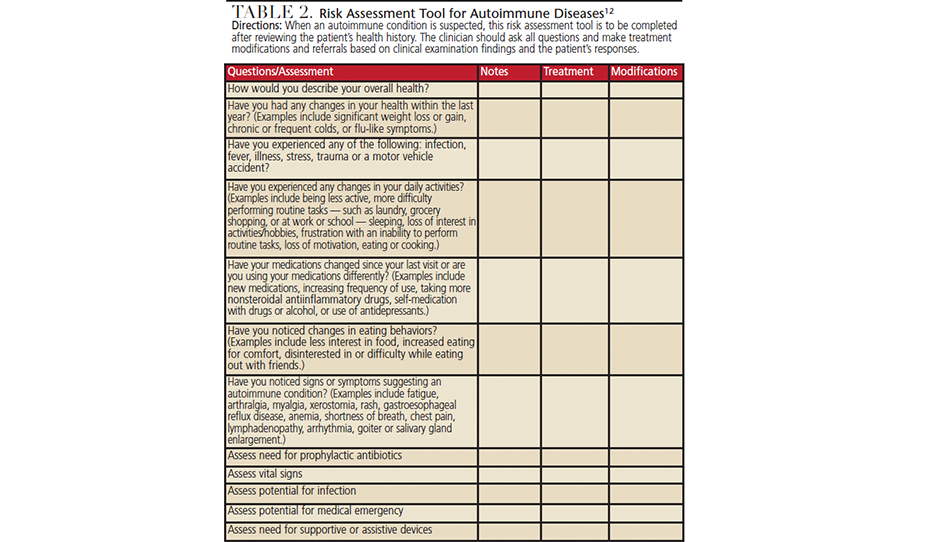
Dental professionals can engage in refined assessment for autoimmune diseases by taking a careful health history and using probing questions for manifestations of problems suggesting an autoimmune component. Table 2 presents a risk assessment tool that can aid clinical decision-making.12 Performing a thorough medical, oral and pharmacologic history review is critical to identify conditions that warrant further medical evaluation. Use of the risk assessment tool presented in Table 2 will assist in determining modifications for treatment. The clinician must determine if the need for medical care supersedes oral care, whether it is safe to provide treatment, and what the patient will be able to tolerate in terms of scheduling and procedures.
Given their relevance to overall patient care and dental treatment, vital signs should be taken on all patients. These include blood pressure, pulse, respiration, temperature, height and weight. Blood pressure may be elevated due to chronic pain. Medication-induced orthostatic hypotension may occur in patients taking antihypertensive medications, increasing the risk for falling.
Blood studies are performed due to these patients’ multisystem organ involvement and multiple medications that affect liver and kidney function. Further, patients are predisposed to infections when taking immunosuppressive drugs. Obtaining results of recent blood studies will help determine whether values are within normal limits and if adaptations to treatment are indicated. Frequency of testing is determined based upon patient complaints, signs and symptoms, and current disease status. A complete blood count with differential and a comprehensive metabolic panel are useful in assessing risks for infection, bleeding (platelets) and possible coagulopathies, and liver and kidney function.
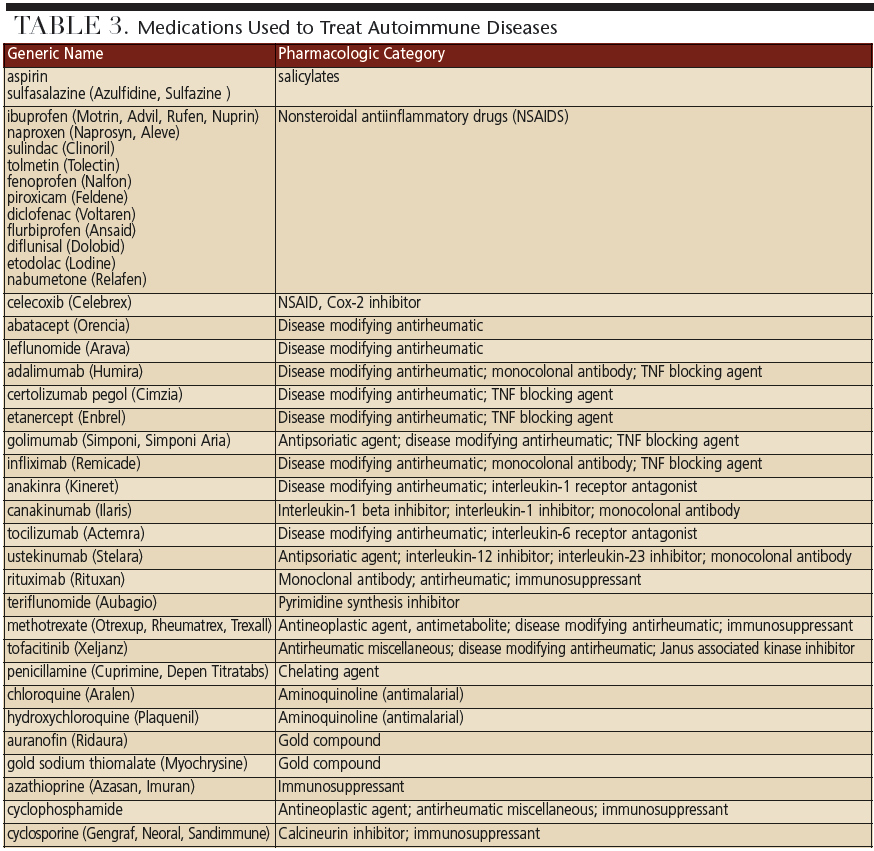
Most patients with autoimmune diseases who have prosthetic joints will not require antibiotic premedication. Clinicians should use the American Academy of Orthopedic Surgeons’ (AAOS) appropriate use criteria endorsed by the American Dental Association to determine the need for premedication.13,14 Note the AAOS has determined that patients with rheumatoid arthritis using biologic disease modifying agents, such as tumor necrosis factor alpha blockers or prednisone > 10 mg per day, are considered to be immunocompromised and premedication may be indicated.14 However, methotrexate and hydroxychloroquine (Plaquenil) are not considered to be immunocompromising agents.14 Clinicians are encouraged to download the AAOS AUC algorithm app for use with determining need for premedication.14
The extra- and intraoral examinations provide critical information about oral health status and function.15–18 Clinicians should assess the patient for signs of neuromuscular involvement, such as limited range of opening, paresthesias and numbness, drooping eyelids, and tremors of the lip, tongue or jaws. Neurological involvement may present as complaints of burning mouth or tongue. Patients may also demonstrate difficulty with speech and/or alterations in voice. Swallowing disorders increase risk for aspiration.
Careful attention should be paid to detection of oral lesions and diagnosis. Many mucosal disorders are autoimmune in nature, such as cicatricial pemphigoid, pemphigus vulgaris, pernicious anemia and systemic lupus erythematosus. Oral adverse events may be disease- and/or drug-related. Common oral conditions affecting this patient population include chronic xerostomia, recurrent caries, periodontal disease and fungal infections. Dental professionals are encouraged to conduct a careful caries risk assessment at each visit.
Many patients live with chronic pain and thus present with a history of regular use of analgesics, including opioids. Dentists should consult with the patient’s rheumatologist and/or pain management specialist before prescribing any additional analgesics. Pain management strategies must consider existing analgesic use, variations in patient response to pain, and possible need for modification of dosage. Epinephrine should be avoided in patients with untreated/uncontrolled hyperthyroidism.9,11 Topical anesthetics are beneficial adjuncts for managing oral mucosal disorders. Proper pain control is an essential component of a stress reduction protocol. Chronic steroid use to reduce inflammation and related joint damage increases risk for adrenal crisis, and good pain and anxiety control help reduce risk for this medical emergency.9,11 Steroid supplementation is rarely needed for routine dental procedures; however, this should be determined based on individual patient needs and type of procedure in consultation with the patient’s physician.9,11
Judicious planning will allow providers to manage the physical demands that may occur on patients who have limitations associated with autoimmune disease. For example, some patients may experience vision and mobility challenges. Therefore, common areas need to be free from obstructions that would hinder patient accessibility and safety. Dental teams should evaluate the office and surrounding areas for fall risk associated with both physical and cognitive impairments, as well as side effects of medications. In addition, short appointments may be advisable to accommodate patients with joint pain, stiffness, swelling, shortness of breath, or other manifestations that affect their ability to sit for long periods. Planned breaks and oral assistive devices should be discussed in advance so there is less stress for the patient and provider. In some cases, the clinician may need to consult with the patient’s physician so that oral care can occur in concert with medical treatment in a safe manner.
CONCLUDING THOUGHTS
Providing oral health education is a key component of care because patients need to understand the relationship between autoimmune disease, medical management and oral considerations. Clinicians should recommend products that will optimally manage biofilm, caries and xerostomia. Fluoride and nonfluoride remineralization products will be needed to reduce risk for caries and hypersensitivity; some patients may also benefit from the use of xylitol for additional caries risk reduction. Salivary stimulants and substitutes should be recommended for patients experiencing salivary hypofunction and xerostomia. Antimicrobials, such as chlorhexidine, essential oils, triclosan or cetylpyridinium chloride, may be indicated for oral disease risk reduction and oral malador. Use of power toothbrushes, oral irrigators or airfloss technology, along with interdental brushes, should be recommended for biofilm removal, oral cleansing and salivary stimulation.19–22
In addition, regular dexterity assessments and nutrition counseling are recommended to help determine if self-care goals are appropriate and realistic. Further, because some autoimmune diseases have oral lesions, teaching patients to perform an oral self-examination is valuable. Patients can communicate findings of these exams with their dental provider and seek immediate evaluation and treatment. Lastly, as disease progresses, some patients may require the assistance of a caregiver. Educating caregivers about how to provide daily oral care is critical to maintaining oral wellness.10,12
Individuals with autoimmune disease should be evaluated on a regular basis.10 Frequent recare appointments are warranted, and two- to three-month intervals may be advisable to assess oral disease state, provide further treatment and reinforce self-care regimens. More frequent visits allow clinicians to monitor general health status and maintain communication with other health care providers. Interprofessional collaborations include registered dieticians, physical and occupational therapists and dermatologists. Rheumatologists are typically the point of care contact for all questions regarding patient management.
Patients affected by autoimmune diseases are medically complex and present numerous challenges. Use of the proposed risk assessment model can assist the clinician with decision-making. Careful analysis of systemic and oral health considerations helps ensure that comprehensive dental care can be delivered safely to improve the oral health of this patient population.
REFERENCES
- American Autoimmune Related Diseases Association Inc. AARDA Facts. Available at: aarda.org. Accessed September 1, 2017.
- U.S. National Library of Medicine National Institutes of Health: Autoimmune disorders. Available at: medlineplus.gov/ency/article/000816.htm. Accessed September 1, 2017.
- Abbas AK, Lichtman AH, Pallai S. Basic Immunology: Functions and Disorders of the Immune System. 3rd ed. Philadelphia: Elsevier Saunders; 2011.
- Kumar V, Abbas AK, Aster JC. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Philadelphia: Elsevier Saunders; 2015.
- Laxminarayana D. Is tolerance broken in autoimmunity? Clin Med Insights Pathol. 2017;10:1–5.
- Watad A, Azrielant S, Bragazzi NL, et al. Seasonality and autoimmune diseases: the contribution of the four seasons to the mosaic of autoimmunity. J Autoimmun. 2017;82:13–30.
- Lin J, Liu J, Davies ML, Chen W. Serum vitamin D level and rheumatoid arthritis disease activity: review and meta-analysis. PLOS One. 2016;11:e0146351.
- Cárdenas-Roldán J, Rojas-Villarraga A, Anaya JM. How do autoimmune diseases cluster in families? A systematic review and meta-analysis. BMC Med. 2013;11:73.
- DeRossi SS, Ciarrocca KN. Autoimmune and Connective Tissue Diseases. In: Patton LL, Glick M, eds. The ADA Practical Guide to Patients With Medical Conditions. 2nd ed. Hoboken: Wiley Blackwell; 2016:201–230.
- Gurenlian JR, Spolarich AE. Persons with Autoimmune Diseases. In: Darby ML, Walsh MM, eds. Dental Hygiene Theory and Practice. 4th edition. St Louis: Elsevier Saunders; 2015:891.
- Little JW, Falace DA, Miller CS, Rhodus, NL. Dental Management of the Medically Compromised Patient. 8th ed. St Louis: Elsevier Mosby; 2013.
- Gurenlian JR, Spolarich AE. Risk assessment for autoimmune diseases. Dimensions of Dental Hygiene. 2012;10(12):30–33.
- American Dental Association —Appointed Members of the Expert Writing and Voting Panels Contributing to the Development of American Academy of Orthopedic Surgeons Appropriate Use Criteria. American Dental Association guidance for utilizing appropriate use criteria in the management of the care of patients with orthopedic implants undergoing dental procedures. J Am Dent Assoc. 2017;148:57–59.
- American Academy of Orthopedic Surgeons. Ortho guidelines. Appropriate use criteria: Management of patients with orthopaedic implants undergoing dental procedures. Available at: www.orthoguidelines.org/go/auc/default.cfm?auc_id=224995&actionxm=Terms. Accessed September 1, 2017.
- Magliocca KR, Fitzpatrick SG. Autoimmune disease manifestations in the oral cavity. Surg Pathol Clin. 2017;10:57–88.
- Mustafa MB, Porter SR, Smoller BR, Sitaru C. Oral mucosal manifestations of autoimmune skin diseases. Autoimmun Rev. 2015;14:930–951.
- Bascones-Martínez A, García-García V, Meurman JH, Requena-Caballero L. Immune-mediated diseases: what can be found in the oral cavity? Int J Dermatol. 2015;54:258–270.
- Abrão AL, Santana CM, Bezerra AC, et al. What rheumatologists should know about orofacial manifestations of autoimmune rheumatic diseases. Rev Bras Reumatol Engl Ed. 2016;56:441–450.
- Starke M, Delaurenti M, Ward M, Souza S, Milleman KR, Milleman JL. A comparison of the effect of two power toothbrushes on the gingival health and plaque status of subjects with moderate gingivitis. J Clin Dent. 2017;28(1 Spec No A):A29–A35.
- Mwatha A, Olson M, Souza S, et al. Gingival health and plaque regrowth response following a four-week interdental hygiene intervention. J Clin Dent. 2017;28(1 Spec Iss A):A36–A44.
- de Jager M, Rmaile A, Darch O, Bikker JW. The effectiveness of manual versus high-frequency, high-amplitude sonic powered toothbrushes for oral health: a meta-analysis. J Clin Dent. 2017;28(1 Spec Iss A):A13–A28.
- Papas A, Singh M, Harrington D, et al. Stimulation of salivary flow with a powered toothbrush in a xerostomic population. Spec Care Dentist. 2006;26:241–246.
Featured image by LIGHTFIELDSTUDIOS/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. October 2017;3(10):45–48.


{kind=link}
{kind=link}
{kind=link}
{kind=link}