

How 3D-Printing Is Reshaping the Dental Workflow
From surgical guides to same-day crowns, photopolymer-based three-dimensional printing is transforming digital dentistry.
Three-dimensional (3D) printing, once considered a curiosity confined to engineering labs, has rapidly become a foundational technology for modern dentistry.¹ As dentists transition from traditional milling methods that carve away at blocks of material to additive processes that build restorations layer by layer, they have embraced an unprecedented level of customization and efficiency. Milling offered significant advantages by shortening chairside time for single-unit restorations, but it also created limitations on geometric complexity and wasted potentially costly materials.² The additive approach, however, constructs parts only where needed, minimizing excess and opening possibilities for intricate designs that milling could never replicate.
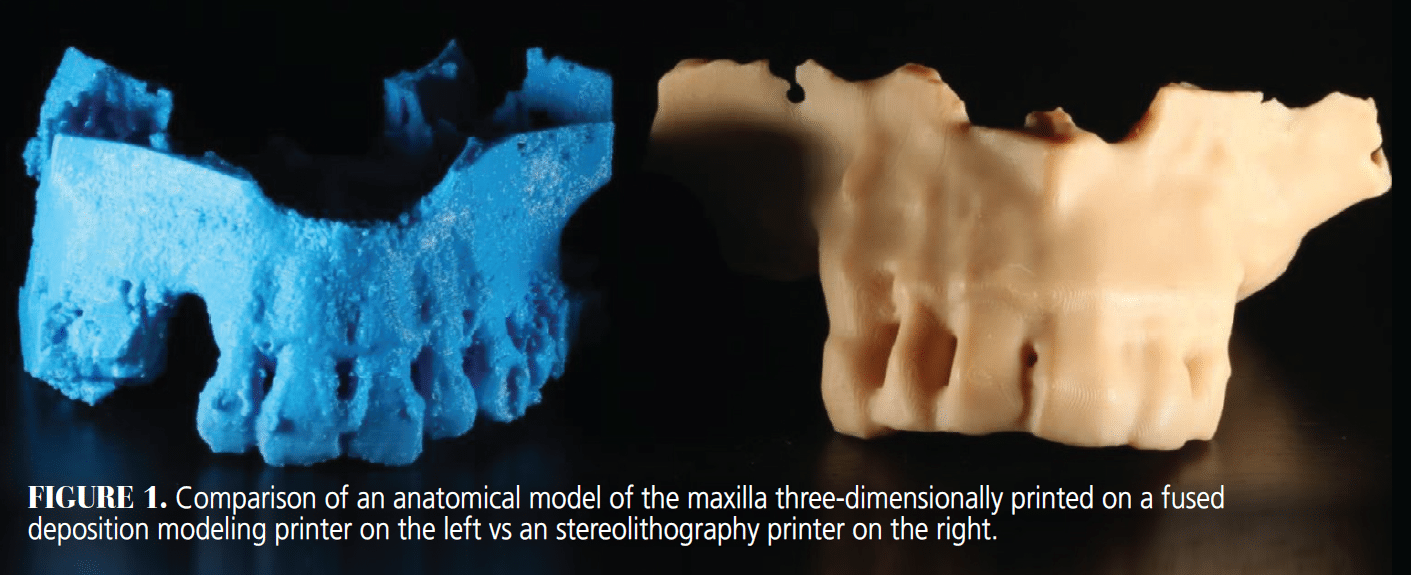
Yet the initial foray into additive manufacturing for dentistry was not always smooth. Early experiments with fused deposition modeling printers produced coarse finishes, questionable mechanical properties, and visible layer lines ill-suited for intraoral use.³ The true turning point came with the refinement of photopolymerization-based 3D printing (Figure 1), particularly stereolithography apparatus (SLA) and digital light processing (DLP). By using laser beams or projector flashes to selectively cure layers of resin with ultraviolet (UV) or visible light, these technologies deliver the high resolution and physical strength necessary for many dental applications, such as night guards and provisional hybrids.⁴
Small and more affordable “desktop” SLA/DLP printers became available, enabling their entry into everyday clinical workflows. This shift from large, expensive laboratory-based machinery to compact, user-friendly devices allowed dentists to print surgical guides, temporary crowns, dentures, and orthodontic models on demand.⁵ Additionally, resin-based 3D printing is conceptually familiar territory for many clinicians. In dentistry, light-based polymerization has long been the foundation for curing composites; SLA and DLP simply apply that same principle in a layer-by-layer approach to fabricate precise 3D objects.
From Milling to Additive Mastery
The leap from milling to additive manufacturing was driven largely by a desire for finer detail and reduced material waste. Milling, while groundbreaking in its heyday, is subtractive: a block of ceramic or composite is whittled away to form a restoration.² This process can be wasteful, particularly for complex shapes. Intricate internal geometries are nearly impossible to mill out without specialized burs, and the leftover ceramic powder or composite dust often cannot be reused. For restorations that demand highly specific contours or internal channels, such as implant-supported frameworks, subtracting material quickly becomes impractical.
In contrast, SLA and DLP deposit or cure only the material needed for a given design. The build platform in these printers descends incrementally into a vat of photosensitive resin; after each layer is cured, the platform lifts so fresh resin can flow underneath.⁴ The resin that remains uncured can stay in the vat for subsequent prints, minimizing waste. This efficiency aligns well with sustainability goals that many dental practices are now adopting. More important, additive manufacturing supports shapes and design features that were either prohibitively difficult or impossible with milling. Dentists can incorporate features, such as retentive elements, undercuts, or highly detailed anatomical geometry, in surgical guides and restorations.³
While milling technology remains a valuable option for certain restorations and materials (eg, zirconia crowns), its limitations become evident as digital dentistry moves toward increased customization. Indeed, some large laboratories still rely on milling for metal substructures or final ceramics, but many labs are also adopting or converting to additive systems. The versatility of 3D printing, combined with improvements in resin durability, is quickly closing the gap between what was once a specialized adjunct process and a mainstream clinical tool.⁵
Harnessing Resin-Based Technologies
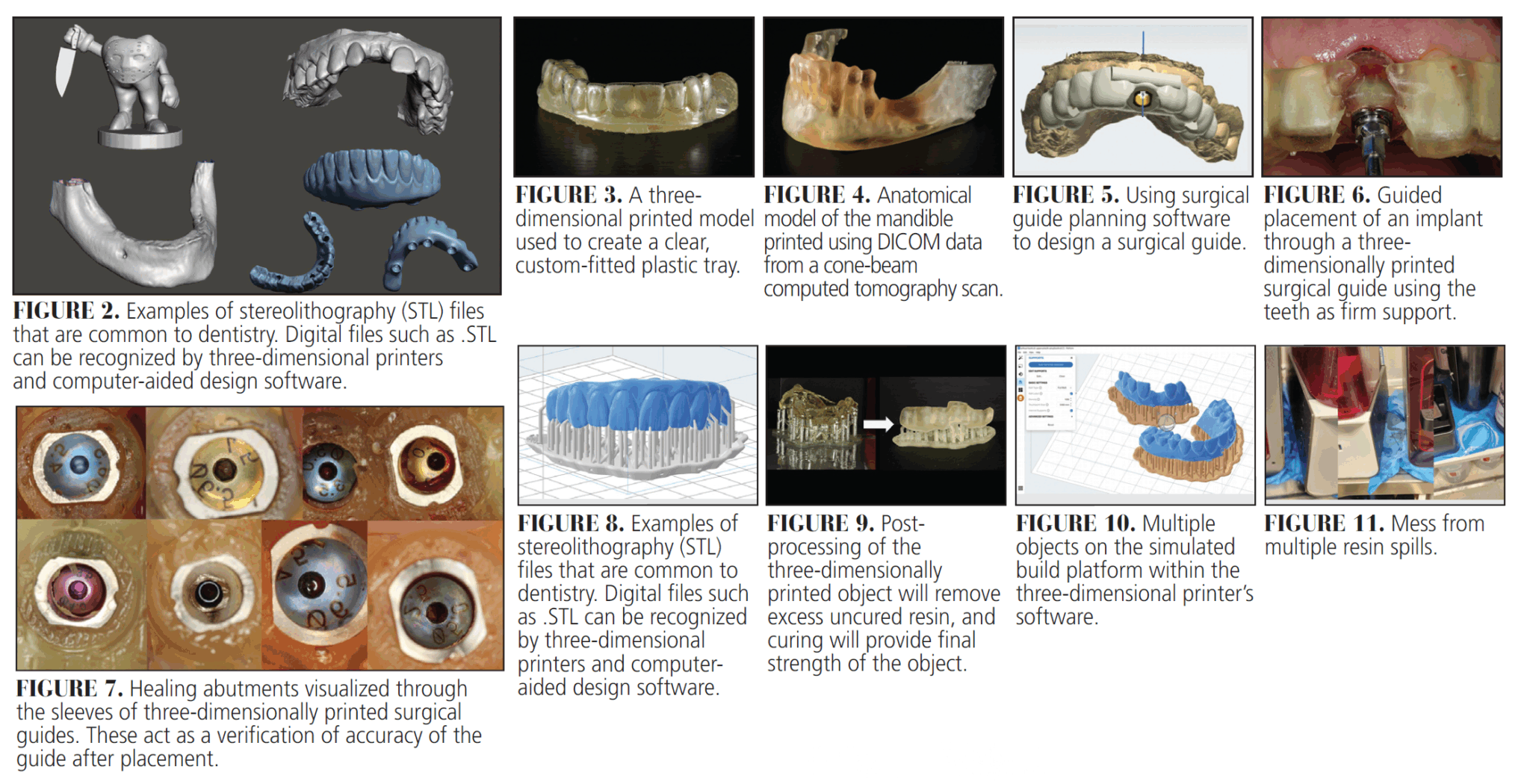
SLA relies on a UV laser that traces thin cross-sections of a steriolithography (STL) file (Figure 2) within a photosensitive resin tank. As each layer is exposed, it solidifies, and the build platform rises to allow the next layer to form.⁶ DLP also uses photopolymer resins but cures each layer in one flash of projected light rather than a moving laser beam. Both approaches deliver surprisingly high accuracy: resolution as fine as tens of microns ensures that appliances such as night guards or implant guides fit almost perfectly upon delivery (Figure 3).
Resin-based printing also caters to the varied demands of different applications. Surgical guides require a rigid, transparent resin that can be sterilized; dentures or splints might need a resin that mimics gum tissue flexibility or is tinted for esthetics.⁴ Temporary crowns usually call for formulations that balance mechanical strength with surface polish and shade matching.⁵ These materials are not only differentiated by their mechanical properties but also by regulatory classifications because any resin that contacts patient tissue must meet strict biocompatibility standards.¹ With continual research and new developments, these printer-specific resins are advancing rapidly, enabling more durable, color-stable, and high-strength results.
Clinical Workflow in Action
 The typical workflow for a 3D-printed dental restoration or appliance often begins with digital data acquisition. Intraoral scanners capture STL files of teeth and soft tissues at micron-level detail, while cone-beam computed tomography (CBCT) provides DICOM data (Figure 4) of the underlying bony structures.⁷ These datasets can be merged in software (Figure 5), allowing dentists to plan implant placement or model restorative margins. Surgical guide creation involves mapping the planned implant angulation and depth onto a digital model of the arch, then generating a guide design to fit snugly around existing dentition (Figures 6 and 7).
The typical workflow for a 3D-printed dental restoration or appliance often begins with digital data acquisition. Intraoral scanners capture STL files of teeth and soft tissues at micron-level detail, while cone-beam computed tomography (CBCT) provides DICOM data (Figure 4) of the underlying bony structures.⁷ These datasets can be merged in software (Figure 5), allowing dentists to plan implant placement or model restorative margins. Surgical guide creation involves mapping the planned implant angulation and depth onto a digital model of the arch, then generating a guide design to fit snugly around existing dentition (Figures 6 and 7).
Once the design is finalized, printing software automatically adds support structures in areas that will not affect the seating surface (Figure 8). In STL printing, the vertical resolution is set by the thickness of each cured layer, so thinner layers yield smoother surfaces but take longer to build. The user then selects a layer thickness — most printers offer three common presets: 25 µm for ultra-high detail (eg, castable patterns and thin-wall shells); 50 to 100 µm for balanced clinical work (eg, surgical guides, splints, provisional restorations); and 100 to 150 µm for rapid model production (eg, orthodontic study casts or aligner molds where fine layer lines are hidden during thermoforming). This 50- to 100-µm window usually strikes the best compromise: fine enough to capture delicate occlusal anatomy and margin detail, yet thick enough to keep print times practical and reduce the risk of interlayer defects.
After printing, the part is typically rinsed in isopropyl alcohol to remove uncured resin, then exposed to UV light in a curing unit (Figure 9). This final cure ensures the object reaches its recommended mechanical properties and biocompatibility. Supports are removed and, if necessary, the appliance is polished.
In practices that outsource large volumes of lab work, performing these steps in-house can significantly reduce turnaround times and increase control over the final product. Dentists who print their appliances can iterate on designs rapidly — tweaking an occlusal guard to reduce bulk or adding small retention features to a provisional crown — without incurring repeated lab fees. The result is a nimble workflow that patients appreciate, not just for the novelty but for the tangible decrease in waiting time and, in many cases, total cost.⁸
Clinical Advantages and Real-World Experiences
The main advantage of 3D printing is precision. When prints consistently achieve accuracy within a few microns, fewer adjustments are needed chairside, and final seating becomes more predictable.⁶ Equally important is the ability to print multiple items simultaneously (Figure 10, page 16). A single build platform might hold a full-arch model, a bite splint, and a surgical guide, enabling batch production that suits busy practices. This flexibility extends to a wide range of applications: some clinicians rely on 3D printing to produce bleaching tray models or orthodontic aligner setups, while others print custom impression trays or even try experimental workflows for partial denture frameworks.
Despite success stories, real-world anecdotes reveal that 3D printing does come with practical challenges. Resin spills are notorious; one small tilt of the resin vat can make a sticky mess that rivals the clinginess of spilled honey (Figure 11, page 16). Similarly, handling uncured resin demands protective gloves, eye protection, and careful disposal procedures.¹ Printer maintenance is another consideration. Over time, factors, such as dust on mirrors, aging projector bulbs, or worn resin tanks, can degrade print accuracy. This means that a clinic must adopt some protocols akin to a mini lab environment, devoting space, time, and staff training to keep the system running smoothly.⁴
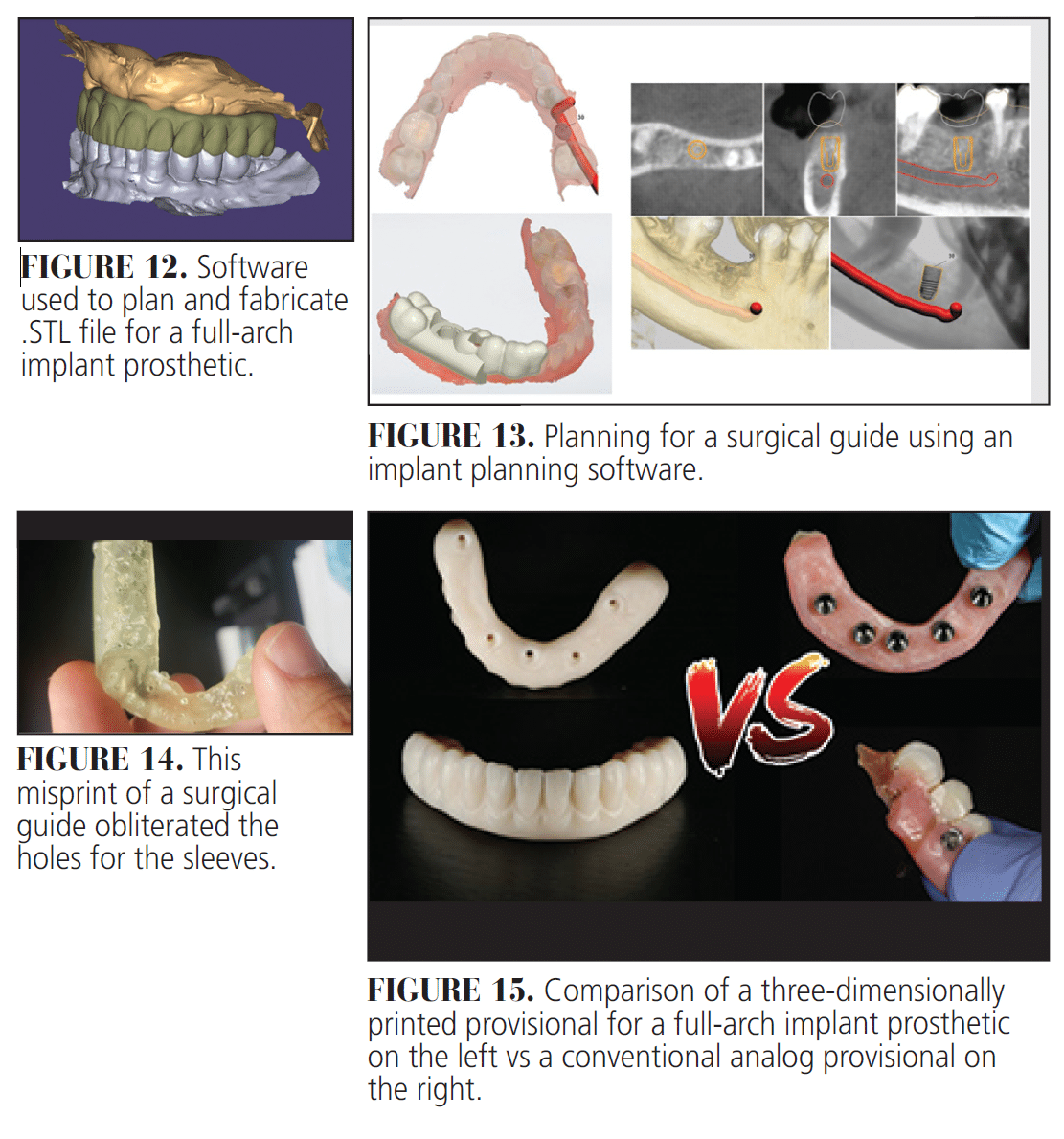
Clinicians also describe a learning curve in mastering the software (Figure 12). Designing surgical guides, for instance, involves importing CBCT data, segmenting the jawbone, merging intraoral scans, and placing virtual implant fixtures before exporting the final STL for printing (Figure 13). Mastery of these steps can be time-intensive, especially for less tech-savvy staff. Yet many have found that tackling simple projects, such as printing study models, helps the team gain confidence quickly, paving the way for more advanced applications.⁷
Challenges and Considerations
One pivotal concern is ensuring material safety. Not all resins are cleared for intraoral use, so clinicians must confirm their chosen resins meet United States Food and Drug Administration’s or European Conformity (CE) standards for biocompatibility. Post-print processes, such as thorough washing and UV curing, are integral to making sure any residual monomers are minimized.⁴ Even with the right materials, issues can arise from operator error or rushed post-processing, underscoring the importance of adequate staff training.
Printer calibration must be carried out at regular intervals. A misaligned build plate or partially obstructed laser can turn a routine print into a warped or partially cured fiasco (Figure 14).² Consumables, such as the resin tray, have limited lifespans, as the translucent membrane that contacts the UV light can cloud or tear over time. Moreover, different resins often require separate trays to prevent cross-contamination. These overhead details can surprise dentists expecting a completely hassle-free experience, but adopting a standardized maintenance schedule can keep misprints to a minimum.
Looking Ahead
The future of 3D printing in dentistry is boundless. Artificial intelligence (AI) tools capable of real-time margin detection, occlusal scheme optimization, and implant angulation prediction already exist in some capacity, and their integration with 3D printing could compress workflows into near chairside experiences.⁷,⁸ Bioprinting — in which living cells are deposited onto scaffolds — hints at the possibility of regenerating missing bone or gingival tissues in situ rather than relying solely on grafts.⁶,⁹ While printing entire teeth with their own pulp remains speculative, each advance in regenerative medicine and scaffold design brings that concept a step closer.
New resin formulations push beyond the boundaries of what was once possible with polymers in the dental realm.10 Durable, color-stable, and fracture-resistant resins that rival conventional ceramic materials are edging closer to mainstream availability (Figure 15). With these enhanced materials and improved printer reliability, the distinction between a “temporary” 3D-printed solution and a “permanent” milled or cast restoration may gradually blur.
Another trend is the scaling up of 3D printing for high-volume production. Some large dental labs are adopting automated systems capable of printing dozens of aligner models in a single cycle, complete with robotic arms that remove parts and initiate new jobs. The synergy of scanning, AI-driven design, and hands-off printing promises faster turnarounds and fewer human errors. Even in smaller practices, partial automation, such as connecting an intraoral scanner directly to the printer’s software, reduces manual file handling and speeds up day-to-day operations.
Conclusion
Three-dimensional printing in dentistry merges precision, efficiency, and customizability in ways that older manufacturing methods could not. Though it requires an investment of time and capital, many dentists who adopt this technology soon discover the power of on-demand fabrication for surgical guides, dentures, occlusal guards, and beyond. Careful handling of resin, regular maintenance of equipment, and consistent operator training remain nonnegotiable, ensuring a safe and reliable workflow.
As new materials gain regulatory approval and AI-driven design matures, dentists stand at the cusp of further breakthroughs. Already, patient demands for faster service and personalized solutions dovetail with 3D printing’s inherent strengths. In many ways, it is the fulfillment of digital dentistry’s promise to free clinicians from the constraints of manual techniques and to create a future where virtually any shape or configuration can be manufactured at will. It is perhaps only a matter of time before fully regenerative, bioprinted teeth become a reality, further cementing additive manufacturing as a mainstay in the modern dental practice. Until then, each cured layer brings fresh opportunities for innovation and patient satisfaction.
References
- Revilla León M, Sadeghpour M, Özcan M. A review of the applications of additive manufacturing technologies used to fabricate metals in implant dentistry. J Prosthodont. 2020;29:579-593.
- Lerner H, Nagy K, Pranno N, et al. Trueness and precision of 3 D printed versus milled monolithic zirconia crowns: an in vitro study. J Dent. 2021;113:103792.
- Wang G, Wang S, Dong X, et al. Recent progress in additive manufacturing of ceramic dental restorations. J Mater Res Technol. 2023;26:1028-1049.
- Lai YC, Yang CC, Levon JA, Chu TMG. Effects of additive manufacturing technologies and finish line design on the trueness of 3 D printed dies. J Prosthodont. 2022;32:519-526.
- Perlea P, Ștefănescu C, Dalaban MG, Petre AE. Dimensional variations of 3 D printed dental models based on printing orientation. Clin Case Rep. 2024;12:e8630.
- Fayyaz Y, Ali M, Ullah R, Shaikh MS. Applications of 3D printed teeth in dental education: a narrative review. J Taibah Univ Med Sci. 2024;19:816-822.
- Chen Y, Wei J. Application of 3D printing technology in dentistry: a review. Polymers. 2025;17:886.
- Gkantidis N, Koopman P, Ross K, et al. 3D printed orthodontic aligners: a scoping review. Appl Sci. 2024;14:10084.
- Agarwal S, Mistry LN, Kamath S, et al. Pioneering the future of oral healthcare: bioprinting and its transformative clinical potential in dentistry. Cureus. 2025;17:e79030.
- Jun MK, Kim JW, Ku HM. Three dimensional printing in dentistry: a sco.ing review of clinical applications, advantages, and current limitations. Oral. 2025;5(2):24.
From Decisions in Dentistry. July/August 2025;11(4):14-18.
