

Dentists’ Role in Interprofessional Education and Practice
As the silo model of health care fades, oral health professionals will play an increasingly important part in efforts that ensure comprehensive interprofessional care.
As the silo model of health care fades, oral health professionals will play an increasingly important part in efforts that ensure comprehensive interprofessional care
PURCHASE COURSE
This course was published in the August 2018 issue and expires August 2021. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
As science continues to identify links between oral and systemic health, compartmentalization of dental and medical care appears to be fading — which, in turn, is driving the paradigm shift toward interprofessional education and practice. The call to action in Oral Health in America: A Report of the Surgeon General in 2000 increased interest in examining the potential causality of oral disease and systemic conditions.1 An aging population, increased longevity and chronic health conditions place growing demands on interprofessional care teams that provide medical, dental and social services.2 The most recent Surgeon General’s report focuses on the challenges associated with unprecedented levels of substance abuse, including tobacco, alcohol and opioids, which directly and indirectly impact oral health.3 Like those before it, the report calls for coordinated care and prevention strategies, and strongly speaks to prevention through safe prescribing of controlled substances and use of alternative approaches to manage pain and anxiety. Dentistry is directly involved in these specific strategies, and joins the extended professional community in increasing prescription drug monitoring programs.3
This course was published in the August 2018 issue and expires August 2021. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the concept of team-based patient management, and factors behind the paradigm switch to interprofessional education and practice.
- Explain models of interprofessional education and the benefits of a collaborative approach to practice.
- Discuss the clinical strategies and skills that are essential to the success of multidisciplinary, team-based care.
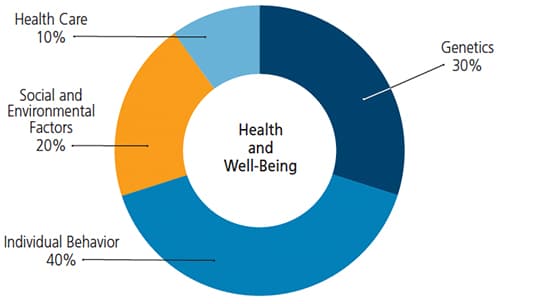
There exists a growing awareness that, in addition to the clinical factors with which the dental profession is highly familiar, social factors have a significant influence on oral disease and care outcomes. The U.S. Centers for Disease Control and Prevention recognizes the following determinants of health as especially impactful:
- Biology and genetics (examples: sex and age)
- Individual behavior (examples: alcohol, injected drug use, unprotected sex and smoking)
- Social environment (examples: discrimination, income and gender)
- Physical environment (examples: where a person lives and/or crowding)
- Health services (examples: access to quality health care and health insurance).4
Additionally, the effects of health literacy (a person’s capacity for obtaining and understanding basic health information) and ability to navigate complex health care systems are becoming more fully recognized.5 In similar fashion, individuals vary in their ability to apply reading, listening, analysis and decision-making skills to health care decisions.5
Finally, in its 2016 definition of oral health, the FDI World Dental Federation recognized that it is a fundamental component of physical health and mental well-being. “Influenced by the values and attitudes of individuals and communities, [it] reflects the physiological, social and psychological attributes that are essential to quality of life.”6 Compared to other factors influencing health and wellness, recognizing the importance of oral health care points to the fact that historical models of care — restorative dental interventions — may not yield the disease prevention, risk reduction and long-term outcomes that patients and providers desire (Figure 1).7
INTERPROFESSIONAL EDUCATION AND TEAM-BASED CARE
To address these multifactorial etiologies, the health care profession has demonstrated a growing commitment to the Institute for Healthcare Improvement’s Triple Aim framework. The goal is threefold: to improve the patient’s experience during care, improve the health of various populations, and reduce the per capita cost of health care.2 Grounded in evidence-based practice, quality improvement, technology and outcome assessment, Triple Aim goals may best be accomplished through IPE and comprehensive patient care.8
Comprehensive care is an approach that addresses the totality of the patient’s needs (i.e., physical and emotional health), and thus requires coordination among the extended health care team.9 As part of these efforts, representatives from dentistry, nursing, medicine, osteopathic medicine, pharmacy and public health convened to develop core competencies that would shape and support IPE and interprofessional care. Supported by the nongovernment, nonprofit Health and Medicine Division of The National Academies of Sciences, Engineering, and Medicine (formerly the Institute of Medicine), the goal was to “prepare future health professionals for enhanced, team-based care and improved outcomes.” The work of this group culminated with the publication of Core Competencies for Interprofessional Collaborative Practice.10 Updated in 2016, these competencies were brought into four topical areas under the single domain of interprofessional collaboration, and further defined as:11
- Competency 1: Work with individuals of other professions to maintain a climate of mutual respect and shared values.
- Competency 2: Use the knowledge of one’s own role and those of other professions to appropriately assess and address the health care needs of patients and promote and advance the health of populations.
- Competency 3: Communicate with patients, families, communities, and professionals in health and other fields in a responsive and responsible manner that supports a team approach to the promotion and maintenance of health, and the prevention and treatment of disease.
- Competency 4: Apply relationship-building values and the principles of team dynamics to effectively plan, deliver and evaluate patient/population-centered care, and population health programs and policies that are safe, timely, efficient, effective and equitable.11
According to the World Health Organization (WHO) definition, IPE occurs “when students from two or more professions learn about, of, and between themselves to allow an effective collaboration.”8 Underscoring the importance of these concepts, oral health, medicine, nursing, physical therapy and pharmacy programs include IPE among their standards for accreditation.12 The goal of this emerging interprofessional collaborative practice paradigm, WHO asserts, is for “multiple health workers from different professional backgrounds to provide comprehensive services by working with patients, their families, caregivers and communities to deliver the highest quality of care across settings.”8 The Affordable Care Act, which includes dental benefits for children, frequently alludes to such team-based interprofessional care and organizational models aligning to provide coordinated patient care and improved outcomes.13
DENTISTRY’S RESPONSE
Dental educators have responded to meet the goals of interprofessional education and practice. In 2016, the American Dental Association Commission on Dental Accreditation for Dental Education Programs revised standards to require graduates to be “competent in communicating and collaborating with other members of the health care team to support comprehensive patient care.”14 By 2014, 69% of dental schools required IPE offerings for dental students, with the three most common partners noted as pharmacy, nursing and medicine.15 By 2015, approximately 90% of dental schools offered some form of formal IPE coursework for students, and 75% of dental schools in the study also provided training for faculty.15 Medicine has responded similarly by offering oral-systemic training for medical students.16
Models of IPE include development and implementation of prenatal patient screening, education and referral — including conversations about the safety of dental treatment for pregnant patients — in a team-based, medical-dental clinical setting.17 Another example of collaborative practice matched oral health and pharmacy students to examine chronic conditions, such as hypertension, diabetes and polypharmacy, to address existing primary care needs that might otherwise go unmet in a dental setting.18
Interdisciplinary teams are common in the care of patients with head and neck cancers and cleft craniofacial conditions. Such teams rely on the partnership of radiation oncology, pediatrics, internal medicine, social work, otolaryngology and medical oncology. Together, the American Cleft Palate-Craniofacial Association and Cleft Palate Foundation have developed recommended, voluntary expectations for establishment and approval of these functional teams. The six components they note as essential to a strong, coordinated process are generic, and might be considered when building any number of interprofessional collaborative practice relationships. These include team composition, team management and responsibilities; patient and family/caregiver communication; cultural competence; psychological and social services; and outcomes.19 Management of chronic, recurrent and medically related disease of the oral cavity and maxillofacial region also relies on a medical-dental team approach.20
As evidenced by joint efforts, such as the 2014 Conference on Interprofessional Education and Practice — convened by the California Dental Association and American Dental Education Association (ADEA) — the dental profession is lending support to interprofessional education and practice.21 During the meeting, one panelist, Richard W. Valachovic, DMD, MPH, president and CEO of ADEA, characterized the trend of interprofessional care as “not just minor revisions of the rules … but a systemic change in the culture of health care education and practice.”22
The American Academy of Pediatrics is an advocate for partnerships between pediatric medical and dental homes, and supports pediatricians incorporating oral health assessments and education into well-child examinations.23 Training tools to assist this collaborative network of oral health services are beginning to appear. For example, the National Interprofessional Initiatives on Oral Health is a consortium of funders and health care professionals that is focused on the training and collaboration of family medicine, pediatrics, obstetrics and internal medicine to reduce dental disease. Nondental providers can access a web-based curriculum that provides information about oral health topics and behavior modification.24
One of the most recent examples of interprofessional synergy is a proposal by the American Cardiology Association to the American Medical Association to promote and support legislative action to include preventive and therapeutic dental services as a standard benefit for all Medicare recipients.25 Currently, Medicare covers dental services that are an essential part of a medical procedure — such as surgery related to trauma or pathology. Routine dental services, including examinations and preventive or restorative care, are not covered.26 Considering that 42% of individual in the U.S. age 65 and older made at least one dental visit between 2000 to 2013 — along with projections the geriatric population will double to 92 million by 2060 — any additional coverage for patients in this population stands to have a significant impact on oral health care utilization.27,28
CURRENT EXAMPLES OF INTEGRATED SYSTEMS OF CARE
Organizations demonstrating successful systems of comprehensive care include Kaiser Permanente, HealthPartners, and Programs for All-Inclusive Care for the Elderly (PACE). Kaiser’s Permanente Dental Associates is a corporation of shareholder dentists who, through a shared electronic health record, are able to identify “care gaps” and alert patients of overdue and pending needs — including routine screenings and vaccinations.29 HealthPartners is a collaborative organization of medical, dental and pharmacy professionals that includes multiple hospitals and a trauma center. In addition to providing team-based care, HealthPartners Dental Group participates in practical research through the National Dental Practice-Based Research Network.30,31 Each of these systems-based approaches to care involves performance and quality metrics. Included in these metrics is total cost-of-care, which attempts to confirm positive health outcomes at reduced cost — and with greater patient satisfaction.29
Finally, the primary goal of PACE, a national system of community-based programs that offers long-term care for the frail, elderly and individuals with disabilities, is to help this patient population delay or avoid placement in a nursing home. PACE programs offer medical and dental care, physical therapy, occupational therapy, dietary guidance and recreational therapy, along with specialty medical and social services. All are provided through a coordinated, team-based approach in the home, community and PACE centers, reducing more costly use of inpatient hospital and nursing home services.32
IMPLEMENTATION CHALLENGES
Although more recent dental graduates are likely familiar with interprofessional care, clinicians accustomed to the autonomy associated with private practice may find transition to this model more challenging. Increased communication skills may be needed to motivate patients — especially individuals with low oral health literacy — to make the behavioral changes necessary for collaborative care to succeed. At the same time, providers must heed regulatory constraints and legal issues regarding scope of practice.
While the lack of platforms for sharing electronic health records hinders efficient communication at this time, shared medical and dental records are beginning to emerge. Such technology allows a variety of health care providers to serve patients more effectively and efficiently, and discover preventive and therapeutic approaches that may lead to improved oral-systemic disease management.33 An additional barrier may be dentistry’s procedure-based compensation model, which differs significantly from the medical model of care based on preventive and management approaches to disease. Value-based payment systems, which are becoming more common in medicine, reward providers for patient health and may incentivize collaborative care models. However, this compensation model has been slower to gain traction in dentistry.34
SUMMARY
Ranking among the most significant changes to health care education and delivery in the 21st century, interprofessional education and practice rely on a new model of collaborative care.34 Fostering a team-based approach is expected to positively influence the patient experience, improve oral and systemic health care outcomes, and reduce the cost of care — making it a worthwhile commitment for the educational and practicing communities. Through optimized expertise, interprofessional care teams may help achieve more inclusive, comprehensive and patient-centered care that promises to improve access, and minimize the number of patients who “fall through the cracks” as a result of numerous referrals.35 Working across disciplines, oral health care providers will bring unique insights and value to multidisciplinary teams. Under this new paradigm of care, the interprofessional education and practice communities must continue to break down traditional silo settings so as to serve patients in more sustainable and cost-effective ways that will improve prevention and treatment of oral and systemic diseases.
REFERENCES
- National Institute of Dental and Craniofacial Research. Oral Health in America: A report of the Surgeon General (Executive Summary). Available at: www.nidcr.nih.gov/research/data-statistics/surgeon-general. Accessed July 10, 2018.
- Institute for Healthcare Improvement. IHI Triple Aim Initiative. Available at: www.ihi.org/Engage/Initiatives/TripleAim/Pages/default.aspx. Accessed July 10, 2018.
- U.S. Department of Health and Human Services Office of the Surgeon General. Facing Addiction in America: The Surgeon General’s Report on Alcohol, Drugs, and Health. Available at: https://addiction.surgeongeneral.gov/. Accessed July 10, 2018.
- The National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. NCHHSTP Social Determinants of Health. Available at: www.cdc.gov/nchhstp/socialdeterminants/definitions.html. Accessed July 10, 2018.
- Office of Disease Prevention and Health Promotion. Determinants of Health. Available at: www.healthypeople.gov/2020/about/foundation-health-measures/Determinants-of-Health. Accessed July 10, 2018.
- Glick M, Williams DM, Kleinman DV, Vujicic M, Watt RG, Weyant RJ. A new definition for oral health developed by the FDI World Dental Federation opens the door to a universal definition of oral health. J Am Dent Assoc. 2016;147:915–917.
- Schroeder SA. We can do better — Improving the health of the American people. N Engl J Med. 2007;357:1221–1228.
- World Health Organization. Framework for action on interprofessional education and collaborative practice. Available at: www.who.int/hrh/resources/framework_action/en/. Accessed July 10, 2018.
- American Academy of Family Physicians. Comprehensive Care, Definition of. Available at: www.aafp.org/about/policies/all/care-definition.html. Accessed July 10, 2018.
- Interprofessional Education Collaborative. Core Competencies for Interprofessional Collaborative Practice: Report of an Expert Panel. Available at: www.aacom.org/docs/default-source/insideome/ccrpt05-10-11.pdf?sfvrsn=77937f97_2. Accessed July 10, 2018.
- Interprofessional Education Collaborative. Core Competencies for Interprofessional Collaborative Practice: 2016 update. Available at: https://hsc.unm.edu/ipe/resources/ipec-2016-core-competencies.pdf. Accessed July 10, 2018.
- University of Connecticut. Current IPEH Accreditation Standards. Available at: interprofessional.uconn.edu/current-ipe-accreditation-standards-health-professions-programs/. Accessed July 10, 2018.
- Affordable Care Act and Oral Health: ADA analysis of impact. Available at: https://ebusiness.ada.org/assets/docs/2256.PDF?OrderID=1752119. Accessed July 10, 2018.
- Commission on Dental Accreditation. Accreditation Standards for Dental Education Programs. Available at: www.ada.org/~/media/CODA/Files/pde.pdf?la=en. Accessed July 10, 2018.
- Palatta A, Cook BJ, Anderson EL, Valachovic RW. 20 Years beyond the crossroads: The path to interprofessional education at U.S. dental schools. J Dent Edu. 2015;79:982–996.
- Association of American Medical Colleges. Report IX, Contemporary Issues in Medicine: Oral Health Education for Medical and Dental Students. Available at: https://members.aamc.org/eweb/upload/Contemporary%20Issues%20in%20Med%20Oral%20Health%20Report IX.pdf. Accessed July 10, 2018.
- Leone SM, Quinonez RB, Chuang A, Begue A, Kerns A, Jackson J, Phillips C. Introduction of prenatal oral health into medical students‘ obstetrics training. J Dent Edu. 2017;8:1405–1412.
- Branch-Mays GL, Pittenger AL, Williamson K, Milone A, Hein E, Thiere T. An interprofessional education and collaborative practice model for dentistry and pharmacy. J Dent Edu. 2017;81:1413–1420.
- American Cleft Palate-Craniofacial Association. Standards of Approval for Team Care. Available at: http://acpa-cpf.org/team-care/standardscat/standards-of-approval-for-team-care/. Accessed July 10, 2018
- American Academy of Oral Medicine. Available at: www.aaom.com/mission-and-vision. Accessed July 10, 2018.
- California Dental Association. Conference on Interprofessional Education and Practice: Creating a Vision for the Dentist of the Future. Available at: www.cda.org/portals/0/pdfs/i_ep_conf_reg_brochure.pdf. Accessed July 10, 2018.
- Valachovic RW. Building a foundation for interprofessional education practice. Keynote address: Integrating oral and overall health care: On the road to interprofessional education and practice. J Calif Dent Assoc. 2014;42:25–27.
- Norwood KW, Slayton RL, Council on Children With Disabilities, Section on Oral Health. Oral health care for children with developmental disabilities. Pediatrics. 2013;131:614–619.
- Smiles for Life. Learn online. Available at: www.smilesforlifeoralhealth.org/buildcontent.aspx?pagekey=101554&lastpagekey=62948&userkey=13892385&sessionkey=4187155&tut=555&customerkey=84&custsitegroupkey=0. Accessed July 10, 2018.
- American Medical Association. House of Delegates Handbook. Resolution 111 (A-18). Available at: www.ama-assn.org/sites/default/files/media-browser/public/hod/a18-handbook-combined.pdf. Accessed July 10, 2018.
- Medicare Interactive. Medicare and Dental Care. Available at: www.medicareinteractive.org/get-answers/medicare-covered-services/limited-medicare-coverage-vision-and-dental/medicare-and-dental-care. Accessed July 10, 2018.
- Nasseh K, Vujicic M. American Dental Association Health Policy Institute Research Brief. Available at: www.ada.org/~/media/ADA/Science%20and%20Research/HPI/Files/HPIBrief_1015_1.pdf. Accessed July 10, 2018.
- Deringer J, Phipps K, Carsel B. Critical Trends Affecting the Future of Dentistry; Assessing the Shifting Landscape. Available at: www.ada.org/~/media/ADA/Member%20Center/FIles/Escan2013_Diringer_Full.ashx. Accessed July 10, 2018.
- Jones JA, Snyder JJ, Gesko DS, Helgeson MJ. Integrated medical-dental delivery systems: models in a changing environment and their implications for dental education. J Dent Educ. 2017;81:eS21–eS29.
- Health Partners. Available at: www.healthpartners.com/hp/index.html. Accessed July 10, 2018.
- Norton WE, Funkhouser E, Makhija SK, et al. Concordance between clinical practice and published evidence: findings from the National Dental Practice-Based Research Network. J Am Dent Assoc. 2014;145:22–31.
- Chávez EM, Hendre A. Caring for older adults with complex needs: drafting an interdisciplinary team. J Calif Dent Assoc. 2015;43:597–604.
- Hostetter M, Klein S. In Focus: Integrating Oral Health into Primary Care. Available at: www.commonwealthfund.org/publications/newsletters/quality-matters/2015/february-march/in-focus. Accessed July 10, 2018.
- Cole JR, Dodge WW, Findley JS, et al. Interprofessional collaborative practice: how could dentistry participate. J Dent Educ. 2018:82:441–445.
- Mowat S, Hein C, Walsh T, MacDonald L, Grymonpre R, Sisler S. Changing health professionals’ attitudes and practice behaviors through interprofessional continuing education in oral-systemic health. J Den Educ. 2017;81:142–1429.
Featured image by SKYNESHER/E+/GETTY IMAGES PLUS
From Decisions in Dentistry. August 2018;4(8):30–32,35.


[…] This course intends to teach students how to effectively communicate with patients and members of the extended health care team to foster a team-based approach. […]