
 GOODLIFESTUDIO / E+/ GETTY IMAGES PLUS
GOODLIFESTUDIO / E+/ GETTY IMAGES PLUS
Diagnosing and Treating Nasopalatine Duct Cysts
Oral health professionals who understand the common characteristics of nasopalatine duct cysts can effectively diagnose and manage these lesions.
PURCHASE COURSE
This course was published in the February 2023 issue and expires February 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the February 2023 issue and expires February 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 730
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify the prevalence and etiology of nasopalatine duct cysts.
- Describe the clinical and radiographic presentations of nasopalatine duct cysts.
- Discuss treatment considerations when caring for patients who present with a nasopalatine duct cyst.
The nasopalatine duct cyst (NPDC), also known as the incisive canal cyst, is the most common nonodontogenic cyst of the oral cavity.1 First described by Meyer2 in 1914, these developmental cysts typically occur in the midline of the anterior maxilla near the incisive foramen. While the presentation may appear to be characteristic, other benign conditions can mimic NPDCs; thus, an overview of the NPDC will allow oral health professionals to become familiar with the characteristics and management of these lesions.
The NPDC comprises 12% of jaw cysts, with a slightly higher frequency in men. Most present in the fourth through sixth decades, with the average age at diagnosis reported as 46.2 years.3 No racial predilection has been identified.3
The etiology of NPDCs is unknown. Most cases appear to be idiopathic.4,5 Possible causes may include trauma, infections, ill-fitting dentures, and retention phenomenon of blocked mucous glands.6 Spontaneous cystic degeneration of epithelial remnants has been suggested as a likely etiology.4,7 More recently, cystic development after placement of a dental implant has been reported.8
PATHOPHYSIOLOGY
The origin of NPDCs is believed to arise from embryonic epithelial remnants of the nasopalatine duct.9 This duct plays an important role in fetal development, as it is the connection between the nasal cavity and premaxilla. As the fetus continues to develop, this connection narrows as the anterior bones of the palate fuse. This results in the formation of the incisive canal that houses nerves and blood vessels.9 The nasopalatine canals usually fuse together prior to exiting the incisive foramen.10 These canals can exit the incisive foramen in three different patterns: type 1, which is a single canal; type 2, where the canals remain separated (parallel canals); or type 3, where the canals fuse prior to exiting, forming a “Y” type of canal.10
Cell types within the nasopalatine canals are variable and change as the canal moves downward to exit the incisive foramen.4,9,11 Histologically, the upward portions of the canals near the nasal area contain respiratory epithelial cells. As the canal moves downward, cuboidal cells are found in the lining. Squamous cells are found near the oral cavity. In addition, mucous secreting glands are also found in the canals. The branches of the descending palatine and sphenopalatine arteries are also housed within these canals.4,9,11 The nasopalatine cells undergo degeneration; however, remaining epithelial cells and mucous secreting cells can create a foundation for NPDCs.11
CLINICAL PRESENTATION
Clinically, an NPDC can vary in size and presentation. In the early stages, NPDCs are frequently small and asymptomatic. Case reports have demonstrated these lesions are more likely to be identified on routine radiographic examination.7,9,12–14
The most commonly reported clinical symptom of larger cysts is swelling in the anterior part of the palate.15,16 Another symptom is pain in the anterior part of the maxilla that radiates into the bridge of the nose. The pain can present as an intermittent burning sensation and may be associated with infection. Tooth displacement, nasal obstruction, or discharge into the nasal cavity or oral cavity are other symptoms associated with NPDCs.1,12,17,18 The vitality of teeth is variable.18
DIFFERENTIAL DIAGNOSIS
Due to the radiographic similarities and location of this particular cyst, a differential diagnosis for NPDCs may include odontogenic cysts, such as periapical granuloma and radicular cysts, or median palatine cysts.19,20 Nonodontogenic tumors, osteitis, an enlarged nasopalatine duct, and nevoid basal carcinoma syndrome have also been considered as possible differential diagnoses.4
Odontogenic cysts can be inflammatory, such as periapical granulomas and radicular cysts, or developmental. The periapical granuloma is considered the first stage of inflammation as granulation tissue is created.19 Chemical mediators induced by chronic inflammation stimulate epithelial rests, which transform the granuloma into a radicular cyst. Both the granuloma and radicular cyst create a well-defined round or ovoid radiolucency around the apical portion of the tooth; they are confirmed through a histological examination. Differential diagnoses between a periapical granuloma, radicular cyst and an NPDC is determined by tooth vitality testing.19,21,22
The median palatine cyst — which is usually located in the same region as the NPDC, but will be more posteriorly placed and centered toward the midline of the palate — is an example of a developmental cyst.19 This lesion is lined by stratified squamous epithelium and is believed to develop from the entrapped epithelial cells in the embryonic fusion of the lateral maxillary process to form the hard palate. Pain is often reported with this cyst as it expands and compresses the nasopalatine nerve. There is also a male predilection similar to the NPDC.19
Nonodontogenic tumors, such as the central giant cell granuloma (CGCG), are more commonly found in the mandible (65% to 75%); however, these lesions can also be located in the maxilla.19,20 Clinically, CGCGs are most often found anterior to the molar region. Although painless, CGCG will appear as a radiolucent lesion with expanding margins. If the lesion extends through the maxillary or mandibular bone structure, it will appear intraorally as a soft, flat-based nodule with a purple-blue color. Teeth and roots may also be divergent with the CGCG’s enlarged growth.19
Osteitis can be considered a differential diagnosis, especially with a fistula tracking toward the palate.4 A bucconasal or buccosinusal communication might also be present, with manifestations similar to that of an NPDC. An enlarged nasopalatine duct less than 6 mm in diameter would serve as an additional differential diagnosis.4
Nevoid basal cell carcinoma syndrome is an inherited autosomal dominant disorder primarily affecting men, with a median age of 41 at diagnosis. This condition, which can manifest as jaw cysts,19 will often present with odontogenic keratocysts, which can be round and ovoid in appearance, with well-defined borders and appear lateral to a tooth radiographically. Although odontogenic keratocysts are predominantly located in the mandible (80%), they can also manifest in the maxilla.19
DIAGNOSIS
Imaging studies are used to identify NPDCs. Radiographic examination may include panoramic, occlusal and periapical imaging, and typically discloses a well-defined, ovoid, round, pear-shaped or heart-shaped radiolucency located in the midline of the maxilla between the central incisors.3,9,23 The diameter of the incisive canal is expected to be 6 mm or less; therefore, radiolucencies larger than this size should warrant further investigation for pathologic lesions, such as NPDCs.3,9

Other radiographic techniques used to diagnose NPDC include multimodal tomography, magnetic resonance imaging and computed tomography scanning. Three-dimensional images are highly reliable in differentiating NPDCs from other anatomical features or other cysts of odontogenic origin. In addition, these techniques facilitate planning the best surgical approach for removing the lesion.3,4,15
Tooth vitality testing and percussion testing may be performed to avoid unnecessary endodontic treatment when there is concern about the vitality of the maxillary central incisors.22,24 Aspiration of radiolucencies may be useful in distinguishing solid masses from cystic lesions, but is not diagnostic per se. For example, a clear or straw-colored aspirate is suggestive of an NPDC. However, this type of aspirate is also suggestive of a lateral radicular cyst or cystic ameloblastoma.3
Histopathologic examination of NPDCs reveals squamous cell epithelium surrounded by a connective tissue wall. Other types of epithelium may be present, including columnar, cuboidal, and ciliary cylindrical cells. Melanin remains and erythrocytes have been found in the cyst wall, as well as an inflammatory infiltrate of polymorphonuclear leukocytes and plasma cells. Immunohistochemistry profiles have also been used for diagnosis, including profiles for K7, K13, MUC-1 and P63.3,4,16,25
TREATMENT AND PROGNOSIS
Treatment of an NPDC is by surgical enucleation, while marsupialization has been applied for larger cysts.1,4 Bone regeneration within the bony defect is anticipated. That noted, options for treatment of large cystic defects when both cortical plates are perforated include fibrin powder, thrombin, patient’s blood and antibiotics, platelet-rich fibrin, xenograft bone with aspirate bone marrow, recombinant bone morphogenic protein-2 in conjunction with rib graft, fibrin and collagen sponges, hydroxyapatite, calcium sulphates, and synthetic materials.15 Paresthesia of the anterior palate has been reported as a complication in 10% of cases if portions of the long sphenopalatine nerve are removed or damaged during the surgical procedure.17,26,27 Following surgical removal, recurrence of an NPDC is rare. Malignant transformation has been reported in two cases, indicating this is an extremely unusual complication.28,29

CASE REPORT
A 50-year-old male presented to the clinic for a routine examination and a full-mouth series of radiographs. The health history revealed the presence of seasonal allergies and a positive COVID-19 test during the second week of January 2022. The dental history included a high caries risk and clinical gingival health on a reduced periodontium in a nonperiodontitis patient. The patient reported sensitivity along the face around the area of the maxillary left central incisor when he had COVID-19, so initially the symptoms were blamed on his illness. Once he recovered from his illness, the patient complained that the maxillary left central and left lateral incisors (teeth #9 and 10) felt mobile when blowing his nose. He also reported symptoms of pain, tenderness and swelling associated with tooth #9.
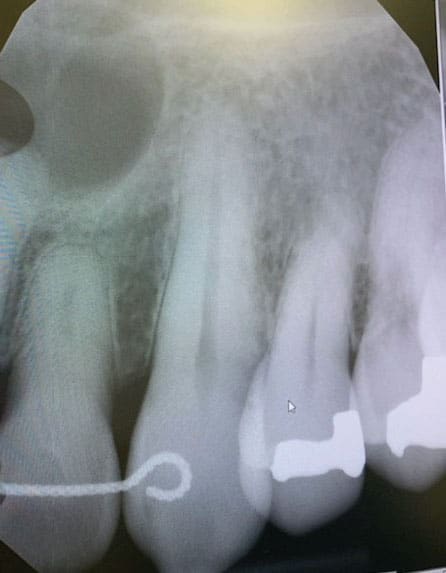
Upon completion of the full-mouth series, the anterior periapical radiograph revealed a large radiolucent lesion above tooth #9 (Figure 1). The patient was referred to a periodontist for further evaluation. Although the patient did have mobility associated with the tooth, subsequent tooth vitality testing was negative. He was then referred to an endodontist, who performed root canal therapy on tooth #9 and referred the patient back to the periodontist for removal of the cyst.
As an NPDC was suspected, a cone beam computed tomography scan of the cyst was recommended and performed (Figure 2). The cyst was surgically removed (Figure 3) and the biopsy report confirmed the finding of an NPDC. The patient was informed that the prognosis was good and recurrence was rare. He was advised to return for follow-up to monitor wound healing.
While this case resulted in a favorable outcome, there are examples in which a patient can be misdiagnosed and improper treatment can occur. Hilfer et al30 noted instances in which NPDC lesions have an inverted pear or heart shape superimposed on the nasal spine, which are misdiagnosed as a nonhealing periapical granuloma, resulting in unnecessary extraction of one or more teeth. It is important to use multiple diagnostic modalities to identify these lesions and ensure appropriate treatment is rendered.
CONCLUSION
As noted, the NPDC is one of the most common nonodontogenic cysts of the oral cavity, but this condition is sometimes misdiagnosed. Although the etiology of NPDCs is unknown, these lesions can vary in presentation. The NPDC is most often detected through radiographs and can be confirmed through multiple imaging studies. Patients will often report swelling of the anterior maxilla and intermittent pain that radiates across the bridge of the nose. Other symptoms might include nasal obstruction or discharge into the nasal cavity or oral cavity. Tooth displacement can also be present. In order to avoid unnecessary or inappropriate treatment, a differential diagnosis must be considered before developing a treatment plan. Surgical enucleation and marsupialization are considered effective treatment options for NPDCs.
References
- Neville BW, Damm DD, Allen CM, Chi AC. Oral and Maxillofacial Pathology. 4th ed. Philadelphia: Elsevier; 2016:26–28.
- Meyer AW. A unique supernumerary paranasal sinus directly above the superior incisors. J Anat.1914;48:118–129.
- Kurnatowski P. Nasopalatine duct cyst. Available at: https://emedicine.medscape.com/article/蜆-print. Accessed January 3, 2023.
- Francoli JE, Marques NA, Aytes LB, Escoda CG. Nasopalatine duct cyst: report of 22 cases and review of the literature. Med Oral Patol Oral Cir Bucal. 2008;13:E438–E443.
- Sankar D, Muthusubramanian V, Nathan JA, et al. Aggressive nasopalatine duct cyst with destruction of palatine bone. J Pharm Bioallied Sci. 2016;8(Suppl 1):S185–S188.
- Aparna M, Chakravarthy A, Acharya SR, Radhakrishnan R. A clinical report demonstrating the significance of distinguishing a nasopalatine duct cyst from a radicular cyst. BMJ Case Rep. 2014:bcr2013200329.
- Bodner L, Manor E, Glazer M, Brennan PA. Cystic lesions of the jaws in edentulous patients: analysis of 27 cases. Br J Oral Maxillofac Surg. 2010:49:643–646.
- Al-Shamiri HM, Elfaki S, Al-Maweri SA, et al. Development of nasopalatine duct cyst in relation to dental implant placement. N Am J Med Sci. 2016;8:13–16.
- Nelson BL, Linfesty RL. Nasopalatine duct cyst. Head Neck Pathol. 2010;4:121–122.
- Suter VG, Sendi P, Reichart PA, Bornstein MM. The nasopalatine duct cyst: An analysis of the relation between clinical symptoms, cyst dimensions, and involvement of neighboring anatomical structures using cone beam computed tomography. J Oral Maxillofac Surg. 2001;69:2595–2603.
- Allard, RH, van der Kwast WA, van der Waal I. Nasopalatine duct cyst. Review of the literature and report of 22 cases. Int J Oral Surg. 1981;10:447–461.
- Elliott KA, Franzese CB, Pitman KT. Diagnosis and surgical management of nasopalatine duct cysts. Laryngoscope. 2004;114:1336–1340.
- Righini CA, Bettega G, Boubagra K, Reyt E. Nasopalatine duct cyst (NPDc): one case report. Acta Otorhinolaryngol Belg. 2004;58:129–133.
- Tanaka S, Iida S, Murakami S, et al. Extensive nasopalatine duct cyst causing nasopalatine protrusion. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106:e46–e50.
- Perumal CJ. An unusually large destructive nasopalatine duct cyst: a case report. J Maxillofac Oral Surg. 2013;12:100–104.
- Tsuneki M, Maruyama S, Yamazaki M, et al. Inflammatory histopathogenesis of nasopalatine duct cyst: a clinicopathological study of 41 cases. Oral Dis. 2013;19:415–424.
- Szubert P, Sokalski J, Krauze A, et al. Nasopalatine duct cyst: case reports. Dent Med Probl. 2010;47:508–512.
- Velasquez-Smith MT, Mason C, Coonar H, Bennett J. A nasopalatine cyst in an 8-year-old child. Int J Paediatr Dent. 1999;9:123–127.
- Delong N, Burkhart NW. General and Oral Pathology for the Dental Hygienist. 3rd ed. Alphen aan den Rijn, Netherlands: Wolters Kluwer; 2019:438–482.
- Cecchetti F, Ottria L, Bartuli F, Bramanti NE, Acuri C. Prevalence, distribution, and differential diagnosis of nasopalatine duct cysts. Oral Implantol (Rome). 2012;5:47–53.
- Faitaroni LA, Bueno MR, Carvalhosa AA, Mendonca EF, Estrela C. Differential diagnosis of apical periodontitis and nasopalatine duct cyst. J Endod. 2011;37:403–410.
- Regezi JA, Scuibba JL, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 7th ed. Philadelphia: Elsevier; 2017:260–261.
- Moss HD, Hellstein JW, Johnson JD. Endodontic considerations of the nasopalatine duct region. J Endod. 2000;26:107–110.
- Gnanasekhar JD, Walvekar SV, Al-Kandari Am, et al. Misdiagnosis and mismanagement of a nasopalatine duct cyst and its corrective therapy. A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;80:465-470.
- Vasconcelos R, de Aguiar MF, Castro W, et al. Retrospective analysis of 31 cases of nasopalatine duct cyst. Oral Dis. 1999;5:325–328.
- Anneroth G, Hall G, Stuge U. Nasopalatine duct cyst. Int J Oral Maxillofac Surg. 1986;15:572–580.
- Bodin I, Isacsson G, Julin P. Cysts of the nasopalatine duct. Int J Oral Maxillofac Surg. 1986;15:696–706.
- Takagi R, Ohashi Y, Suzuki M. Squamous cell carcinoma in the maxilla probably originating from a nasopalatine duct cyst: report of case. J Oral Maxillofac Surg. 1996;54:112–115.
- Takeda Y. Intra-osseous squamous cell carcinoma of the maxilla: probably arisen from non-odontogenic epithelium. Br J Oral Maxillofac Surg. 1991;29:392–394.
- Hilfer PB, Bergeron BE, Ozgul ES, Wong DK. Misdiagnosis of a nasopalatine duct cyst: a case report. J Endod. 2013;39:1185–1188.
From Decisions in Dentistry. February 2023;9(2)36,39-41.

