

Minimally Invasive Removal of a Traumatic Fibroma Using CO₂ and Diode Lasers
This case report highlights the efficient and patient-friendly removal of a traumatic fibroma with a 9300 nm CO₂ laser and enhanced healing using a 970 nm diode laser.
PURCHASE COURSE
This course was published in the May/June 2025 issue and expires June 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the May/June 2025 issue and expires June 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 730
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the clinical presentation, etiology, and histological features of traumatic fibroma in the oral cavity.
- Compare traditional surgical approaches with laser-assisted excision for soft tissue lesions.
- Identify key laser parameters and techniques that preserve tissue integrity for biopsy and promote optimal post-operative healing through photobiomodulation.
During a dental career, clinicians will encounter a wide variety of benign oral mucosal lesions. One common lesion is a traumatic fibroma, also referred to as an irritation or biting fibroma. It typically presents as an asymptomatic, small, solitary mucosa-colored, smooth, pedunculated, or sessile papule.1-4 Histologically, traumatic fibromas consist of bundles of collagen fibers, fibroblasts, and an infiltrate of mild chronic inflammatory cells while the lesion is covered by a layer of stratified squamous epithelium, which may exhibit varying degrees of hyperplasia or hyperkeratosis.2-8
The formation of traumatic fibroma is linked to a history of prior injury to the mucosa. Etiologies usually include trauma by chronic cheek or lip biting, irritation from a fractured tooth, or an ill-fitting removable prosthesis.1,3,4 Symptoms range from none to varying levels of discomfort that may interfere with a patient’s daily activities such as eating. When a fibroma is present, it is often subject to further trauma by continual irritation from the patient during chewing or by repeated biting of the inflamed mucosa.1
In cases in which an individual is displaying symptoms that are interfering with his or her quality of life, treatment can involve surgical removal of the lesion, along with biopsy. In addition, the underlying source of irritation must be eliminated when possible.5,7 When any tissue of unknown etiology is excised from the oral cavity, a definitive diagnosis by histological examination of the specimen by a pathologist is recommended and, in the case of traumatic fibroma, the definitive treatment.3,9
Prior to the approval for the use of dental lasers on soft tissue by the United States Food and Drug Administration, the clinical approach for traumatic fibroma removal required the use of a scalpel or an electrocautery device.10 Using these instruments would often produce intra- and post-operative bleeding; difficulties in wound healing; necessitate sutures and deep anesthesia; and cause swelling, scarring, and post-surgical pain.10 Compared to traditional methods using scalpel or electrocautery for tissue excision, lasers produce less post-operative pain, often eliminate the need for sutures, reduce swelling, promote faster healing, and can easily be performed by general dentists.11-14 These clinical results demonstrate the laser-tissue interaction that produces a thin layer of denatured proteins in the tissue, plasma, and collagen, which acts as a biological wound dressing on the tissue surface while sealing the sensory nerve endings.15-18
Lasers are becoming a viable option for procedures in healthcare, offering a minimally invasive treatment approach for hard and soft tissue while promoting healing. The most effective lasers for soft tissue applications in dentistry are the diode (445-980 nm), Er:YAG (2940 nm), and CO2 lasers (9300 nm and 10,600 nm).10,16,19
The energy produced by these lasers is well absorbed on the cellular level by specific chromophores in the target tissue, in this case hemoglobin, melanin, and water.20 When such energy is absorbed, it causes thermal changes within the cells. This concentrated energy produces a photothermal effect, absorbed by the chromophore in a precise and controlled manner resulting in the excision/ablation of tissue and coagulation of blood vessels.15-18,21 The net result is less bleeding and faster healing times.11-14 In addition to photothermal effects, diode lasers can produce energy for photobiomodulation (PBM). This noninvasive energy is absorbed by mitochondria at the cellular level to stimulate production of adenosine triphosphate (ATP), which in turn promotes healing, reduction of inflammation, tissue regeneration, and decrease of pain.22
The clinical outcome of PBM or tissue ablation depends on the specific parameter settings of each laser including wavelength, power, duration, emission mode, beam shape, and spot size. Heat is the byproduct of energy used in PBM and can easily be controlled by contact time with the target tissue prior to the occurrence of collateral damage. For tissue ablation, these parameters can inadvertently produce damage to the surrounding tissue.21 This zone of collateral damage, referred to as the thermal damage zone, is produced by the energy absorbed in the surrounding tissue generating changes that can interfere with proper histological examination of the specimen.21
To preserve the specimen’s integrity, the provider should establish a tissue safety zone by removing tissue beyond the specimen’s margins to minimize potential damage. In this case, a CO2 laser was used due to the shallow depth of tissue penetration and corresponding narrow thermal damage zone as compared to a diode laser. For a CO2 laser, a 1 mm tissue safety zone is recommended.23
Histological artifacts in the thermal damage zone can complicate the evaluation of the collected tissue sample, therefore, it is important to incorporate an appropriate safety zone for the specific laser when excising the sample to help minimize artifacts and the misinterpretation of findings caused by such artifacts.10,21,23
The dentist should communicate to the pathologist the type of laser used along with the settings used to collect the tissue sample. This information, as well as a narrative of the surgical technique performed, will be used by the pathologist to avoid misinterpretation of the tissue sample’s margin during their evaluation as they are looking for any infiltration of hyperplastic tissue or malignancy, which could lead to inappropriate treatment strategies.10,21,23
Each year, more dental practices incorporate a diode, an erbium, a CO₂, or a combination of these lasers into their armamentarium. Clinicians must be aware of the thermal damage zones produced by a laser when excising tissue for biopsy. As previously noted, the CO₂ and erbium lasers induce a smaller thermal damage zone compared to diode lasers.10,23 Understanding these parameters enables clinicians to account for the affected tissue zones during excisions, thereby preserving the integrity of the specimen for accurate histological examination.
The aim of this report is to determine the efficiency and safety of the CO2 laser for tissue removal while evaluating the surgical operating field, patient comfort during the procedure, coagulation/need for sutures, integrity of tissue sample, and post operative pain and healing.
Clinical Case and Laser Protocol
A 68-year-old man presented to Midwestern University College of Dental Medicine, Arizona dental clinic for a routine dental appointment on March 19, 2024. The patient gave a history of cigarette smoking but none in the past 39 years, no history of smokeless tobacco or vaping, and no known allergies. The patient’s overall oral hygiene was good with minimum to low visible plaque levels and no pocket depths greater than 5 mm, except on one tooth.
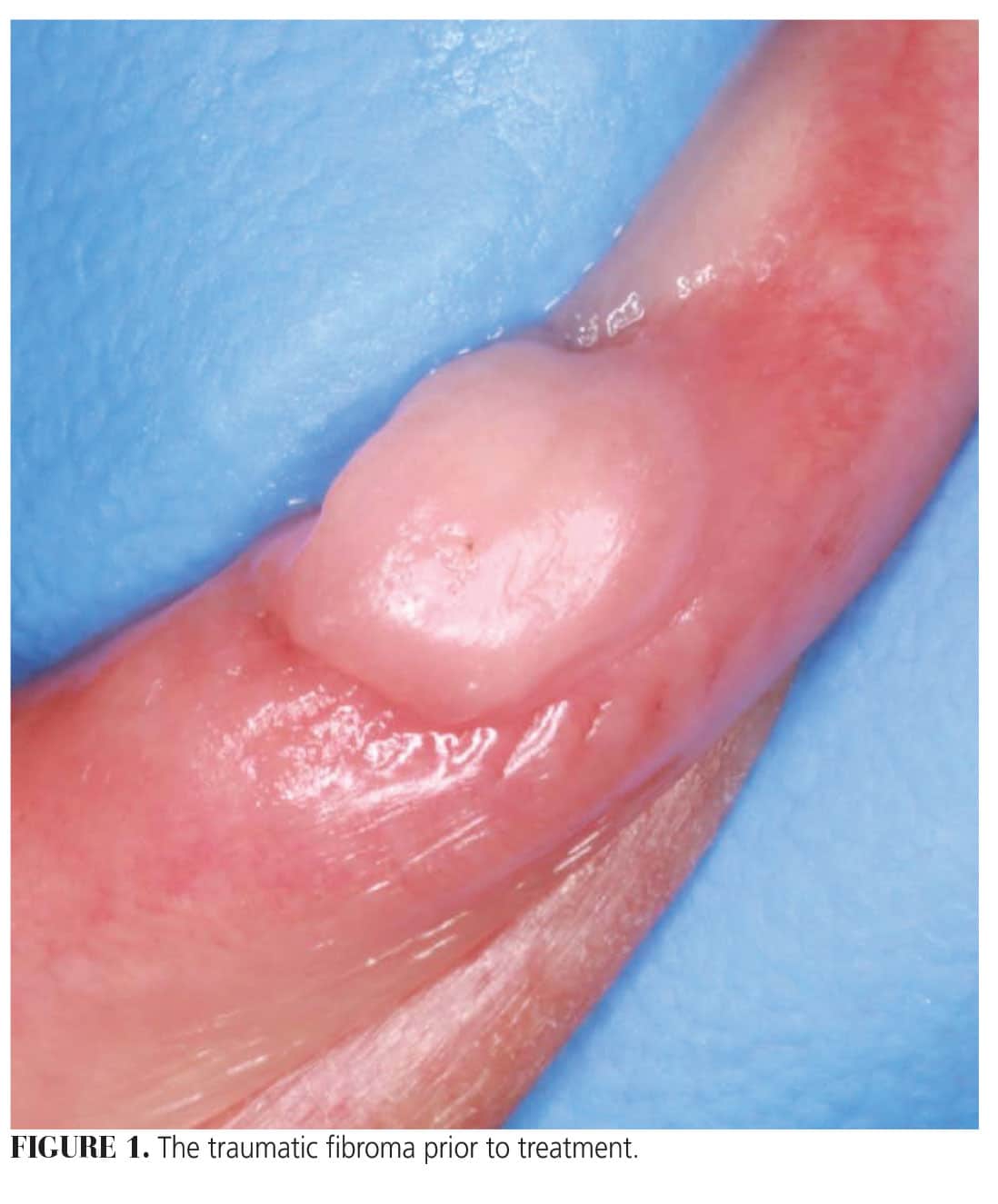
The patient reported a 3-year history of a pink, smooth, raised lesion following trauma from biting his lip. Clinical evaluation confirmed the presence of the reported lesion which was 5 mm x 5 mm in length and width on the right side of the lower lip (Figure 1). Periapical radiographs were taken with no clinical findings in the mandibular anterior quadrant. Due to a lack of other factors, a clinical diagnosis was determined to be a traumatic fibroma, which the patient elected to be removed followed by biopsy. Removal of the lesion with a CO2 laser was discussed with the patient who consented to such treatment at the next visit.
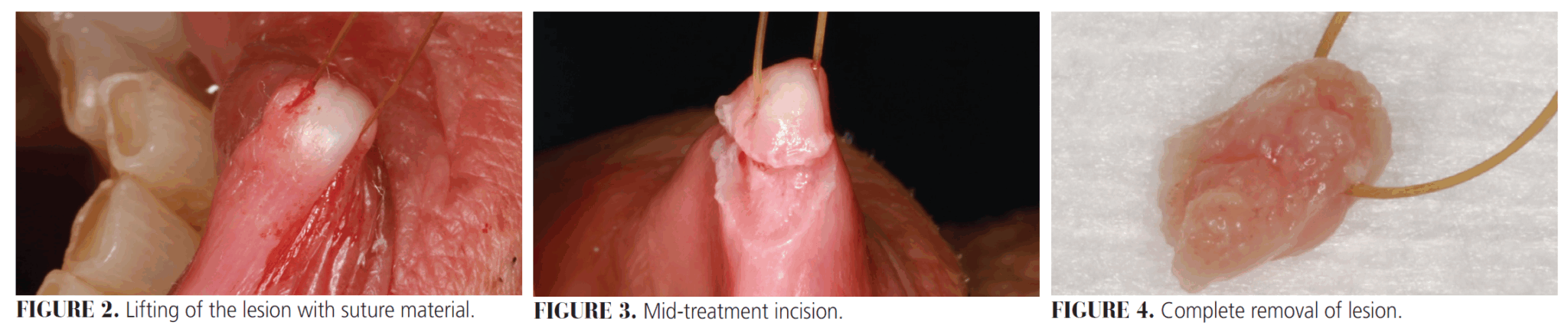
A single visit, excisional ablation/removal of the lesion was completed on March 29, 2024, with a 9300 nm CO2 laser using hard and soft tissue settings of 7W (beam spot size at target of 0.008cm2, 15% mist, and 60% cutting speed) and a skin contact application technique for about 60 seconds with 20% benzocaine topical anesthetic and 0.45 cc 2% lidocaine/1:100,000 epinephrine local anesthetic. The lesion was lifted/raised from the lip surface with a 3-0 chromic gut suture and ablated (1 mm width) in a continuous linear motion at 10 to 14 mm above the tissue surface until the entire lesion was removed (Figures 2 to 4).
The patient reported no pain during the procedure. A stable blood clot was achieved by coagulation from the laser-tissue interaction and no surgical dressing or sutures were applied to the site. Irradiance at the target was 875 W/cm2, fluence was 1.2 5J/cm2, and total radiant energy was 420 J.
In addition to the excisional biopsy the site was treated with a 970 nm diode laser using settings of 2.0 W continuous wave, 320-micron fiber (0.0008cm2 spot size) uninitiated for 30 seconds to provide stimulation (PBM) for wound healing. Irradiance and fluence at the target were 2500 W/cm2 and 2500 J/cm2 respectively and total radiant energy was 60 J.
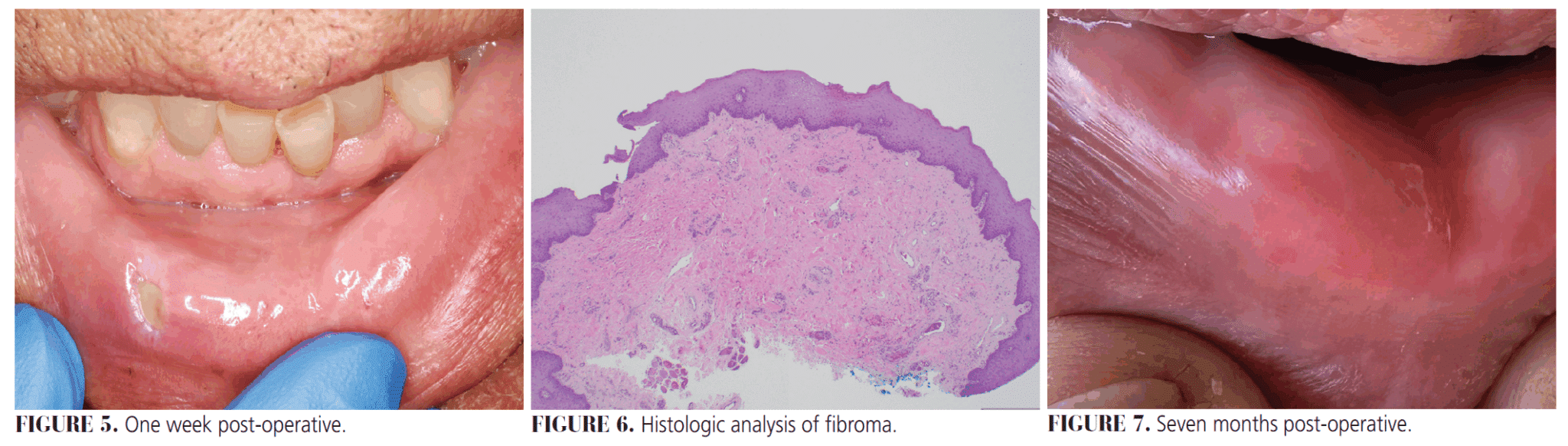
Patient was seen on April 4, 2024, for a 1-week post-operative visit. The site was healing well with no signs of inflammation and no reports of pain (Figure 5). A histologic diagnosis of fibroma from the surgical pathology report was reviewed with the patient (Figure 6). During the next several months, the patient reported further improvement in the tissue color and contour with no symptoms of pain or inflammation. On November 1, 2024, the patient sent us a final post-operative photo and was pleased with the outcome of the procedure (Figure 7).
Discussion
This case report demonstrates a successful removal of traumatic fibroma using a 9300 nm CO2 laser for excision and a 970 nm diode laser for tissue stimulation/PBM in a single visit. The surgical excision included complete removal of the lesion with a 1 + mm additional margin for safety as recommended in previous studies23,24 followed with PBM to enhance tissue healing. The excision took only 60 seconds to complete and required no sutures. We feel this was primarily due to the coagulation effect, characteristic of the CO2 wavelength of laser allowing the procedure to be completed in a bloodless operating field. In a previous study, Cohn et al25 utilized a CO2 laser to remove an amalgam tattoo with a similar surgical time while experiencing a bloodless operating field. Even though similar procedures have been reported without anesthesia,23 the patient preferred to be numb and a minimal amount of 0.45 cc of local anesthetic was used as previously described above. The patient reported no discomfort during the procedure, likely due to the use of local anesthesia but also due to the precision and short duration of the procedure.
Because the size of the lesion was clinically significant and in the esthetic zone, we chose to incorporate the use of a diode laser to stimulate wound healing. This resulted in a 30-second treatment as similarly reported by Gholizadeh et al19 and Schindl et al.27 In a similar study, Najafi et al28 found that low-level laser therapy is well tolerated by patients, causes less damage to the surrounding tissues, and provides better healing of the lesions. Healing time and tissue characteristics were favorable, pleasing to the patient, and the lesion has not recurred at the 1- year point.
This outcome compares favorably with other studies using CO2 lasers based on anesthesia used, duration of procedure, intraoperative bleeding, and post-operative pain.23,26 Finally, regarding the pathology report, the pathologist did report a cautery artifact at the surgical base but did not affect the diagnostic process.
Conclusion
This case report describes a fibroma removal using a 9300 nm CO2 laser for excision and a 970 nm diode laser to stimulate wound healing. The procedure was accomplished in a single, short visit under local anesthesia with no sensitivity reported by the patient, operative or post-operative, and healing was favorable.
Acknowledgment
The authors wish to express thanks to Midwestern University College of Dental Medicine, Arizona, for its support of the predoctoral training in laser treatment. The authors also do not have financial or other conflict of interest that relates to this case. This case report met all criteria set forth by the Midwestern University Office of Research and Sponsored Programs to be conducted as a case study and was exempt from review by the Midwestern University Institutional Review Board.
References
- Cohen PR. Biting Fibroma of the Lower Lip: A case report and literature review on an irritation fibroma occurring at the traumatic site of a tooth bite. Cureus. 2022;14:e32237.
- Hunasgi S, Koneru A, Vanishree M, Manvikar V. Assessment of reactive gingival lesions of oral cavity: a histopathological study. J Oral Maxillofac Pathol. 2017;21:180.
- Zhao X, Liu DJ, Xu CX, et al. Multiple irritation fibromas after dorsum linguae biopsy. J Craniofac Surg. 2014;25:524-526.
- de Santana Santos T, Martins-Filho PR, de Souza Andrade ES. Focal fibrous hyperplasia: a review of 193 cases. J Oral Maxillofac Pathol. 2014;18:S86-89.
- Toida M, Murakami T, Kato K, et al. Irritation fibroma of the oral mucosa: a clinicopathological study of 129 lesions in 124 cases. Oral Med Pathol. 2001;6:91-94.
- Barker DS, Lucas RB. Localised fibrous overgrowths of the oral mucosa. Br J Oral Surg. 1967;5:86-92.
- Bakhtiari S, Taheri JB, Sehhatpour M, Asnaashari M, Attarbashi Moghadam S. Removal of an extra-large irritation fibroma with a combination of diode laser and scalpel. J Lasers Med Sci. 2015;6:182-184.
- Lalchandani CM, Tandon S, Rai TS, Mathur R, Kajal A. Recurrent irritation fibroma- “what lies beneath”: a multidisciplinary treatment approach. Int J Clin Pediatr. 2020;13:306-309.
- Zarei MR, Chamani G, Amanpoor S. Reactive hyperplasia of the oral cavity in Kerman province, Iran: a review of 172 cases. Br J Oral Maxillofac Surg. 2007;45:288-292.
- Diwan B, Shirbhate U, Bajaj P, Reche A, Pahade A. Conventional scalpel and diode laser approach for the management of traumatic fibroma. Cureus. 2023;15:e47810.
- Davari A, Ziaei F. Use of CO2 laser in treatment of oral irritation fibroma adjacent to implant: a case report. J Isfahan Dent Sch. 2022;18:107-112.
- Gatlewar P, Patil RT, Dhadse P, Salian SS, Punse SD. Laser excision of buccal mucosa growth: a case report. Cureus. 2024;e70180.
- Do Amaral AL, Carneiro MC, Almeida GP, Da Silva Santos PS. Surgical treatment of oral fibrous hyperplasia with diode laser: an integrative review. Int J Odontostomat. 2023;17:136-141.
- Mendonca MP, Risemberg RIS, Maltarollo TH, Shitsuka C, Pedron IG. Peripheral ossifying fibroma removed by co2 laser: case report. SVOA Dentistry. 2021;203-207.
- Pedron IG, Muller Ramalho K, Artioli Moreira L, Moriera de Freitas P. Association of two lasers in the treatment of traumatic fibroma: excision with Nd:YAG laser and photobiomodulation using InGaAIP: a case report. J Oral Laser Ap. 2009;9:49-53.
- Suter VG, Altermatt HJ, Dietrich T, Warnakulasuriya S, Bornstein MM. Pulsed versus continuous wave CO2 laser excisions of 100 oral fibrous hyperplasias: a randomized controlled clinical and histopathological study. Lasers Surg Med. 2014;46:396-404.
- Pogrel MA, Yen CK, Hansen LS. A comparison of carbon dioxide laser, liquid nitrogen cryosurgery, and scalpel wounds in healing. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1990;69:269-273.
- Wilder-Smith P, Arrastia AM, Liaw LH, Berns M. Incision properties and thermal effects of three CO2 lasers in soft tissue. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;79:685-691.
- Gholizadeh N, Taheri JB, Namazi Z, et al. Excision of different oral benign exophytic lesions with a diode laser: a clinical case series. J Lasers Med Sci. 2020;11:502-508.
- Gundlapalle P, Nagappan N, Ramesh P, et al. Comparison of oral mucosal biopsies done using scalpel and diode lasers: a vivo study. J Pharm Bioallied Sci. 2022;14:947-954.
- Romeo U, Palaia G, Del Vecchio A, et al. Effects of KTP laser on oral soft tissues. An in vitro study. Lasers Med Sci. 2010;25:539-543.
- Dompe C, Moncrieff L, Matys J, et al. Photobiomodulation-underlying mechanism and clinical applications. J Clin Med. 2020;9;1724.
- Suter VG, Altermatt HJ, Bornstein MM. A randomized controlled clinical and histopathological trial comparing excisional biopsies of oral fibrous hyperplasias using CO2 and Er:YAG laser. Lasers Med Sci. 2017;32:573-581.
- Suter VG, Altermatt HJ, Dietrich T, Reichart PA, Bornstein MM. Does a pulsed mode offer advantages over a continuous wave mode for excisional biopsies performed using a carbon dioxide laser? J Oral Maxillofac Surg. 2012;70:1781-1788.
- Cohn MP, Wall BJ, Schuster GM, Morales R. Use of laser therapy in amalgam tattoo removal. Decisions in Dentistry. 2024;10(3):16-17.
- Kishore A, Kathariya R, Deshmukh V, Vaze S, Khalia N, Dandgaval R. Effectiveness of Er:YAG and CO2 lasers in the management of gingival melanin hyperpigmentation. Oral Health Dent Manag. 2014;13:486-491.
- Schindl M, Kerschan K, Schindl A, Schon H, Heinzl H, Schindl L. Induction of complete wound healing in recalcitrant ulcers by low-intensity laser irradiation depends on ulcer cause and size. Photodermatol Photoimmunol Photomed. 1999;15:18-21.
- Najafi S, Sheykhbahaei N, Khayamzadeh M, Gholizadeh N. The effect of low level laser on number of Candida albicans colonies in-vitro: a new finding. BMC Oral Health. 2019;19:4.
From Decisions in Dentistry. May/June 2025;11(3):40-45.

