
Enhancing Early Caries Management
vVARDIS’ Curodont is perfectly designed to support the Innovative Proactive Enamel Repair Protocol.
Dental caries is the most prevalent chronic disease worldwide, yet traditional dentistry often fails to intercept disease at an early stage.1 The Innovative Proactive Enamel Repair Protocol (IPERP) integrates advanced diagnostics and biomimetic therapy to preserve and restore natural enamel and reduce the burden of surgical restorative care.
This article expands on the rationale for why I developed IPERP, reviews the underlying science of detection and repair, illustrates clinical case applications, and reports practice-level outcomes. The findings underscore that IPERP not only transforms the clinical pathway of caries management but also strengthens patient trust and facilitates practice growth.
Dental caries, affecting more than 2.3 billion individuals and more than 520 million children globally, is a significant public health challenge with substantial physical, social, environmental, and economic implications.1 Traditional dentistry has largely focused on surgical restorative care — diagnosing decay once structural damage is visible, intervening surgically through drilling, and replacing the lost tooth structure with an artificial substitute.2 Not only is this approach costly and irreversible, it can also trigger long-lasting dental anxiety, especially in the pediatric population, eroding trust between families and clinicians.3
Innovative Proactive Enamel Repair Protocol
IPERP was conceived as a paradigm shift to serve as both a clinical workflow and a philosophical model for the future of dentistry. The core principle is to preserve as much natural tooth structure as possible while guiding biological healing processes. IPERP employs diagnostic technologies to identify the earliest stages of disease and applies biomimetic therapies to repair enamel via hydroxyapatite generation.
The IPERP workflow redefines the hygiene visit as a platform for proactive disease interception rather than just routine prophylaxis, with minimal additional chairtime. Communication is central, with technology serving as the bridge between clinical insight and parental understanding.
Diagnosing Early-Stage Caries
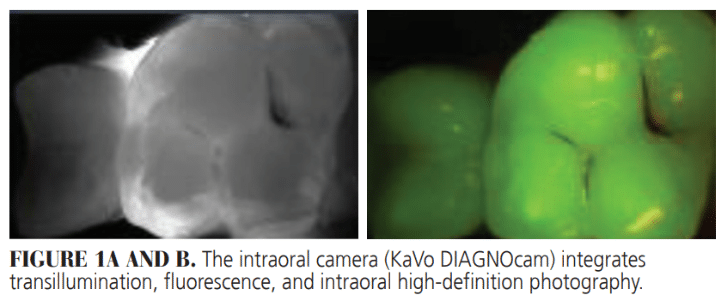
I combine the use of tried-and-tested diagnostic methods with modern techniques to systematically identify carious lesions that are still noncavitated. Among the ones I use routinely is an intraoral camera, which integrates transillumination, fluorescence, and intraoral high-definition photography (Figure 1).4 As it involves no radiation, it is safe for repeated use in pediatric patients. It also helps families visualize hidden lesions on screen, strengthening patient communication.
Artificial Intelligence in Radiography
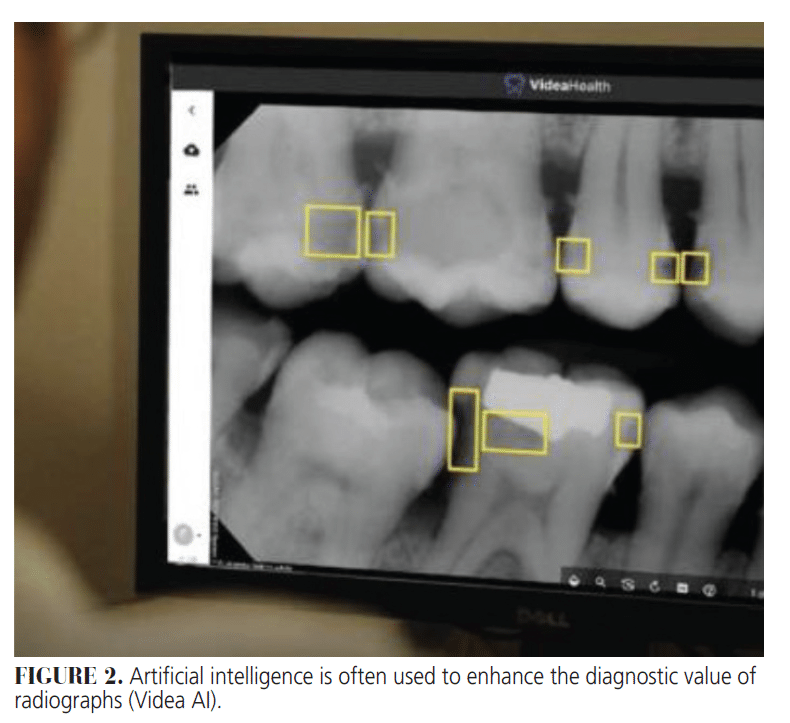
Today, artificial intelligence (AI) is increasingly used to enhance the diagnostic value of radiographs. I use AI in my practice to highlight areas of concern in real time, supporting more confident decision-making and patient communication as well as improving treatment acceptance (Figure 2).
When combined with these advanced diagnostic tools, AI-interpreted radiography provides an additional layer of diagnostic certainty, creating a robust system of detection that minimizes error.5
Guided Hydroxyapatite Generation
The therapeutic foundation of IPERP is the treatment of early-stage caries with guided hydroxyapatite generation, implemented with vVARDIS’ Curodont Repair Fluoride Plus. This biomimetic formulation, containing a low concentration of fluoride (~225 ppm), penetrates the pseudo-intact surface of noncavitated caries and disperses into the entire body of the lesion (Figure 3). It utilizes calcium and phosphate ions from the saliva for hydroxyapatite generation throughout the depth of the lesion.6-8
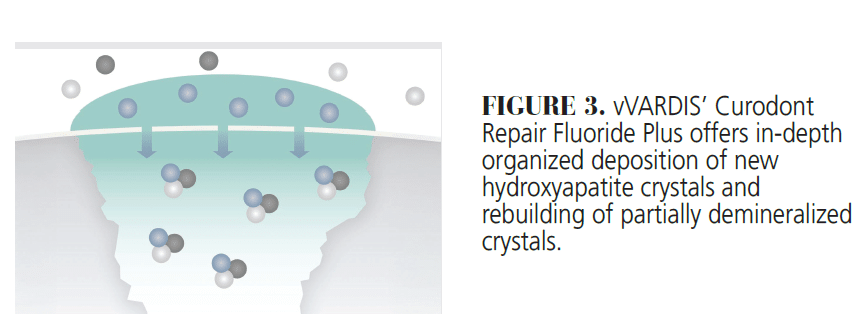
Curodont Repair Fluoride Plus bridges the gap between surface-level preventive strategies and invasive restorative solutions with in-depth, organized generation of new hydroxyapatite crystals and rebuilding of partially demineralized crystals. Nonstaining, Curodont is implemented through an easy and quick procedure in as little as 3 minutes of chairtime.9
A recently published in vitro study used micro-computed tomography (CT) and scanning electron microscope (SEM) analysis to evaluate the effect of Curodont on artificial enamel carious lesions (n = 3) over 2 weeks.10 The micro-CT analysis demonstrated a 15% increase in mineral density (p < 0.001) with no significant difference in lesions depths at which this improvement occurred.
The SEM images show areas near the lesion surface to be fully fused with sound enamel and larger hydroxyapatite crystals in the deeper areas compared with the control.10 This represents the central therapeutic innovation of IPERP. It operationalizes the principle of minimal intervention, allowing children to avoid drilling, anesthesia, and surgical restorative cycles.
The Protocol’s Workflow
The IPERP workflow integrates diagnostics and therapy into a structured patient journey. The steps are as follows:
- Screening begins with early-stage caries identification using diagnostic methods such as localized pH testing, transillumination and fluorescent imaging, and AI-supported radiographs.
- Parents are educated using visual evidence and colorimetric confirmation.
- Prophylaxis is completed as part of the routine hygiene visit.
- Curodont is applied during the same appointment.
- Supportive self-care measures are prescribed.
- Regular recalls to diagnose new lesions in a timely manner and treat them noninvasively.
Case Series
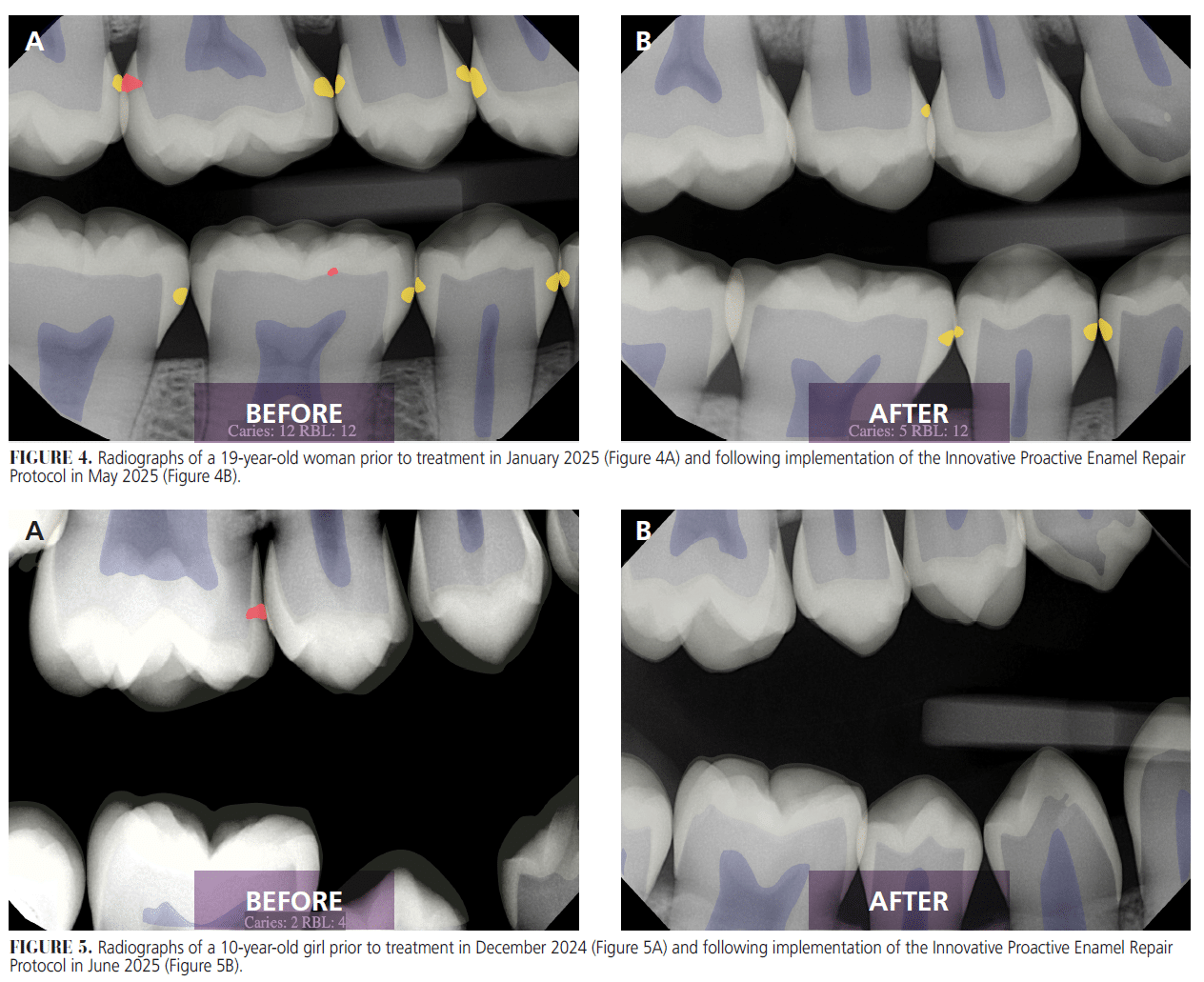
In 2024, I documented outcomes directly attributable to IPERP (Figures 4 and 5). Treatment acceptance reached 95%, driven by the clarity of diagnostic visuals and the simplicity of the noninvasive intervention. IPERP has easily integrated into our existing workflows and allowed us to be more efficient, without auxiliary staff involvement or additional chair time.
IPERP illustrates that by adopting thorough diagnostics and biomimetic repair, clinicians can intervene earlier and more effectively. The results of IPERP resonate with broader movements in healthcare that emphasize prevention, personalization, and minimally invasive interventions, with implications that extend beyond the operatory.
Especially for pediatric dentistry, IPERP helps develop in children lifelong positive relationships with oral healthcare and motivate parents to invest in early intervention. For underserved populations, as exemplified by my work with Nosara Sonríe, a program that provides free pediatric dental care, education, and treatments to children in the Nosara district of Costa Rica, noninvasive protocols could extend the reach of care in resource-limited settings.
From a practice management perspective, IPERP offers a protocol that aligns the patient benefit with practice growth. Rather than relying solely on surgical restorative cycles, practices can grow through minimal, early intervention services that enhance trust and long-term retention.
Conclusion
IPERP redefines the management of early caries. The combination of cutting-edge modern diagnostics and a science-driven noninvasive technology that works by in-depth restoration of hydroxyapatite can preserve enamel, improve patient trust, and strengthen practice sustainability.
vVardis
vvardis.com
800-217-0064
References
- FDI World Dental Federation. Oral Health in Comprehensive Cleft Care. Available at fdiworlddental.org/cleftcare. Accessed October 15, 2025.
- Ismail AI, Tellez M, Pitts NB, et al. Caries management pathways preserve dental tissues and promote oral health. Commun Dent Oral Epidemiol. 2013;41:e12-40.
- Karim R, Splieth CH, Schmoeckel J. Impact of invasiveness of dental treatment history on anxiety expression in recall patients. Minerva Dent Oral Sci. 2025;74:232-240.
- Söchtig F, Hickel R, Kühnisch J. Caries detection and diagnostics with near-infrared light transillumination: clinical experiences. Quintessence Int. 2014;45:531-538.
- Negi S, Mathur A, Tripathy S. Artificial intelligence in dental caries diagnosis and detection: an umbrella review. Clin Exp Dent Res. 2024;10:e70004.
- Khairy SM, Talaat DM, Dowidar KML. Remineralization of white spot lesions in primary teeth using an intensive application protocol of curodont repair fluoride plus, mi varnish or duraphat varnish (randomized controlled clinical trial). J Evid Based Dent Pract. 2025;25:102163.
- Shaalan O, El-Sayed KF, Abouauf E. Evaluation of the remineralization potential of self-assembling peptide P11-4 with fluoride compared to fluoride varnish in the management of incipient carious lesions: a randomized controlled clinical trial. Clin Oral Investig. 2024;28:438.
- Amin OA, Shaalan OO, Riad M. Remineralization potential of curodont repair flouride plus versus cpp-acp in white spot lesions. Advanced Dental Journal. 2023;5(1):110-118.
- vVARDIS AG. Curodont Repair Fluoride Plus. Available at https://professional.vvardis.us/product/curodont-repair-fluoride-plus. Accessed October 15, 2025.
- Cowen M, Gilmartin M, Powers JM. In vitro evaluation of enamel carious lesion treatment with Curodont™ Repair Fluoride Plus. Biomater Res Rep. 2025;175.
From Decisions in Dentistry. October/November 2025;11(5):20-22.
