
 ODEBALA/E+/GETTY IMAGES PLUS
ODEBALA/E+/GETTY IMAGES PLUS
Treating Adolescents With Major Depressive Disorder
With training and empathy, oral health professionals can provide quality care for adolescent patients with major depressive disorder.
PURCHASE COURSE
This course was published in the March 2021 issue and expires March 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the March 2021 issue and expires March 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the prevalence and rates of severe impairment of major depressive disorder (MDD) in adolescents, and the effects of depression on daily activities and oral health.
- Explain common symptoms of MDD in this patient population, risk factors, and the role of screening in dental settings.
- Discuss clinical tools, techniques and treatments dental teams can use in support of adolescent patients with MDD.
Adolescence is shaped by biological, cognitive and social processes.1 Healthy adolescent development is characterized by an increased self-awareness, satisfaction, growth and resilience.1 This period represents a critical phase in exploration and risk-taking behaviors, formation of peer relationships, changes in family relationships, and development of identity and self-direction.1 Stress, hormones, unlearned resilience, and other challenges are why adolescents are vulnerable to depression and anxiety.1
Depression is one of the leading causes of illness and disability among adolescents worldwide.2 In 2017, the National Institute of Mental Health reported 3.2 million adolescents ages 12 to 17 had suffered at least one major depressive episode, noting a higher prevalence for females (20%, compared to males at 6.8%), and those with mixed-race/ethnicity (16.9%).2 Approximately 71% of this adolescent population that experienced a major depressive episode had severe impairment.2 Major depressive disorder (MDD) affects all aspects of an adolescent’s life, including diet, exercise and oral hygiene habits — all of which impact risk for oral disease.3–6
With training and empathy, dental professionals can provide quality care to adolescents with MDD. Understanding and support of these patients can reduce dental-related stress and anxiety, thus helping the patient and extended care team manage this disorder.5,6 A trusting patient-provider relationship is necessary for compliance of self-care recommendations and adherence to regular dental visits.6 This paper will provide an overview of the complexity of adolescent depression, its effect on oral health, and the key role dental teams play in supporting positive oral and behavioral health outcomes.
WHAT IS MAJOR DEPRESSIVE DISORDER?
This condition is defined by the Diagnostic and Statistical Manual of Mental Disorders-5 as five or more of the following symptoms presenting during a two-week period, along with either a depressed mood or loss of interest or pleasure.7 These symptoms tend to occur most of the day, nearly every day, with the most common symptoms being:7
- Significant weight loss or gain
- Insomnia or hypersomnia
- Psychomotor agitation or retardation
- Feelings of worthlessness or guilt
- Fatigue or loss of energy
- Inability to think or concentrate; indecisiveness
- Thoughts of death or suicide
In adolescents, MDD affects physical, emotional and social development,8 as well as school, family and social relationships.9 Inhibitory processes and deficits include the inability to control and stabilize negative moods with positive and rewarding stimuli.10,11 Patients with MDD may also have feelings of hopelessness and boredom, and experience changes in sleep patterns.8
Common risk factors include a family history of depression, trauma, abuse, neglect, parental conflict, inadequate peer relationships, poor academic performance, substance use/abuse, negative thinking, and deficits in coping skills.8,9 No specific gene has been identified in causing MDD; however, research has shown that genomic biomarkers can help identify patients who are most susceptible to depression.12 Additionally, low levels of three major neurotransmitters — dopamine, norepinephrine and serotonin — have been linked to MDD.12
Even as the most common mental health disorder among adolescents,13 depression is under-recognized and underdiagnosed.8,14 When left untreated, it can lead to substance use, criminality, suicide15 and mental health illness in adulthood.9,16 While suicide is the second leading cause of death among adolescents and young adults ages 15 to 24,13 research shows less than 20% of adolescents receive care from a health professional after a major depressive episode — and an even smaller percentage receive a combination of medication therapy and professional treatment.2 The growing number of untreated adolescents suggests a widening mental health treatment gap17 that may contribute to prevalence rates and negative outcomes.
SCREENING FOR DEPRESSION
Although there is limited research on the effectiveness of depression screenings by dental professionals, the U.S. Preventive Services Task Force (USPSTF) recommends primary care physicians screen for depression among adolescents ages 12 to 18.9 Further, adequate systems must be in place to ensure accurate diagnosis, effective treatment, and appropriate follow-up.9 Oral health professionals are in a unique position to screen adolescents for depression since preventive dental visits often occur twice a year, and more frequently if the patient is undergoing orthodontic treatment. According to a National Health Interview Survey, approximately 73% of children ages 12 to 17 visited a dentist within six months of being surveyed.18
Developing a multidisciplinary relationship with the patient’s pediatrician and mental health provider is important when caring for patients with MDD.5,9 Depression screening can be used effectively in the dental office when referrals for mental health services for diagnosis and treatment are readily available.9 The USPSTF recommends depression screenings for all adolescents, and especially those at high risk for MDD, as identified through common risk factors. A comprehensive patient history allows the dental team to identify risk factors, including sociodemographic influences (e.g., age: adolescent, gender: female, race/ethnicity: minorities, parental income: lower income, and/or public insurance).8,9 Depression is more likely to be a comorbid condition when a patient has other chronic medical conditions.5–7 Therefore, the initial health history interview is critical to providing quality care.6
SCREENING TOOLS
Multiple depression screening tools are available to dental professionals. Two tools that have been researched most often for adolescents are the Patient Health Questionnaire for Adolescents (PHQ-A) and the primary care version of the Beck Depression Inventory.9 The latter can be self-scored, while the PHQ-A provides a scoring system. Both are valid and reliable.19,20 In addition, researchers have found that asking these questions verbally, rather than in written form, is more effective in identifying patients with depression.21
The PHQ-A is an adolescent modified version of the PHQ-9, a nine-question depression scale.22 While the PHQ-A is easy to use,20,23 the inclusion of a question about suicidal thoughts is a powerful instrument to assess feelings of hopelessness, which are a symptom of MDD in adolescents and a characteristic of suicidal thoughts.24 Johnson et al20 reported that adolescents with a PHQ-A diagnosis expressed significantly impaired mental functioning, as well as more physical pain and poorer overall health compared to those without an MDD diagnosis.
ORAL HEALTH IMPLICATIONS
Besides using the PHQ-A for screening in dental settings, additional circumstances may suggest a referral to the patient’s primary care provider for further examination. These include extreme fear of dental treatment, sleep bruxism and/or temporomandibular joint pain, extensive decayed, missing, or abfracted teeth, chronic medical condition(s), unexplained dissatisfaction with the appearance of teeth, intermittent pain of unknown origin, or poor oral hygiene inconsistent with overall appearance.5 Furthermore, a causative relationship was identified through poor diet, physical inactivity, obesity, smoking, poor oral health, sleep, and vitamin D deficiency.3,4 Some researchers recommend dental providers adopt a more relevant role in the treatment of patients with MDD.4–6 Toward this goal, dental teams can be trained to understand and support patients with MDD. Moreover, they can monitor medication adherence, implement dental treatment strategies, and identify the oral health implications of MDD, including adverse effects of antidepressants, potential drug interactions, and the correct dose of local anesthesia with vasoconstrictors.6
Mental health has a direct relationship with oral health status and outcomes.4 Compared to the general population, adolescents with MDD have a greater risk of oral health issues stemming from poor oral hygiene, unhealthy eating habits, and comorbid conditions, such as substance misuse, emotional stress and trauma.4,5,8,9 Maida et al25 studied adolescent perceptions of oral health, including self-image and the effect on social relationships. Adolescent beliefs and attitudes toward oral health are viewed in terms of social interaction, friendship and personal appearance; in addition, oral health is seen as important for their chances of succeeding in life.25
Gungormus and Erciyas26 found evidence of an association between bruxing and higher levels of self-reported anxiety and/or depression, especially in patients with temporomandibular disorder. While bruxism is more common in patients with depression and/or anxiety, antidepressants — such as selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors — often cause bruxing and jaw pain as side effects.27 Patients experiencing these effects from antidepressant therapy may be treated with a substitute medication, dose reduction, or cessation of antidepressant medication in concert with alternate psychotherapy.27 Antidepressant medications also affect salivary flow, inducing xerostomia and increasing the risk for caries.4,5
Additionally, adolescents with depression are at an increased risk of developing periodontal conditions.5,6 This relationship is based on biological (e.g., host immune response and inflammation), behavioral and psychosocial factors.3,5,28 Researchers have proposed that stress and depression may modify the host immune response, which, in turn, increases susceptibility to periodontal disease.3,28 Further, individuals who experience depression and stress may have elevated inflammatory markers; for example, treatment with antidepressants, particularly selective serotonin reuptake inhibitors, decreases the production of pro-inflammatory cytokines (such as tumor necrosis factor-α and interleukin-1), potentially affecting periodontal tissues.3 In fact, Okoro et al29 reported findings of an epidemiological study that showed adults with depression were less likely to seek oral healthcare and more likely to experience tooth loss than controls.
Therefore, oral health professionals should work closely with adolescents who present with depression (or symptoms of depression) to create a treatment plan to address periodontal health. A clinical guide for treating adolescent patients with MDD should consider:4–6
- The symptoms of MDD and medications used to treat it, as well as side effects (including interactions with local anesthetics).
- The complete medical history, including past and present mental health conditions, medications, and contact information for the patient’s primary care physician.
- Consulting with other members of the comprehensive care team to identify patients who might need special management (e.g., mental health referral).
- Being empathetic, respectful and nonjudgmental of the patient’s mental health condition.
- Keeping appointments short and using positive reinforcement. Clinicians should be willing to adapt, allowing the patient autonomy to choose how much can be accomplished at any given appointment.
- Completing the initial intake and assessment of the patients’ oral health needs, developing a treatment plan, and educating patients and caregivers about the possible side effects of antidepressant medications, and the impact of diet on oral and systemic health (i.e., nutritional counseling).
- Scheduling more frequent continuing care visits to reinforce oral health behaviors and monitor the progression of oral conditions.
- Helping the patient set realistic and achievable oral health goals.
- Using caution when recommending or prescribing nonsteroidal anti-inflammatory drugs or analgesics (such as hydrocodone, oxycodone, or tramadol) due to the increased risk of self-harm and possible interactions with antidepressants.
COGNITIVE BEHAVIORAL THERAPY
In addition to consulting with the patient’s medical management team, dental teams can provide professional guidance and support to help to change dysfunctional thoughts and behaviors associated with MDD.10,11 Appropriate techniques to use in the dental setting include cognitive behavioral therapy (CBT) and motivational interviewing (MI). While oral health professionals have used MI as an effective strategy for interventions,30 CBT may be an adjunct means of supporting adolescents with MDD by helping them improve self-control, perceptions of self-worth, social skills, problem-solving skills and dysphoria.11
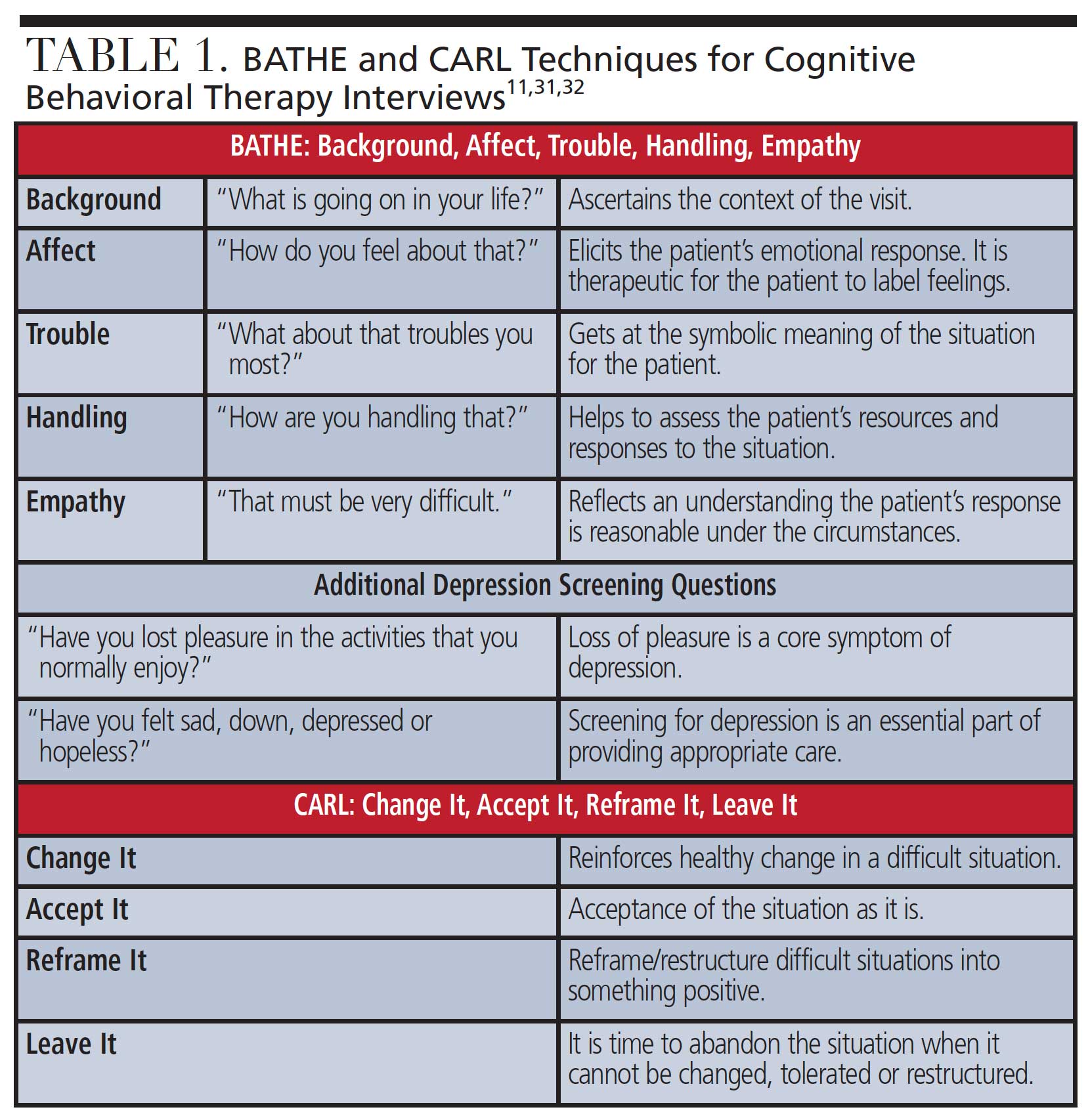
In 2006, Clabby11 introduced a menu of CBT techniques that can be used during dental appointments. For example, using the BATHE (background, affect, trouble, handle, empathy) technique during the initial interview facilitates assessment of depression, anxiety or stress disorders (Table 1). This quick assessment guide works well for identifying illnesses and managing treatment, and is the standard for medical documentation.31,32 Use of BATHE encourages adolescents to share their perceptions, feelings, concerns and solutions for a troubled situation. The clinician’s empathetic response should acknowledge the patient’s feelings and concerns as valid, and the conversation should be directed toward coping strategies that enhance the patient’s ability to control the situation.31,32 Lieberman32 suggests the addition of two more questions following the BATHE method to provide effective screening for depression (Table 1). The recognition of depressive symptoms can minimize the number of adolescents with depression who are undiagnosed or misdiagnosed.6,33
Clabby11 also described the CARL (Change it, Accept it, Reframe it, or Leave it) technique as a successful intervention for adolescents with MDD (Table 1). This tool allows adolescents to recognize and reflect on their decisions, and empowers them to think about options for difficult circumstances. Use of CARL helps adolescents with MDD reduce feelings of helplessness by understanding the four choices they have in every situation. The foundation of these strategies is patient-provider communication and rapport.11 In concert, CBT is a helpful modality because it connects coping skills to specific actions.11 The prepared dental professional can recognize adolescent depression risk factors and symptoms, subsequently introducing family support and community resources to form a collaborative care team. In this framework, dentists and dental hygienists can be part of a multidisciplinary team that supports adolescents experiencing MDD.
CONCLUSION
Oral health professionals who work with adolescents should be knowledgeable of the manifestation and appearance of depression, as this knowledge base is essential to screening in the dental setting. Working as part of a multidisciplinary care team, dental providers can facilitate early intervention and treatment that leads to positive health and behavioral health outcomes — including increased motivation to perform daily oral self-care tasks.
Clinicians can be trained in the effective use of CBT in the dental setting. This is key, because teaching coping skills and emotional regulation techniques has shown promise when applied to thoughts and behaviors associated with depression. In order to provide optimal care, dental professionals should seek to understand the complexity of adolescent depression, its effect on oral health, and the crucial role they play in serving this patient population.
REFERENCES
- National Academies of Sciences, Engineering, and Medicine. The Promise of Adolescence: Realizing Opportunity for All Youth. Available at: https://www.nap.edu/catalog/25388/the-promise-of-adolescence-realizing-opportunity-for-all-youth. Accessed January 28, 2021.
- National Institute of Mental Health. Major Depression. Available at: https://www.nimh.nih.gov/health/statistics/major-depression.shtml. January 28, 2021.
- Berk M, Williams LJ, Jacka FN, et al. So depression is an inflammatory disease, but where does the inflammation come from? BMC Medicine. 2013;11:200.
- Kisely S. No mental health without oral health. Can J Psychiatry. 2016;61:277–282.
- Hexem K, Ehlers R, Gulch J. Dental patients with major depressive disorder. Curr Oral Health Rep. 2014;1:153–160.
- Doyle PE, Longley AJ, Brown PS. Dental-mental connection. Dimensions of Dental Hygiene. 2012;10(11):19–20,22.
- American Psychiatric Association. Desk Reference to the Diagnostic Criteria From DSM-5. Washington, DC: American Psychiatric Association Publishing; 2013:94–95.
- Clark MS, Jansen KL, Cloy JA. Treatment of childhood and adolescent depression. Am Fam Physician. 2012;86:442–448.
- Siu AL. Screening for depression in children and adolescents: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2016;164:360–366.
- Kircanski K, Joormann J, Gotlib IH. Cognitive aspects of depression. Wiley Interdiscip Rev Cogn Sci. 2012;3:301–313.
- Clabby JF. Helping depressed adolescents: A menu of cognitive-behavioral procedures for primary care. Prim Care Companion J Clin Psychiatry. 2006;8:131–141.
- Saveanu RV, Nemeroff CB. Etiology of depression: genetic and environmental factors. Psychiatr Clin North Am. 2012;35:51–71.
- The American College of Obstetricians and Gynecologists Committee on Adolescent Healthcare. Mental Health Disorders in Adolescents. Available at: acog.org/-/media/project/acog/acogorg/clinical/files/committee-opinion/articles/2017/07/mental-health-disorders-in-adolescents.pdf. Accessed January 28, 2021.
- Halfin A. Depression: The benefits of early and appropriate treatment. Am J Manag Care. 2007;13:S92–S97.
- Thapar A, Collishaw S, Pine DS, Thapar AK. Depression in adolescence. Lancet. 2012;379:1056–1067.
- Naicker K, Galambos NL, Zeng Y, Senthilselvan A, Colman I. Social, demographic, and health outcomes in the 10 years following adolescent depression. J Adolesc Health. 2013;52:533–538.
- Mojtabai R, Olfson M, Han B. National trends in the prevalence and treatment of depression in adolescents and young adults. Pediatrics. 2016;138;e20161878.
- U.S. Centers for Disease Control and Prevention. National Health Interview Survey. Available at: https://www.cdc.gov/nchs/nhis/shs.htm. Accessed January 27, 2021.
- Zuckerbrot RA, Jensen PS. Improving recognition of adolescent depression in primary care. Arch Pediatr Adolesc Med. 2006;160:694–704.
- Johnson JG, Harris ES, Spitzer RL, Williams JB. The patient health questionnaire for adolescents — validation of an instrument for the assessment of mental disorders among adolescent primary care patients. J Adolescent Health. 2002;30:96–204.
- Arroll B, Khin N, Kerse N. Screening for depression in primary care with two verbally asked questions: cross sectional study. BMJ. 2003;327:1144–1146.
- Maurer DM, Raymond TJ, Davis BN. Depression: screening and diagnosis. Am Fam Physician. 2018;98:508–515.
- Kung S, Alarcon RD, Williams MD, Poppe KA, Moore MJ, Frye MA. Comparing the Beck Depression Inventory-II (BDI-II) and Patient Health Questionnaire (PHQ-9) depression measures in an integrated mood disorders practice. J Affect Disord. 2013;145:341–343.
- Parker GF. DSM-5 and psychotic and mood disorders. J Am Acad Psychiatry Law. 2014;42:182–190.
- Maida CA, Marcus M, Hays RD, et al. Child and adolescent perceptions of oral health over the life course. Qual Life Res. 2015;24:2739–2751.
- Gungormus Z, Erciyas K. Evaluation of the relationship between anxiety and depression and bruxism. J Int Med Res. 2009;37:547–550.
- Garrett AR, Hawley JS. SSRI-associated bruxism. Neurol Clin Pract. 2018;8:135–141.
- Ramesh A, Malaiappan S, Prabhakar J. Relationship between clinical depression and the types of periodontitis — a cross-sectional study. Drug Invent Today. 2018;10:659–663.
- Okoro CA, Strine TW, Eke PI, Dhingra SS, Balluz LS. The association between depression and anxiety and use of oral health services and tooth loss. Community Dent Oral Epidemiol. 2012;40:134–144.
- Gillam DG, Yusuf H. Brief motivational interviewing in dental practice. Dent J (Basel). 2019;7:51.
- Lieberman JA, Stuart MR. The BATHE method: incorporating counseling and psychotherapy into the everyday management of patients. Prim Care Companion J Clin Psychiatry. 1999;1:3–38.
- Lieberman JA. Identifying depression in primary care. J Postgrad Med. 2003;114(Suppl 5):5–9.
- Saluja G, Iachan R, Scheidt PC, Overpeck MD, Sun W, Giedd JN. Prevalence of and risk factors for depressive symptoms among young adolescents. Arch Pediatr Adolesc Med. 2004;158:760–765.
From Decisions in Dentistry. March 2021;7(3):40–43.

