

Mastering the Art of Broken File Retrieval in Endodontics
When a file fractures midprocedure, expert strategies and cutting-edge tools can turn a dreaded complication into a clinical success.
PURCHASE COURSE
This course was published in the May/June 2025 issue and expires June 2028. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the May/June 2025 issue and expires June 2028. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 070
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the risk factors, causes, and prevention strategies associated with endodontic file separation during root canal procedures.
- Describe the clinical protocols and tools used for retrieving broken instruments, including ultrasonic, tube, and lasso techniques.
- Explain the role of magnification, canal anatomy, and irrigation in the successful management and retrieval of fractured endodontic files.
A broken file during an endodontic procedure is a situation that every dentist dreads. The challenges and risks of retrieving the separated fragment from the canal can be daunting, but dentists are not alone in facing this.1
Fracture rates for stainless steel instruments have been reported to range from 0.25% to 6%, whereas nickel-titanium (NiTi) instruments show higher rates, ranging from 1.3% to 10%.2 Because they tend to engage into root canal walls, rotary files are more difficult to remove than hand files;3 anatomical root canal knowledge and well-managed instrumentation sequences are essential factors in minimizing this kind of accident during endodontic procedures.4
When working with NiTi files inside root canals, clinicians should avoid the following:5
- Applying negative pressure on the instrument
- Staying in rotation inside the canals
- Using wide tapers in curved root canals
The use of NiTi files can lead to cyclic fatigue, with more complex curvatures causing the most fatigue, making them more prone to fracture. A routine flute control should be conducted on the files to check for imperfections and signs of fatigue; if found, they should be discarded. Following manufacturer guidelines and analyzing root canal X-rays are critical to preventing file separation.6
During endodontic retreatments, Gates Glidden drills and NiTi files are commonly used to remove gutta-percha from the canal. However, applying high forces during this process can lead to cyclic fatigue, increasing the risk of instrument fracture.7 Even the most skilled endodontists can encounter a broken file.
Biomechanical preparation and canal patency should be established before any file separation occurs. When the canal has already been cleaned and shaped, the chances of successfully bypassing or removing a separated instrument increase due to the available space created by the enlarged canal walls.8 A key consideration is that root canals are typically elliptical rather than circular. When a fractured instrument becomes lodged against the canal wall, having the canal already shaped allows clinicians to identify the precise location of the fragment and create the necessary space to retrieve or bypass it.9
When this happens, implementing the dental microscope is critical. The benefits of multiple magnification steps and coaxial lighting make a significant difference in file retrieval management. With high magnification, the dentist ensures that the fragment is above the root canal curvature and creates the space to reach the file tip. If the dentist can see the instrument, the possibility of file retrieval is more likely.10,11 Explaining the issue to the patient is also a necessary part of ethical care.
File retrieval is impacted by the following factors:12,13
- Presence of infection
- Broken file is below the root canal curvature
- The root is thin
- The instrument fracture occurred at the beginning of the procedure when no disinfection had been done
- Status of the root section where the accident occurred
Once the retrieval file is approached, maintaining straight, clear, visual access to the fragment is crucial.14 Throughout the procedure, sodium hypochlorite should be used alternately with ethylenediaminetetraacetic acid (EDTA), combined with passive or active ultrasonic activation of the irrigants. High magnification is essential to consistently visualize and expose the reflective metal fragment.
Coronal access is the first step toward successful removal of a broken instrument. The axial wall should be enlarged adjacent to the canal containing the fractured instrument and a staging platform should be created to position the tip of the ultrasonic instrument just lateral to the coronal end of the broken file. This facilitates the initiation of trephining procedures and allows for the appropriate removal technique to be selected.15,16
Bypassing the instrument is the first and sometimes the only possible approach to minimize the risk of wear and tear of the canal walls, perforation, or access to the apical third of the canal. It is less invasive than file retrieval.17 To ensure safety and to be able to advance to the working length, K files 08, 10, and 15 should be used with constant recapitulation and irrigation.17
Today, multiple instrument retrieval tools and methods exist, including the tube technique, lasso technique, direct ultrasonic technique, and indirect ultrasonic technique. All of these can be used individually or in conjunction with another system. When choosing the most appropriate technique, domain, patience, and case analysis are key to success.18-21
Tube Technique
The tube technique is based on ready-made kits for removing broken files or silver points from the canal. As in most file retrieval techniques, the broken part of the instrument must be exposed so that the tube (cannula) can reach the coronal part of the instrument and grip it. The length of the exposed fragment and the anatomical conditions of the tooth are the two most important factors to consider when using the tube technique.22
Tube technique kits contain trephines and extractors, with diameters ranging from 0.15 mm to 0.6 mm to 0.9 mm. Most of the tube technique systems have a characteristic window, which plays a significant role in anchoring the broken fragment in the sleeve, and interchangeable screw wedges to mechanically grasp and remove intracanal obstructions. The components of all the tube systems are rigid and large in diameter. Their use is often limited to anterior teeth with wide and straight canals or the coronal third of a wide canal in molars.23
The microtube method introduces the use of modified hypodermic surgical needles or injection needles to the tube technique. This method can also be used further than the coronal third of the root canal or narrower canals, thanks to the relatively small needles.24 Another modification to the tube technique involves applying glue to the fragment with cyianocrilat into a cannula adapted or fluid resin to grip the fragment file and retrieve it.25,26
Lasso Technique
As in the other file-retrieval techniques the root canal is prepared using rotary or ultrasonic instruments to dislodge and loosen the broken fragment and expose the coronal portion for the subsequent step.27 A variety of lasso devices are available with different protocols, guidelines, and technologies. Some lasso methods can be modified to reduce costs. The lasso technique is one of the safest and the most minimally invasive approaches to file removal.27
In the lasso technique, the separated instrument is removed by placing a wire loop projecting from a needle around the fractured end of the file. Once the loop is around the file segment that needs to be removed, it is tightened. This technique works best if there is direct access to the separated instrument. An ISO 70 file or a size 2 GG bur should be used.
The head of the instrument should be exposed by creating a small circular space of at least 1 mm with an ultrasonic tip so that the lasso can be placed around the fractured instrument.28
Direct Ultrasonic Technique
Ultrasonic tips can be used to remove broken instruments from the root canal. They are used in almost all retrieval procedures, with success rates varying from 33% to 100%.29 When using an ultrasonic instrument, the diameter must be small enough to provide direct vision to the head of the broken file.30
The ultrasonic tip must be inserted around the head of the fragmented instrument in a counterclockwise motion, which involves generating ultrasonic vibrations that are transmitted to the fractured fragment to loosen it from the canal’s walls and expel it to the coronal orifice.31 As always, the use of the dental microscope, irrigation, and drying protocol ensures the clinician has a clear vision of the head of the fragmented instrument inside the canal.
Indirect Ultrasonic Technique
The indirect ultrasonic technique transfers the ultrasonic energy from the tip to create a safe motion on a secondary instrument inside the canal. It is accomplished with a sonic steel instrument kit that includes four different angulations and lengths, which are activated indirectly by piezoelectric ultrasonic tips. The transferred oscillation technology of the sonic probes completely eliminates heat buildup and greatly buffers the ultrasonic waves upon the canal walls (Figure 1).
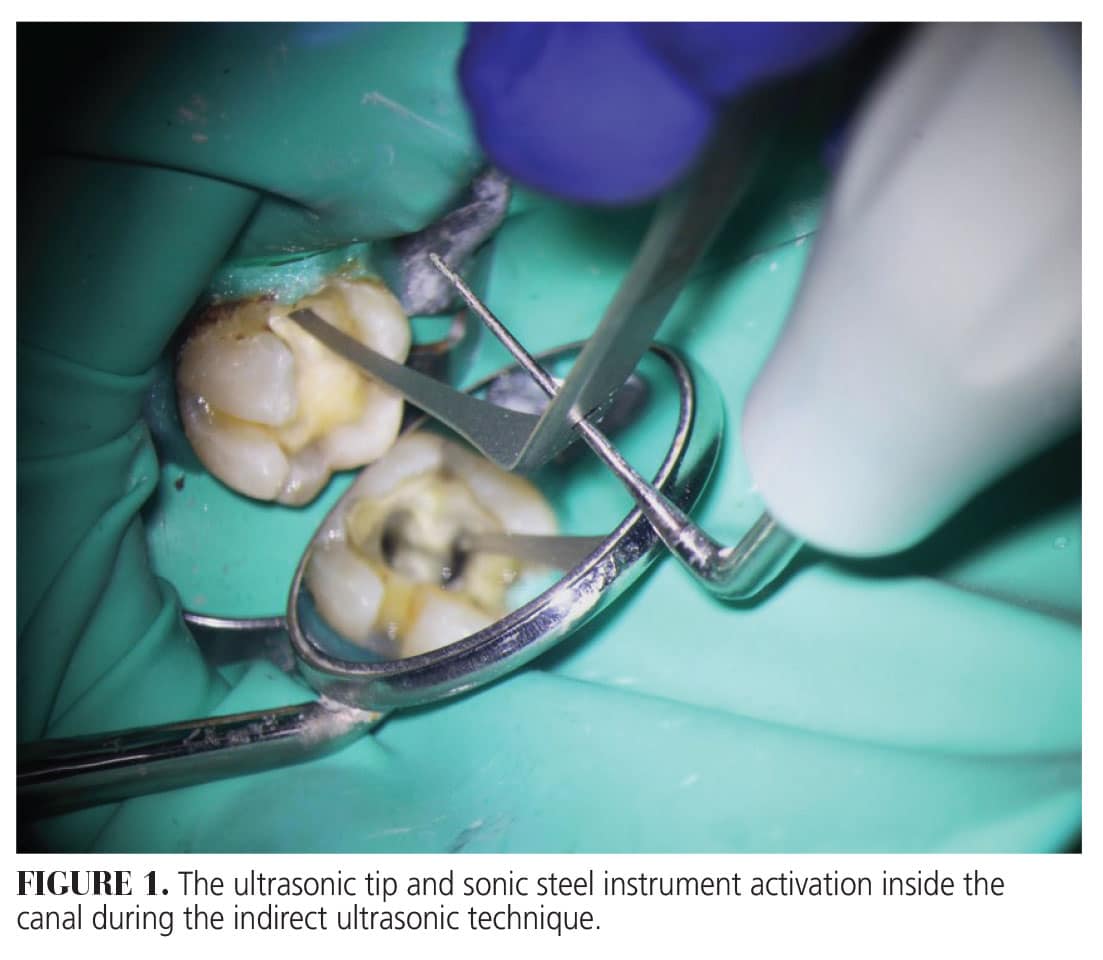
The tips are flexible with diamond-dusted active parts to create a trough and sand the sharp edges of the file. The instrument’s flexibility and different angulations follow the shapes and curves of the canal, minimizing the zips and ledges in the interior walls of the canals.
Clinical Case Report
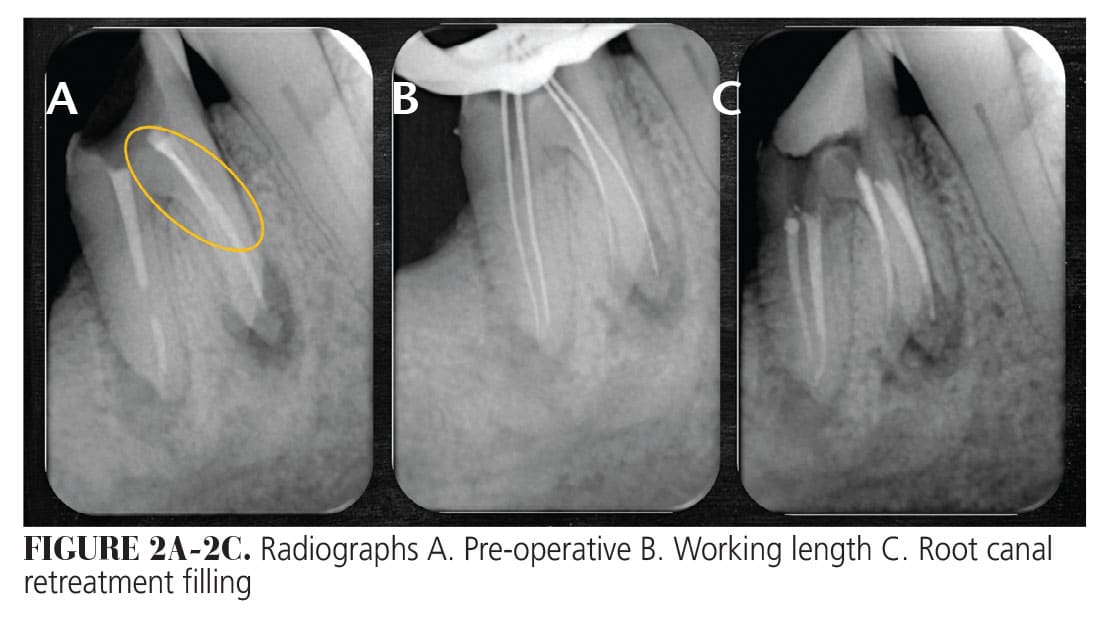
A 64-year-old man presented with mild pain in tooth #19 with a 10-year-old crown and root canal treatment. The old crown fell apart 2 days before the appointment, and the gutta-percha was exposed to the oral environment. Despite the patient being asymptomatic and the soft tissues appearing normal, the thorough examination revealed poor root canal treatment and periapical rarefactions in both roots. Radiographically a bright, white lane was located in one of the mesial canals, suggesting a broken file fragment (Figure 2A-C,).
After reviewing the microscope images and radiographs with the patient and providing a clear explanation, he demonstrated a full understanding of the proposed endodontic retreatment. This understanding and cooperation are crucial as the challenge of managing the broken file is faced.
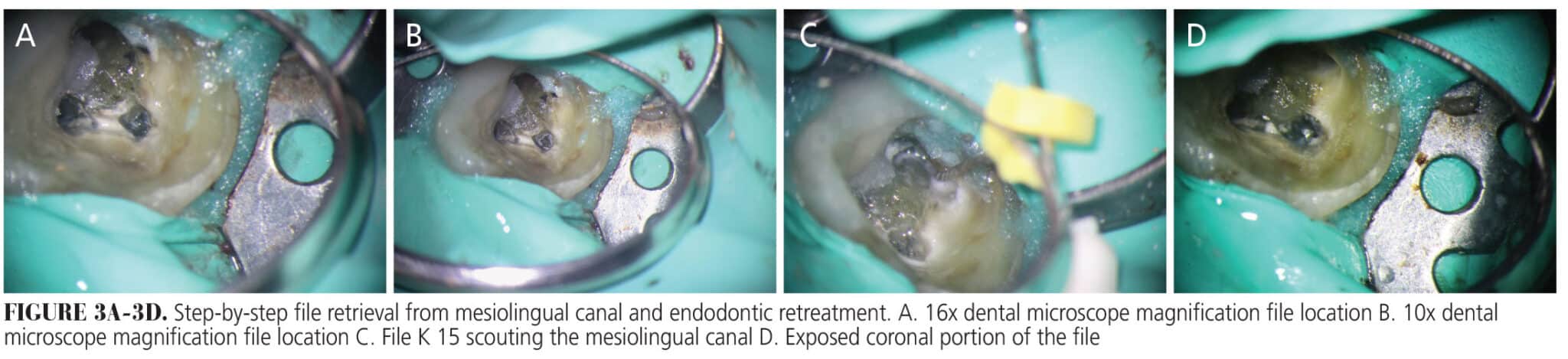
During the procedure, a dental microscope using low, middle, and high magnification was implemented. The pulp chamber walls and floor were cleaned using a ball diamond-coated ultrasonic tip and 5.25% sodium hypochlorite was used throughout the retreatment. When the coronal third of the root gutta-percha was exposed, an E5 ultrasonic tip was used to locate the distolingual unlocated canal, remove the gutta-percha, and expose the broken file from the mesiolingual canal (Figures 3 and 4).
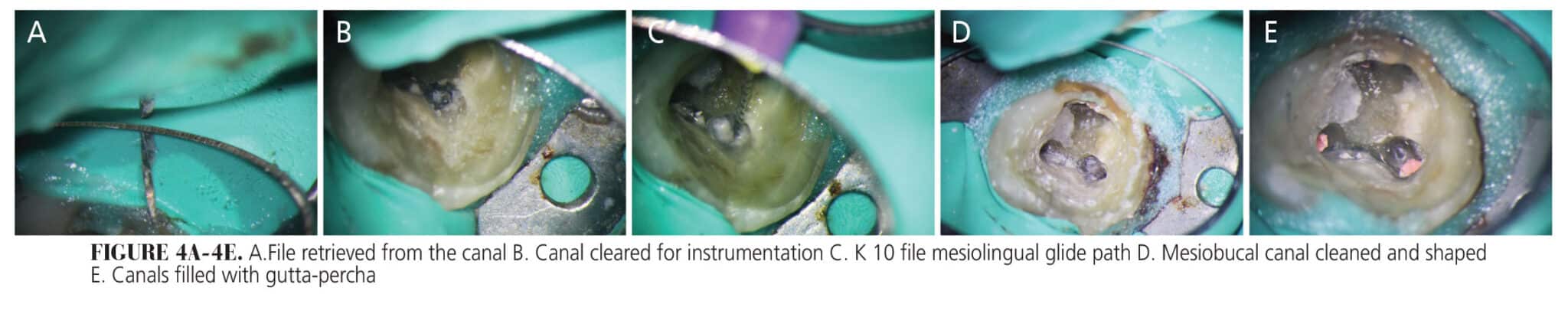
Once the broken file in the untreated mesiolingual root was exposed, an E5 ultrasonic tip was activated surrounding the coronal portion of the fragment, making space for the indirect ultrasonic system, which is activated by the ultrasonic tip. The indirect ultrasonic activation of the sonic steel diamond-coated active part of the instrument provided a smooth activation of the broken file and the canal’s wall.
The activation was done without water but alternatively irrigated with sodium hypochlorite and EDTA to deal with the smear layer. Alcohol was used to reduce drying time and paper points were implemented to dry to ensure a clear field for magnification.
When there is a slight movement of the file remnant on one side, a different angled probe was used to access the opposite side, and repeat the process. The coronal position of the instrument and the diameter of the root canal allowed for flowable management of the instrument retrieval when using the instrument to loosen it. Instrument retrieval went on for 30 minutes and the file was grabbed with Stieglitz forceps, which pulled the fragments out of the canals. Once the broken file was removed from the mesiolingual canal, the bypass and biomechanical treatment of all the root canals were completed in two appointments.
Conclusions
As endodontic retreatments are inherently challenging, the best file retrieval is the one prevented. Implementing the right protocols and using the proper instruments to handle these complex situations can pave a clear path to success. The removal of broken file instruments is best performed by skilled endodontists, as they have a deep understanding of the internal anatomy of the root canal and the tools available to manage these unexpected accidents.
The ultrasonic method for file retrieval is the gold standard; however, other techniques specifically designed for file retrieval can solve the problem as well. Using a sonic steel, ergonomically designed instrument with high magnification can aid in managing primary and complex endodontic file retrievals.
References
- Hindlekar A, Kaur G, Kashikar R, Kotadia P. Retrieval of separated intracanal endodontic instruments: a series of four case reports. Cureus. 2023;15:e35694.
- Iqbal MK, Kohli MR, Kim JS. A retrospective clinical study of incidence of root canal instrument separation in an endodontics graduate program: a PennEndo database study. J Endod. 2006;32:1048–1052.
- Suter B, Lussi A, Sequeira P. Probability of removing fractured instruments from root canals. Int Endod J. 2005;38:112–123.
- Madarati AA, Watts DC, Qualtrough AJ. Factors contributing to the separation of endodontic files. Br Dent J. 2008;204:241-245.
- Patil TN, Saraf PA, Penukonda R, Vanaki SS, Kamatagi L. A survey on nickel titanium rotary instruments and their usage techniques by endodontists in India. J Clin Diagn Res. 2017;11:ZC29–ZC35.
- Ubaed HR, Bakr DK. Cyclic fatigue resistance of nickel–titanium rotary instruments after simulated clinical use. Appl Bionics Biomech. 2022;2022:1716008.
- Kim K, Chang SW, Oh S. Buckling resistance, torque, and force generation during retreatment with D-RaCe, HyFlex Remover, and Mtwo retreatment files. Restor Dent Endod. 2023;48:e10.
- Nevares G, Cunha RS, Zuolo ML, Bueno CE. Success rates for removing or bypassing fractured instruments: a prospective clinical study. J Endod. 2012;38:442-444.
- Peters OA, Laib A, Rüegsegger P, Barbakow F. Three-dimensional analysis of root canal geometry using high-resolution computed tomography. J Dent Res. 2000;79:1405-1409.
- Fu M, Zhang Z, Hou B. Removal of broken files from root canals by using ultrasonic techniques combined with dental microscope: a retrospective analysis of treatment outcome. J Endod. 2011;37:619–622.
- Nevares G, Cunha RS, Zuolo ML, Da Silveira Bueno CE. Success rates for removing or bypassing fractured instruments: a prospective clinical study. J Endod. 2012;38:442-444.
- Parashos P, Messer HH. Rotary NiTi instrument fracture and its consequences. J Endod. 2006;32:1031–1043.
- Shen Y, Peng B, Cheung GS. Factors associated with the removal of fractured NiTi instruments from root canal systems. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98:605–610
- Lambrianidis T, Mazinis E. Parameters influencing the removal of fractured instruments. In: Management of Fractured Endodontic Instruments: A Clinical Guide. Lambrianidis T, ed. Cham, Switzerland: Springer International Publishing AG; 2018:197–206.
- Baumgartner C. Advanced endodontics: ruddle on retreatment. J Endod. 2002;28:413.
- Ruddle CJ. Microendodontic nonsurgical retreatment. In: Microscopes in Endodontic. Philadelphia: W.B. Saunders, 1997:429-454.
- Doumari B, Drouri S, Kharroubi SE, Skallli R, Benkiran I. Management of intracanal separated instrument using bypassing and braiding techniques: case reports. European Journal and Oral Health. 2024;5:1.
- Kulandaivelu. Retrieval of a separated instrument using Masserann technique. J Conserv Dent. 2008;11:42–45.
- Pruthi PJ, Nawal RR, Talwar S, Verma M. Comparative evaluation of the effectiveness of ultrasonic tips versus the Terauchi file retrieval kit for the removal of separated endodontic instruments. Restor Dent Endod. 2020;45:e14.
- Olczak K, Grabarczyk J, Szymański W. Removing fractured endodontic files with a tube technique — the strength of the glued joint: tube-endodontic file setup. Materials. 2023;16:4100.
- XIE Ke-xian, WANG Xiao. [In vitro study of a new lasso device for intra-canal broken instrument removal.] Shanghai Kou Qiang Yi Xue. 2021;30(6):606-610.
- Olczak K, Grabarczyk J, Szymanski W. Removing fractured endodontic files with a tube technique-the strength of the glued joint: tube-endodontic file setup. Materials (Basel). 2023;16:4100.
- Ruddle CJ. Nonsurgical retreatment. J Endod. 2004;30:12.
- AlRahabi MK, Ghabbani HM. Removal of a separated endodontic instrument by using the modified hollow tube–based extractor system: a case report. SAGE Open Med Case Rep. 2020;8:2050313X20907822.
- Bürklein S, Donnermeye D, Wefelmeier M, Schäfer E, Urban K. Removing fractured endodontic NiTi instruments with a tube technique: influence of pre-treatment with various agents on adhesive forces in vitro. Materials (Basel). 2019;30:144.
- Wefelmeier M, Eveslage M, Bürklein S, Ott K, Kaup M. Removing fractured endodontic instruments with a modified tube technique using a light-curing composite. J Endod. 2015;41:733-736.
- American Association of Endodontists. SP-3 A Modified File Retrieval Technique Using a Newly Developed Lasso Device. Available at https://endoondemand.aae.org/products/sp-3-a-modified-file-retrieval-technique-using-a-newly-developed-lasso-device. Accessed May 7, 2025.
- van der Vyver PJ. Modern considerations when approaching fractured endodontic instruments — part 2: a review of the literature and clinical techniques. South African Dental Journal. 2020;75(10):
- Terauchi Y, Ali WT, Abielhassan MM. Present status and future directions: removal of fractured instruments. Int Endod J. 2022:55:685-709.
- Plotino G, Pameijer CH, Grande NM, Somma F. Ultrasonics in endodontics: a review of the literature. J Endod. 2007;33:81-95
- Madarati AA. Retrieval of multiple separated endodontic instruments using ultrasonic vibration: case report. Journal of Taibah University Medical Sciences. 2016;11(3):268-273.
From Decisions in Dentistry. May/June 2025;11(3):32-35.

