

Embrace the Digital Future
How dentists can leverage technology-savvy graduates to transform their practices’ digital workflows.
In 2023, the term “digital imperative” emerged as a prominent new buzzword reflecting the urgency of digital transformation. A recent addition to the professional lexicon, digital imperative represents a critical call to action.1
In the rapidly evolving landscape of dental technology, this mindset is essential. Digital transformation has moved from optional to operational, fundamentally changing how dentists diagnose, plan, and treat. Today, chairside computer-aided design and computer-aided manufacturing (CAD/CAM) systems, intraoral scanners (IOS), and digital design software are not luxuries but necessities. They define the contemporary standard of care and drive both patient satisfaction and practice efficiency.2
For owner-dentists, the challenge is not just adopting digital tools but embracing them in a way that sustains growth and clinical relevance. Fortunately, a new wave of digitally fluent graduates is emerging from dental schools. These future practitioners bring valuable insights and hands-on experience in digital workflows, making them ideal partners in modernizing legacy practices. ideal partners in modernizing legacy practices.
The Intraoral Scanner
The IOS is the cornerstone of digital dentistry. Its origin dates to 1985, with the introduction of the first CAD/CAM system.3 While groundbreaking, the early iterations of the technology faced significant challenges, particularly in scanning precision and image reconstruction. Initially, they relied on monochromatic images and a video-based optical impression system that was highly sensitive to moisture, required perfect isolation, and had difficulty handling reflective surfaces. The software algorithms had limited processing power, making it difficult to achieve clinically acceptable accuracy and reducing the usefulness of early digital impressions.4
These early systems laid the groundwork for the current generation of IOS devices, which now offer rapid, highly accurate scans and are easy to use.5 As digital implant impressions become more reliable and accurate, now comparable to traditional methods,6 the use of conventional impression materials may decline. As a result, dental students may have less exposure to traditional materials, with future graduates relying more on digital scanners.
New graduates entering private practice have typically completed extensive IOS training. Many dental schools now require students to complete full-arch scans and design restorative cases using digital tools.7,8 These students graduate with fluency in IOS, digital margin, assessment, and file preparation. These skills enable them to immediately integrate and flourish in digitally progressive practices.
Advantages of Incorporating Digital Workflows
For owner-dentists looking to modernize their workflow, these graduates represent a vital resource. By onboarding new associates who are comfortable with IOS workflows, clinicians can:
- Reduce the learning curve for the entire team
- Improve accuracy
- Accelerate the practice’s transition into the digital age
- Help evaluate existing systems
- Guide decisions regarding digital upgrades, including scanner compatibility, data management, and integration with milling or lab communication systems.
As part of this transition, owner-dentists must decide whether to adopt open or closed IOS systems. Closed systems streamline the learning curve and provide end-to-end integration, while open systems offer greater flexibility and collaboration with outside labs.9 Whichever path is chosen, implementation must include training for the entire dental team to reach a functional level of competency.10
Open vs Closed Digital Systems
Understanding the difference between open and closed digital systems is crucial when building a sustainable digital workflow, especially for practices integrating new graduates into their clinical teams. Table 1 outlines advantages and disadvantages.
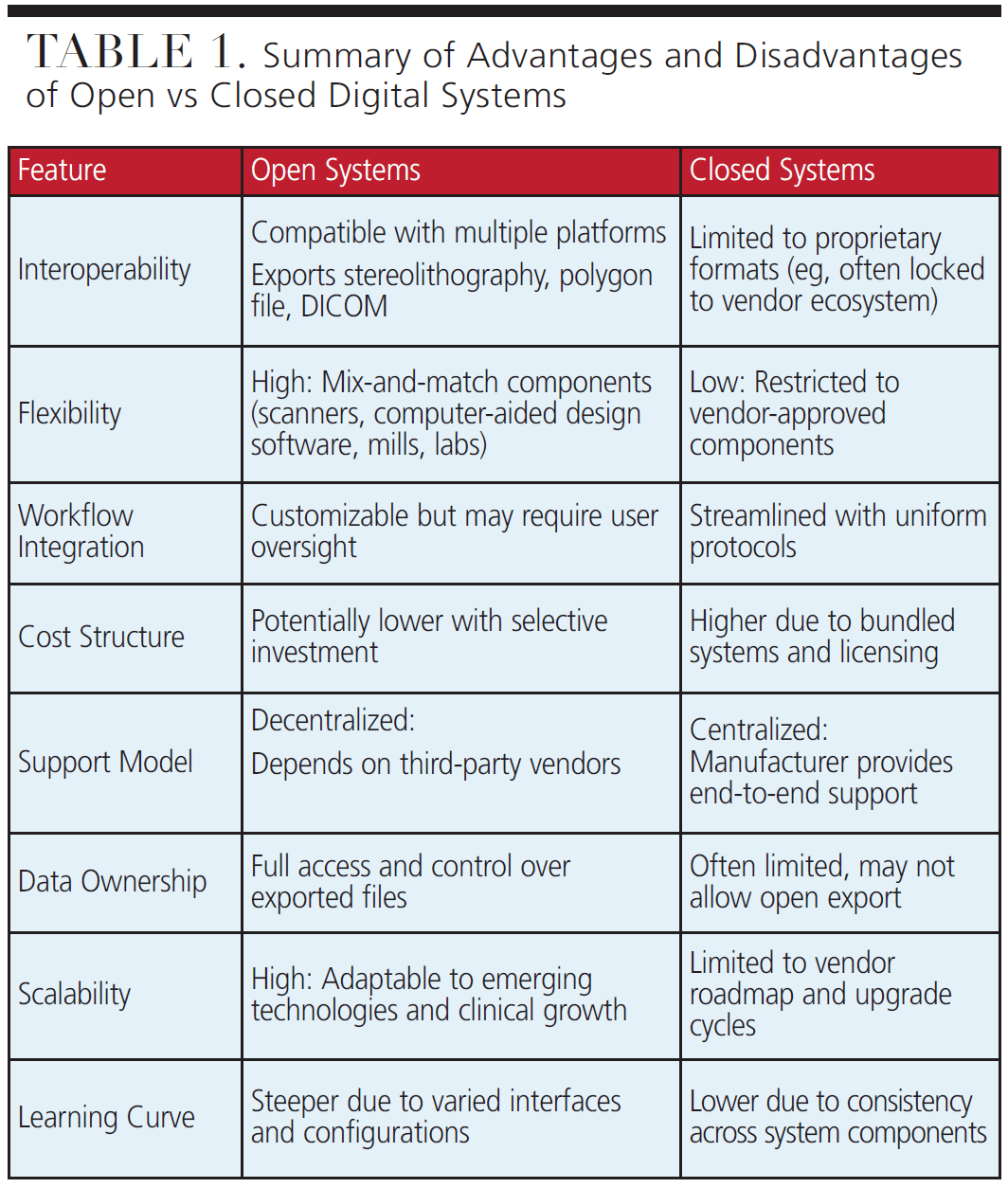
Closed systems are proprietary ecosystems in which all components, including the scanner, design software, and milling unit, are designed by a single company to function seamlessly together. These systems offer simplified onboarding, consistent user interfaces, and dependable manufacturer support.11 Because the software and hardware are unified, troubleshooting is more straightforward, updates are synchronized, and technical assistance is streamlined. This can make closed systems appealing for owner-dentists just beginning their digital transition or looking to minimize their offices’ information technology complexity. However, these systems typically restrict the ability to export files freely, limiting collaboration with third-party laboratories and compatibility with outside software or hardware, forcing users into subscription-based cloud portals.11 Essentially, stereolithography (STL) files may not be easily exported or manipulated outside of the system’s design environment.
In contrast, open systems are nonproprietary digital ecosystems that allow components from different manufacturers to work together through standardized file formats.11 These systems are built around flexibility and interoperability rather than exclusivity. A practice might combine a scanner from one manufacturer with a desktop scanner from another, combined with leading open-source dental design software and a compatible milling unit. This approach allows dentists to customize their digital system based on their unique clinical needs and financial considerations.
Open systems allow more seamless collaboration with external labs, cloud-based storage, and incorporation of future technologies as they emerge.12 The trade-off is that open systems require a deeper understanding of digital workflows and equipment interoperability. When improperly managed, mismatched components or software versions can lead to workflow breakdowns, clinical errors, and end-user frustration
New graduates exposed to both open and closed digital systems are familiar with universal file formats (eg, STL and polygon) as well as proprietary ones and gain hands-on experience with various design software platforms and collaborative digital tools. This background equips them to serve as valuable resources in guiding practices through the complexities of system selection and integration. From a mentorship standpoint, these graduates can help assess existing digital infrastructure and suggest upgrades that strike a balance between ease of use and long-term flexibility.
The choice between an open or closed system is not about right or wrong, it is about alignment with practice goals and the end-user skill set. Practices focused on speed, simplicity, and single-visit dentistry may thrive with a closed system. Prioritizing laboratory collaboration, advanced prosthetics, user flexibility, and vendor relationships may benefit from an open approach. When paired with digitally fluent new associates, owner-dentists can create hybrid environments that can combine the predictability of closed systems with the innovation of open platforms.
Dental graduates trained in closed digital systems are well-prepared to enter private practices and help navigate the integration of both open and closed technologies. Their understanding of digital workflows allows them to manage interoperability between different devices, enhancing patient care and expanding the practice’s digital capabilities. Practices aiming to build a flexible and scalable digital infrastructure can benefit from this versatility. On the other hand, practices seeking a more streamlined and predictable approach to digital adoption may find closed systems better suited to their needs.
Designing in the Digital Age
Once an IOS captures a scan, CAD software enables clinicians to design virtual restorations. Today’s systems include artificial intelligence-driven features, such as margin detection, virtual articulation, and automatic proposal generation.13 However, clinical oversight is essential to ensure accuracy, esthetics, and biomechanical compatibility.
New graduates trained in CAD workflows can bring fresh perspectives and critical thinking to the design process. In educational settings, students learn to refine crown contours, assess occlusal forces, and identify interferences before milling.14 This skillset is highly transferable to private practice and can enhance diagnostic capabilities, reduce remakes, and improve patient communication.
Chairside vs Lab-Based Design
Owner-dentists must decide whether to scan, design, and mill restorations in-house or outsource them to a dental laboratory. In-office workflows offer same-day delivery and full control but require time investment and training. Lab workflows provide material versatility and esthetic refinements, though at the cost of turnaround time and additional fees.15
Hybrid mode, in which simpler cases are handled in-office and complex ones sent to the lab, can maximize efficiency. For example, practices might use chairside milling for posterior crowns but collaborate with labs for layered zirconia anterior restorations.16 Graduates accustomed to this dual approach can help calibrate case selection and optimize outcomes.
Computer-Aided Manufacturing and Material Choices: from mill to mouth
Once a restoration is designed, CAM translates it into a physical product. Options include chairside milling, 3D printing, and lab outsourcing. Lithium disilicate remains the gold standard for its esthetics and durability.17,18 Zirconia, initially limited to posterior zones, has now gained esthetic viability in anterior applications due to improvements in translucency.19
In-office milling offers speed and patient convenience, while 3D printing is growing in use for splints, surgical guides, and digital dentures.20 These tools require proper training and maintenance. New graduates, having handled these tools in school, can guide the practice team through effective implementation.
Beyond the Digital Design
The success of a CAD/CAM workflow culminates in the delivery of the final restoration. Despite digital precision, adjustments are sometimes necessary. Clinicians must evaluate margins, occlusion, proximal contacts, and esthetics. For lithium disilicate, appropriate etching and bonding protocols are vital; for zirconia, cementation technique and primer selection matter and new materials, such as 3D printed resins, require new processing techniques and those trained to do it.21
Digital occlusal mapping and virtual articulation tools now allow clinicians to preemptively visualize occlusal interferences, reducing chairside adjustment time.22 These tools, when used with clinical judgment, can significantly enhance workflow efficiency and clinical success.
Preparing the Team
Digital dentistry is not plug-and-play. Its success depends on team-wide education. One common pitfall is the underutilization of technology due to a lack of proper onboarding and inadequate follow-up training. Owner-dentists must provide training not only for themselves but also for dental hygienists, dental assistants, and front office staff.23
New graduates are often ideal super-users who can coach and develop staff, helping the owner-dentist train and support the staff. They can serve as digital mentors, helping to onboard technology and troubleshoot issues. Dental education now emphasizes cross-functional learning, in which students collaborate with lab technicians and digital support to gain a holistic understanding of digital systems.24
Structured mentorship programs can help bridge generational gaps between owner-dentists and new graduates. For example, a mentorship framework may include:
- Weekly digital case review meetings
- Joint attendance at continuing education courses focused on CAD/CAM or digital implantology
- Shadowing opportunities for the graduate to observe owner-dentist case planning and communication
- Practice-funded access to software simulations for continued learning
These collaborations build confidence on both sides. The owner-dentist gains a partner in technology implementation, while the graduate receives real-world experience and professional guidance. As trust builds, mentorship can naturally evolve into long-term partnerships or ownership transition discussions.
The Business Case for Digital Integration
Investing in digital dentistry is both a clinical and business decision. Initial costs include hardware, software, and training. However, the return on investment comes from reduced lab fees, increased treatment acceptance, and faster turnaround times.25 Owner-dentists should evaluate their patient volume, case types, and long-term goals to determine the right digital mix.
Digital adoption should be strategic; beginning with a closed system to build confidence, then expand into open platforms as competence grows. Manufacturers are identifying buyers’ needs for open systems with reduced complexity and improved efficiency. The introduction to digital dentistry starts with an IOS but the right system should align first with the practice’s philosophy and support its growth trajectory.
The Future Is Now
Digital dentistry is becoming the standard of care. From scan to seat, CAD/CAM systems enhance diagnostic precision, restorative quality, and operational efficiency. Owner-dentists who delay digital adoption risk falling behind in a marketplace that increasingly favors speed, esthetics, and data-driven workflows.
Fortunately, they do not have to navigate this transformation alone. A new generation of graduates is ready to lead the way. With fluency in IOS, CAD/CAM, and digital delivery, these clinicians are prepared to modernize private practices. By strategically hiring and mentoring these individuals, practice owners can future-proof their businesses, improve clinical outcomes, and ensure long-term success.
The digital question has evolved. It’s no longer, “Should we go digital?” It’s, “How can we build a future-ready practice and thrive because of it?” The answer lies in partnerships. Embracing the digital fluency of today’s graduates, owner-dentists can not only modernize their workflows but future-proof their practices against digital inflation. Successful practice in the coming decades will work to cultivate technology, weave it into their practice culture, and mentor new associates and partners to shape the future generations of dentistry.
References
- What is the Digital Imperative? Sharp. Available at sharp.co.uk/news-and-events/blog/what-is-the-digital-imperative. Accessed July 16, 2025.
- Mangano F, Gandolfi A, Luongo G, Logozzo S. Intraoral scanners in dentistry: a review of the current literature. BMC Oral Health. 2017;17:149.
- Moörmann WH. The evolution of the CEREC system. J Am Dent Assoc. 2006;137:7S-13S.
- Miyazaki T, Hotta Y, Kunii J, Kuriyama S, Tamaki Y. A review of dental CAD/CAM: current status and future perspectives from 20 years of experience. Dent Mater J. 2009;28:44-56.
- Borbola D, Mikolicz A, Romanszky L, et al. Complete-arch accuracy of seven intraoral scanners measured by the virtual-fit method. J Dent. 2024;149:105281.
- Papaspyridakos P, Vazouras K, Chen Y, et al. Digital vs conventional implant impressions: a systematic review and meta‐analysis. J Prosthodont. 2020;29:660-678. d
- Prager MC, Liss H. Assessment of digital workflow in predoctoral education and patient care in north american dental schools. J Dent Educ. 2020;84:350-357.
- Kutkut A, Okeson J. Digital implant dentistry predoctoral program at University of Kentucky. J Oral Implantol. 2022;48:533-540.
- Newman M. The optimal digital workflow: Evaluating open and closed dental CAD/CAM systems. Available at dentistryiq.com/dentistry/products/cad-cam-and-3-d-printing/article/14302729/the-optimal-digital-workflow-evaluating-open-and-closed-dental-cad-cam-systems. Accessed July 16, 2025.
- Kaye G. Digital adoption: Training a staff in digital dental technology. Available at dentaleconomics.com/science-tech/article/16385080/ask-dr-kaye-about-digital-dentistrydigital-adoption-training-a-staff-in-digital-dental-technology. Accessed July 16, 2025.
- Fasbinder D, Sterlitz S. Practical considerations for digital dentistry. Decisions in Dentistry. 2017;3(9):14-21.
- Lively T. The realities of open architecture CAD/CAM. Available at dentalproductsreport.com/view/the-realities-of-open-architecture-cad-cam. Accessed July 16, 2025.
- Revilla‐León M, Özcan M. Additive Manufacturing technologies used for processing polymers: current status and potential application in prosthetic dentistry. J Prosthodon. 2019;28:146-158.
- Schwindling FS, Deisenhofer UK, Porsche M, Rammelsberg P, Kappel S, Stober T. Establishing CAD/CAM in preclinical dental education: evaluation of a hands-on module. J Dent Educ. 2015;79:1215-1221.
- Duplantis C. In-office milling vs. lab fabrication: making case decisions. Available at glidewelldental.com/education/chairside-magazine/volume-12-issue-2/milling-vs-fabrication. Accessed July 16, 2025.
- Bessadet M, Auduc C, Drancourt N, Nicolas E, El Osta N. Comparative analyses of time efficiency and cost in fabricating fixed implant-supported prostheses in digital, hybrid, and conventional workflows: A systematic review and meta-analysis. J Prosthet Dent. 2025;133:689-712.
- Park JS, Lim YJ, Kim B, Kim MJ, Kwon HB. Clinical Evaluation of Time Efficiency and Fit Accuracy of Lithium Disilicate Single Crowns between Conventional and Digital Impression. Materials. 2020;13(23):5467.
- Zhang Y, Vardhaman S, Rodrigues CS, Lawn BR. A critical review of dental lithia-based glass–ceramics. J Dent Res. 2023;102:245-253.
- Alqutaibi AY, Ghulam O, Krsoum M, et al. Revolution of current dental zirconia: a comprehensive review. Molecules. 2022;27:1699.
- Mandurino M, Cortili S, Coccoluto L, et al. Mechanical properties of 3d printed vs. subtractively manufactured composite resins for permanent restorations: a systematic review. Materials. 2025;18:985.
- Revilla‐León M, Kois DE, Zeitler JM, Att W, Kois JC. An overview of the digital occlusion technologies: Intraoral scanners, jaw tracking systems, and computerized occlusal analysis devices. J Esthet Restor Dent. 2023;35:735-744.
- Lee KC, Park JH, Kim J, Lee S, Moon D, Lee G. Digital application of three‐dimensional diagnosis and treatment with a virtual articulator. J Esthet Restor Dent. 2024;36:710-722.
- Jones R. Reasons technology training fails. Available at trainingfolks.com/blog/why-technology-training-fails. Accessed July 16, 2025.
- Jurado CA, Tsujimoto A, Punj A, Aida N, Miyazaki M, Watanabe H. Successful development and implementation of a digital dentistry curriculum at a US dental school. J Oral Sci. 2021;63:358-360.
- Bah I, Mathews L. Dental technology purchases: Strategies and considerations. Available at dentaleconomics.com/science-tech/article/55236884/dental-technology-purchases-strategies-and-considerations. Accessed July 16, 2025.
From Decisions in Dentistry. July/August 2025;11(4):20-23.
