
 BACKYARDPRODUCTION / ISTOCK / GETTY IMAGES PLUS
BACKYARDPRODUCTION / ISTOCK / GETTY IMAGES PLUS
Oral Health Professionals’ Role in Ending the Opioid Epidemic
Dental teams can help decrease opioid misuse through risk assessment, patient education, and treatment referrals.
PURCHASE COURSE
This course was published in the June 2022 issue and expires June 2025. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the June 2022 issue and expires June 2025. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe how the COVID-19 pandemic has impacted the opioid epidemic.
- Identify oral health professionals’ role in the opioid crisis during the COVID-19 pandemic and beyond.
- Discuss drugs used for medication-assisted treatment of opioid use disorder or harm-reduction in overdose cases.
- Develop overdose prevention and opioid misuse referral strategies for the dental setting.
The COVID-19 pandemic became a global health crisis in March 2020, exacerbating an already present crisis in substance use disorders (SUDs).1 Social isolation, financial instability, anxiety, loss of social safety nets, and disruption of addiction treatments contributed to an increase in SUDs and overdoses.1 In the United States, the number of overdoses increased 30% from 2019 to 2020, with synthetic opioids — predominately illicitly manufactured fentanyl — causing the most deaths.2 The incidence of opioid use disorder also skyrocketed during the pandemic, as did the rate of untreated mental illness.3
One in four individuals with serious mental illness also has a SUD, which often involves the overuse of opioids. During the early stages of the pandemic and national stay-at-home orders, the increase in self-reported mental health crises dramatically grew, and suicidal ideation increased by approximately 10%.3 Many individuals with serious mental illness turned to increased substance use to deal with their anxiety, depression and trauma. As the pandemic wears on, the substance abuse crisis must be addressed with health communication strategies, community-level intervention, and prevention efforts.3
Medical opioids are used to manage acute and chronic pain. While these medications are effective at alleviating pain, they also pose a high risk for abuse and addiction. Opioids act by binding to opioid receptors on nerve cells, resulting in the release of dopamine, the “reward” neurotransmitter.4 Dopamine sends messages between nerve cells, and affects motor function, mood and decision-making; it also reduces the perception of pain.4 Once opioid use becomes consistent, the body slows down its production of dopamine, and a higher dose of the drug is needed to feel the desired effects of dopamine release.1
In 2019, the National Survey on Drug Use and Health reported 10.1 million people ages 12 and older misused prescription opioids.1 Illicitly manufactured fentanyl is often mixed with heroin, methamphetamine and/or cocaine.1,5 From 2015 to 2019, the number of overdose deaths involving fentanyl, heroin, cocaine and other stimulants rose dramatically, even though the number of opioid prescriptions declined.
A schedule II prescription, fentanyl is a synthetic opioid 50 to 100 times more potent than morphine.6 Fentanyl has a shorter half-life than other opioids, and thus must be injected more frequently by illicit users to attain the desired feeling of euphoria. This increases its risk for overdose and death.
Factors Driving the Rise in Opioid Use Disorders
The COVID-19 pandemic heightened the impact of social and ethnic inequalities surrounding opioid use disorders. Marginalized populations often face greater stigma regarding abuse and addiction. People of color may refrain from using social services and frequently distrust healthcare and justice systems, leaving a large number of patients without treatment for SUDs.1 Additionally, there is a shortage of providers in minority communities, as well as a lack of diversity among healthcare professionals. These factors contribute to disparities in the treatment of opioid use disorder.
Before the pandemic, most insurance companies required preauthorization of professional therapy for opioid use disorders, and treatment itself became even more problematic during the shutdown orders. Many patients also faced difficulty accessing clinics that dispensed medication to treat these disorders.7 As a result, policy changes were made to increase access to medication-assisted treatment. For the first time, medication was dispensed in 28-day doses and compliance monitoring was conducted via video conferencing.1
Additionally, testing for the presence of both prescription and illegal drugs decreased rapidly at the start of the pandemic. This impeded access to medication-assisted treatment for opioid use disorders.7 Once testing resumed, the positivity rate for nonprescribed fentanyl increased by 35%.6
Lack of access to treatment has long been an issue in addressing the opioid crisis. Barriers to care and poor retention in treatment have been deemed the “opioid cascade.”8 Medication-assisted treatment is one of the most successful methods to help individuals recover from opioid use disorder, but there are many impediments, including stigma, lack of availability, and unwilling patients. In 2019, approximately 19% of adults with opioid use disorder received medication-assisted treatment.8 Of these, only 40% remained compliant six months after initiating treatment.8 Many medication-assisted treatment regimens require daily visits to a clinic — which, during the start of the pandemic, became impossible.
Patients accustomed to in-person addiction treatment prior to COVID-19 had to quickly adapt to telehealth. Interruption of treatment, fear of contracting COVID-19, and coping with pandemic-related stress led many individuals to return to drug use.9 Individuals abusing opioids also have a higher risk of contracting COVID-19, as they tend to have less housing security, hindering their ability to socially distance.9 The lack of safe needle exchanges due to the pandemic also raises the risk of transmission.9 Active users often have additional comorbidities due to their opioid use, which may increase the likelihood of hospitalization and need for mechanical ventilation.
Effective strategies for Oral Health Professionals
The dental team’s most effective preventive measure is education. Continuing education is key to identifying patients with a history of opioid use disorders, those currently misusing opioids, and the signs and symptoms associated with addiction. Education can also help the team stay current with state and federal regulations related to opioids.
Oral health professionals can play an important role in identifying and referring patients in need of treatment for opioid use disorders. During the pandemic, it became apparent that all healthcare professionals are crucial in recognizing the signs of social isolation and anxiety, as well identifying those without safety nets. Dental teams may be among the first to recognize those struggling with opioid use disorders due to the amount of time spent interacting with patients.10,11 In order to feel comfortable discussing opioid misuse, clinicians are advised to seek continuing education on addiction. By expanding their knowledge, providers will be better equipped to identify signs of substance abuse and more confident in talking to patients about misuse.10
The first step in identifying patients at risk for opioid use disorder is to include questions regarding substance use and/or abuse on the medical history. There is stigma attached to substance abuse, so approaching the topic without judgment is paramount. Patients should know that all answers are confidential, and that opioid use can potentially affect treatment and outcomes. The negative effects of opioids should also be discussed.10
The screening, brief intervention, and referral to treatment model is an evidence-based practice to help identify, reduce and prevent problematic use of alcohol and illicit drugs.10 A quick screening can help identify those at risk for opioid use disorder.11 The CAGE Adapted to Include Drugs questionnaire is another convenient screening option (Table 1). If the patient responds yes to any of the four questions, a brief discussion on the use of opioids should occur (brief intervention). All clinics should maintain a list of local resources for patients who may need a referral for treatment or counseling.12
Dentists have a responsibility to help prevent and mitigate opioid misuse through informed prescribing practices. The American Dental Association recommends nonsteroidal anti-inflammatory drugs (NSAIDs) as a primary control for pain from dental procedures.13 While the prescription of opioids has decreased across all healthcare professions, those made by dental providers have not decreased as dramatically.13 A recent national survey demonstrated that while dentists believe NSAID-and-acetaminophen combinations are equally effective as prescription opioids, 43% of respondents reported regularly prescribing opioids for pain management, and 69% reported seeing patients who abuse opioids. Among providers who write opioid scripts, 50% prescribe an amount that will result in leftover medication.13 Opioid misuse and abuse in dental patients may lead to adverse events, including overdoses; consequently, patients should be instructed on how to properly — and promptly — dispose of extra medication.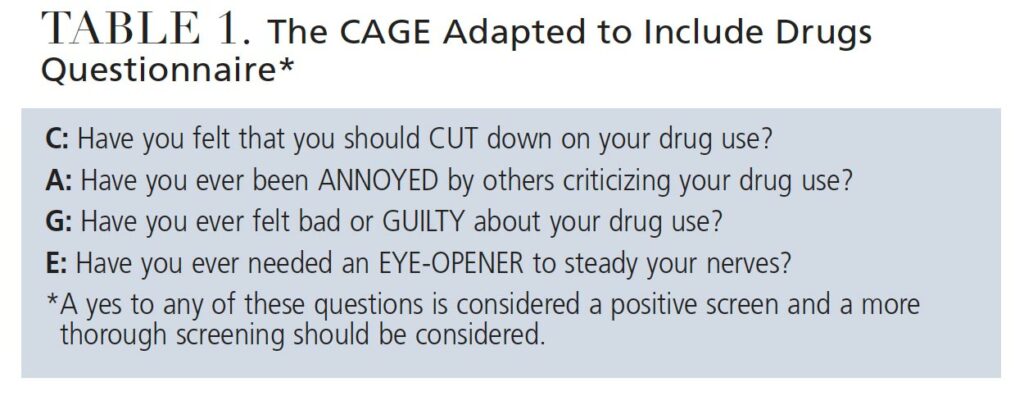
Patient Assurance
When extensive treatment is indicated, a discussion should be initiated with patients about pain management. Providers are advised to assure patients that NSAID-and-acetaminophen combinations can provide effective relief. Those with a history of addiction should be reassured their pain can be managed conservatively. For mild pain relief, ibuprofen should be considered. For moderate-to-severe pain, a combination of ibuprofen and acetaminophen is the pain management of choice. Opioids are only advised for severe pain and should be limited to a three-day supply or less.7
Before writing a prescription for opioids, the state’s prescription drug monitoring program (PDMP) should be reviewed to help determine how many opioid prescriptions the patient has received in the past.10 In a 2019 national survey, 47% of responding dentists said they had never accessed their state’s PDMP.13 Lack of awareness, not understanding how to register, and confusion about how to use the PDMP were reasons why dentists had not utilized this tool. While participants felt the program was helpful, a majority found it did not change their prescribing patterns. States with mandated PDMP utilization had a higher rate of dentist engagement. It is important to identify each state’s requirements, as there is no national guidance.13 Federal requirements would help support consistency and utilization.14
Oral health professionals should be knowledgeable about when to refer a patient to an addiction specialist. Table 2 lists behaviors or observations that would warrant such recommendations.5 As previously noted, each clinic should maintain a list of community resources, and clinicians are encouraged to cultivate a network of addiction specialists for timely referral.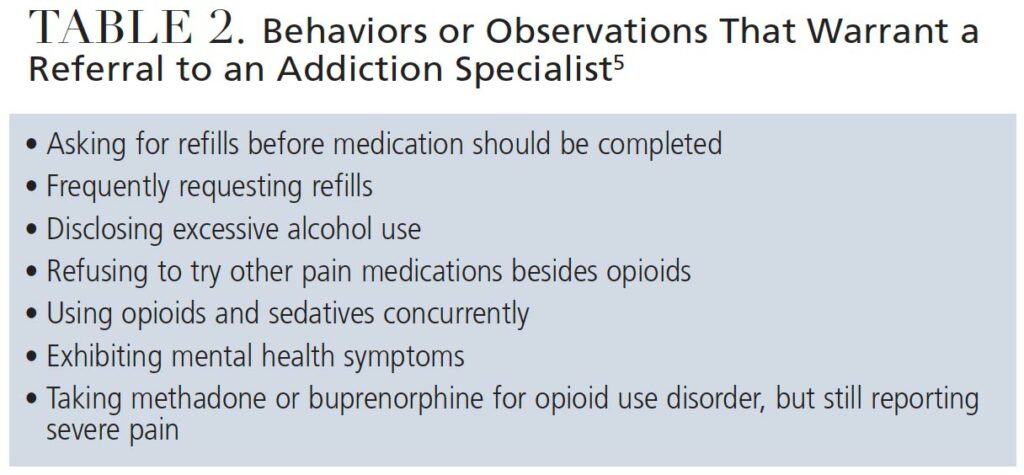
Overdose Prevention Strategies
The U.S. Department of Health and Human Services released guidance for overdose prevention strategies in response to the 250% increase in overdose deaths from 1999 to 2019.15 The guide asserts that primary prevention — including preventive programs and safe prescribing practices — is the first step. To recognize and prevent overdoses, interdisciplinary healthcare teams are necessary.15
The second step is ready access to evidence-based treatment. While oral health professionals do not treat opioid use disorder, they can provide referrals. The dental team can also use motivational interviewing to help patients identify ways to overcome social barriers to care. New treatments are also needed to help engage patients in their own care and improve compliance.8 Continuing education for providers should include communication strategies on how to discuss opioid use disorder and refer for treatment.10,11 Clinicians should maintain referral sources for pain management physicians, addiction specialists and counselors.7
Medication-assisted treatment using methadone or buprenorphine is the most common approach to opioid use disorder.7 While methadone has been the treatment of choice historically, buprenorphine is being prescribed more frequently in today’s practice.7 Methadone is only administered in outpatient clinics, which posed significant challenges during the shutdown phase of the COVID-19 pandemic. Patients on a buprenorphine regimen receive a 28-day prescription and do not require monitoring. This is because buprenorphine is an opioid partial agonist that blocks opioid receptors if a patient concurrently uses an opioid.7
Patients on either a methadone or buprenorphine regimen will experience withdrawal symptoms if the medications are ceased. When treating patients on buprenorphine, ensuring adequate anesthesia to reduce postoperative pain as long as possible is important to reduce the need for opioid pain management.7 When caring for individuals with an addiction or drug abuse history, dentists are advised to consult with the patient’s addiction specialist before prescribing opioids.
The third step in overdose prevention strategy is harm reduction.15 While every state recorded increased overdoses during the pandemic, prescriptions of buprenorphine and naloxone increased only slightly over the past three years.15 Naloxone is a common harm-reduction medication, as it is an opioid antagonist that binds opioid receptors in the brain, effectively blocking opioid receptors and reversing respiratory depression.16 When a patient receives a prescription for high-dose opioids or an opioid plus benzodiazepines, they should also receive a naloxone prescription.17 While naloxone is a critical part of treating opioid use disorder, only one prescription is dispensed for every 70 high-dose opioid prescriptions.16 One of the barriers to its use is the copay required for patients covered by Medicaid. This creates a healthcare inequity among low-income patients.11 If a patient is at high risk for opioid use disorder, dentists should consider adding a naloxone script if opioids are prescribed.
The risk for opioid overdose is high for patients who receive a dosage of 50 morphine milligram equivalents per day or greater; have chronic respiratory conditions, such as chronic obstructive pulmonary disease or sleep apnea; have been prescribed benzodiazepines or have a nonopioid SUD, such as alcohol abuse; or are diagnosed with a mental health disorder.15 A thorough medical history is necessary and a discussion of past opioid use is necessary before a prescription is written.14 If the risk for opioid use disorder is high, the provider should consider an NSAID-and-acetaminophen combination instead of an opioid script.
The final step in the prevention of opioid misuse is recovery support.15 Patients utilizing recovery support services experience improved long-term outcomes. An interdisciplinary recovery support team can help patients refrain from opioid use.15 The interdisciplinary team should consist of an addiction specialist, psychologist and treatment center representative. Oral health professionals can be part of this journey through encouragement in recovery and by helping patients achieve optimal oral health.
As a proactive measure, the Self-Management and Recovery Training program can be implemented as part of recovery support in the dental office.7 This five-step motivational interviewing process solicits behavioral changes in patients with opioid use disorder. The first step is to work with the patient to understand the reality of the problem and how it affects his or her health. The second step is to listen with empathy to the patient’s perspective, which can help remove resistance to change. Address ambivalence using motivational interviewing to explore why the patient wishes to continue to use, and why he or she should quit. If the patient is resistant to change, the clinician should modify the approach because arguing creates greater resistance. Finally, support self-efficacy through encouraging the patient to explore his or her situation and help identify possible changes.7
Conclusion
The COVID-19 pandemic has negatively impacted efforts to reduce the prevalence of opioid use disorder and overdoses. Oral health professionals can be part of preventive measures to reduce the misuse of opioids. Ongoing education involving risk assessment for opioid use disorder and optimal communication techniques will allow dental teams to more effectively help patients who are misusing opioids. In addition, dentists are encouraged to embrace non-opioid pain management strategies that do not place patients at risk.
References
- American Medical Association. National Roadmap on State-Level Efforts to End the Nation’s Drug Overdose Epidemic: Leading-Edge Practices and Next Steps to Remove Barriers to Evidence-Based Patient Care. Available at: https://www.ama-assn.org/system/files/떔-12/ama-manatt-health-2020-national-roadmap.pdf. Accessed May 5, 2022.
- Ahmad FB, Rossen LM, Sutton P. Provisional drug overdose death counts. Available at: https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm. Accessed May 5, 2022.
- Czeisler M, Lane R, Petrosky E, et al. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic — United States, June 24–30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1049–1047.
- Mayo Clinic. How Opioid Addiction Occurs. Available at: https://www.mayoclinic.org/diseases-conditions/prescription-drug-abuse/in-depth/how-opioid-addiction-occurs/art-20360372. Accessed May 5, 2022.
- Substance Abuse and Mental Health Services Administration. Key Substance Use and Mental Health Indicators in the United States: Results from the 2019 National Survey on Drug Use and Health. Available at: https://store.samhsa.gov/product/key-substance-use-and-mental-health-indicators-in-the-united-states-results-from-the-2019-national-survey-on-Drug-Use-and-Health/PEP20-07-01-001. Accessed May 5, 2022.
- Niles JK, Gudin J, Radcliff J, Kaufman HW. The opioid epidemic within the COVID-19 pandemic: drug testing in 2020. Popul Health Manag. 2021;24(S1):S43–S51.
- Nack B, Haas S, Portnof J. Opioid use disorder in dental patients: the latest on how to identify, treat, refer and apply laws and regulations in your practice. Anesth Prog. 2017;64:178–187.
- Nunes E, Levin F, Reilly M, El-Bassel N. Medication treatment for opioid use disorder in the age of COVID-19: Can new regulations modify the opioid cascade? J Subst Abuse Treat. 2021;122:108196.
- U.S. Centers for Disease Control and Prevention. COVID-19 and People at Increased Risk. Available at: https://www.cdc.gov/drugoverdose/resources/covid-drugs-QA.html. Accessed May 5, 2022.
- National Institutes of Health. Screening for Substance Use in the Dental Setting. Available at: https://nida.nih.gov/nidamed-medical-health-professionals/science-to-medicine/screening-substance-use/in-dental-setting#. Accessed May 5, 2022.
- Hoang E, Keith D, Kullch R. Controlled substance misuse risk assessment and prescription monitoring database use by dentists. J Am Dent Assoc. 2019;150:383–392.
- Melton ST, Orr RT. Detection and deterrence of substance use disorders and drug diversion in dental practice. In: The ADA Practical Guide to Substance Use Disorders and Safe Prescribing. O’Neil M, ed. Hoboken, NJ: Wiley Blackwell; 2015.
- Heron MJ, Nwokorie NA, O’Connor B, Brown RS, Fugh-Berman A. Survey of opioid prescribing among dentists indicates need for more effective education regarding pain management. J Am Dent Assoc. 2022;153:110–119.
- McCauley JL, Gilbert GH, Cochran DL, et al. Prescription drug monitoring program use: national dental PBRN results. JDR Clin Trans Res. 2019;4:178–186.
- U.S. Department of Health and Human Services. Overdose prevention strategy. Available at: https://www.hhs.gov/overdose-prevention. Accessed May 5, 2022.
- National Institute on Drug Abuse. Naloxone. Available at: https://nida.nih.gov/publications/drugfacts/naloxone. Accessed May 5, 2022.
- American Medical Association. 2021 Overdose Epidemic Report: Physicians’ Actions to Help End the Nation’s Drug-Related Overdose and Death Epidemic and What Still Needs to Be Done. Available at: https://end-overdose-epidemic.org/wp-content/uploads/떕/葕/AMA-2021-Overdose-Epidemic-Report_92021.pdf. Accessed May 5, 2022.
From Decisions in Dentistry. June 2022;8(6)32-35.

