

Conservative Management of Horizontal Root Fractures
This case report explores the long-term viability of a maxillary lateral incisor with a horizontal root fracture retained primarily by soft tissue, emphasizing conservative management strategies over extraction or endodontic treatment.
PURCHASE COURSE
This course was published in the May/June 2025 issue and expires June 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
This course was published in the May/June 2025 issue and expires June 2028. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 070
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the diagnostic protocol for identifying horizontal root fractures, including clinical, radiographic, and vitality assessments.
- Identify the indications, risks, and outcomes associated with conservative versus proactive treatment approaches to horizontal root fractures.
- Discuss the factors influencing healing and prognosis of HRFs at the cervical root level and the implications for adolescent and adult patient care.
About 15% of the world’s population have experienced a traumatic injury to their permanent dentition, amounting to approximately 1 billion people around the globe.1 The average age of traumatic dental injury is 13.8 years; men and boys are 34% to 52% more likely to experience dental trauma than women and girls.1 Root fractures contribute to 0.5% to 7% of all traumatic cases to the permanent dentition and are often the result of traumatic sports injuries, fights, and accidents.1-4
Single-rooted teeth, such as maxillary central incisors and maxillary lateral incisors, are the most often affected by horizontal root fractures (HRFs).5 Proper treatment of HRFs begins with an accurate diagnosis established through clinical examination, radiographic findings, and sensibility testing.4
Adolescent Patients
Managing traumatic dental injuries in adolescents can be challenging, even for the most experienced dental professional. Treatment for such an injury is often characterized by unpredictability in pulpal response, complexity, and significant financial implications, potentially lasting throughout the lifetime.6 Risks associated with untreated dental trauma can include pain, infection, loss of hard and soft tissues, and missed opportunities for ideal treatment.
The ongoing debate between proactive treatment and conservative management centers on whether to intervene early or preserve the natural tooth for as long as possible. This case study highlights a 34-year-old man with an HRF within the coronal root third of a vital maxillary right lateral incisor. The tooth is primarily soft tissue retained and has received two independent orthodontic treatment periods following a traumatic injury 22 years ago. Long-term prognosis, conservative management vs proactive treatment in the context of HRFs, and the risks and benefits associated with both approaches are discussed.
Case Report
In 2022, a 34-year-old man underwent a comprehensive evaluation in a dental school setting (Figure 1). Routine radiographs revealed a transverse fracture in the coronal root third of his right maxillary lateral incisor at the approximate level of the cementoenamel junction (CEJ) (Figure 2).

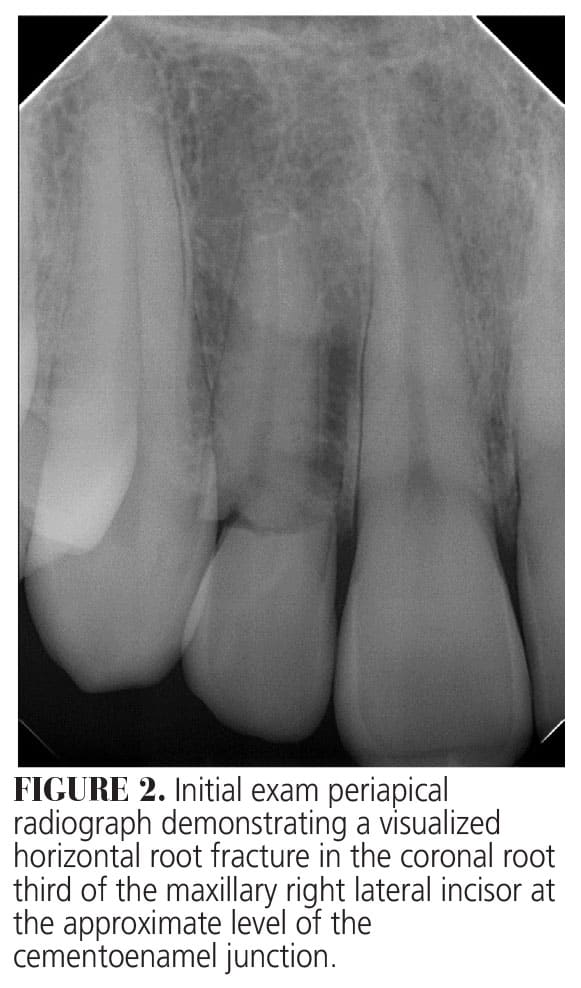
There was no radiographic evidence of periodontal ligament (PDL) space widening or vertical alveolar osseous defects. The radiograph demonstrated approximately 1 mm of mesial displacement of the coronal segment with an unmineralized pulpal canal and 1 mm radiolucent discontinuity between the coronal and radicular segments.
Following the radiographic finding, pertinent patient history was taken in which he reported sustaining trauma to the right labial alveolus caused by a weighted fishing lure while fishing in 2002. He experienced transient sharp pain lasting no more than 12 hours. Due to the absence of bleeding, visual displacement, or significant symptoms, the patient did not seek immediate treatment.
The patient maintained annual dental visits for prophylaxis and maintenance, had undergone orthodontic treatment as an adolescent, and a second and final round of orthodontic treatment as an adult from 2020 to 2021. The HRF remained undiagnosed.
The patient completed his final round of orthodontic aligner therapy prior to the discovery of the HRF in 2022. The tooth clinically displayed grade I mobility, a normal response to cold and electronic pulp testing (EPT), with slight discomfort to percussion. All other maxillary and mandibular anterior dentition tested vital with apical tissues within normal limits.
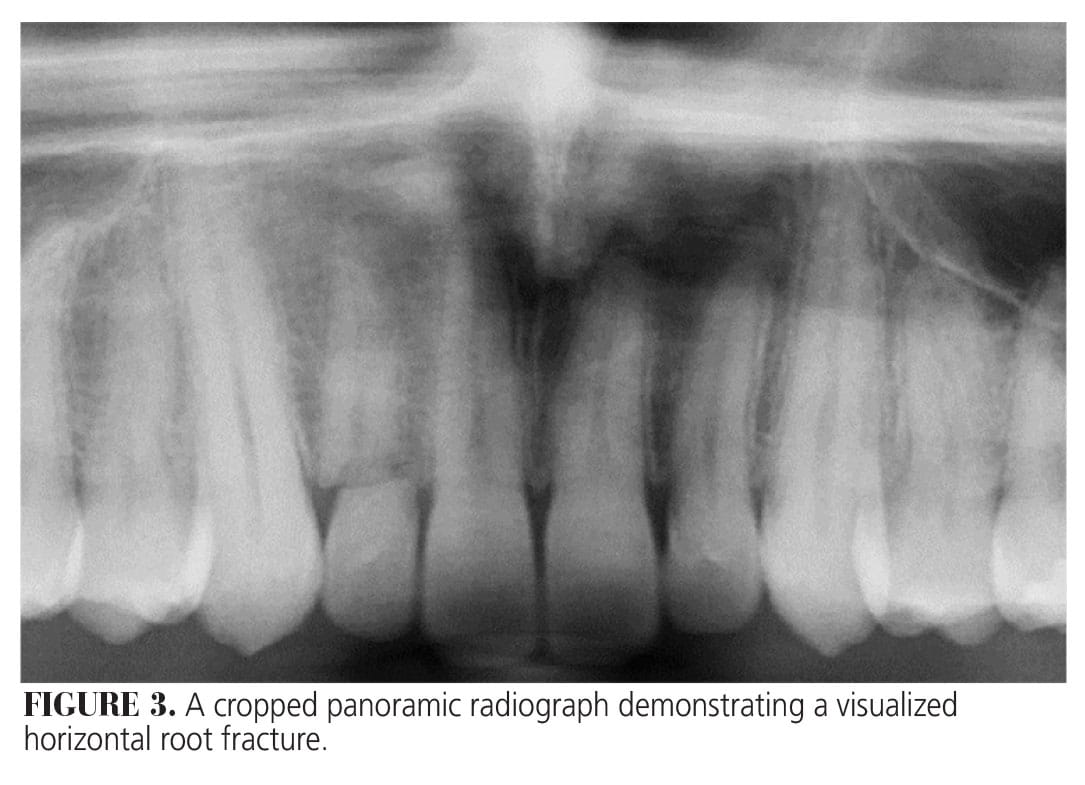
A panoramic radiograph and a 0.075 mm resolution limited field of view cone-beam computed tomography (CBCT) scan were acquired (Figure 3). The CBCT showed a low-density line coursing the full root dimension in all directions at the approximate CEJ level with #7 crown displaced mesially (Figure 4). The pulpal canal has an apparent “S” shaped delineation across the root fracture (Figure 4) and is unmineralized in both the coronal and root segments (Figure 5).
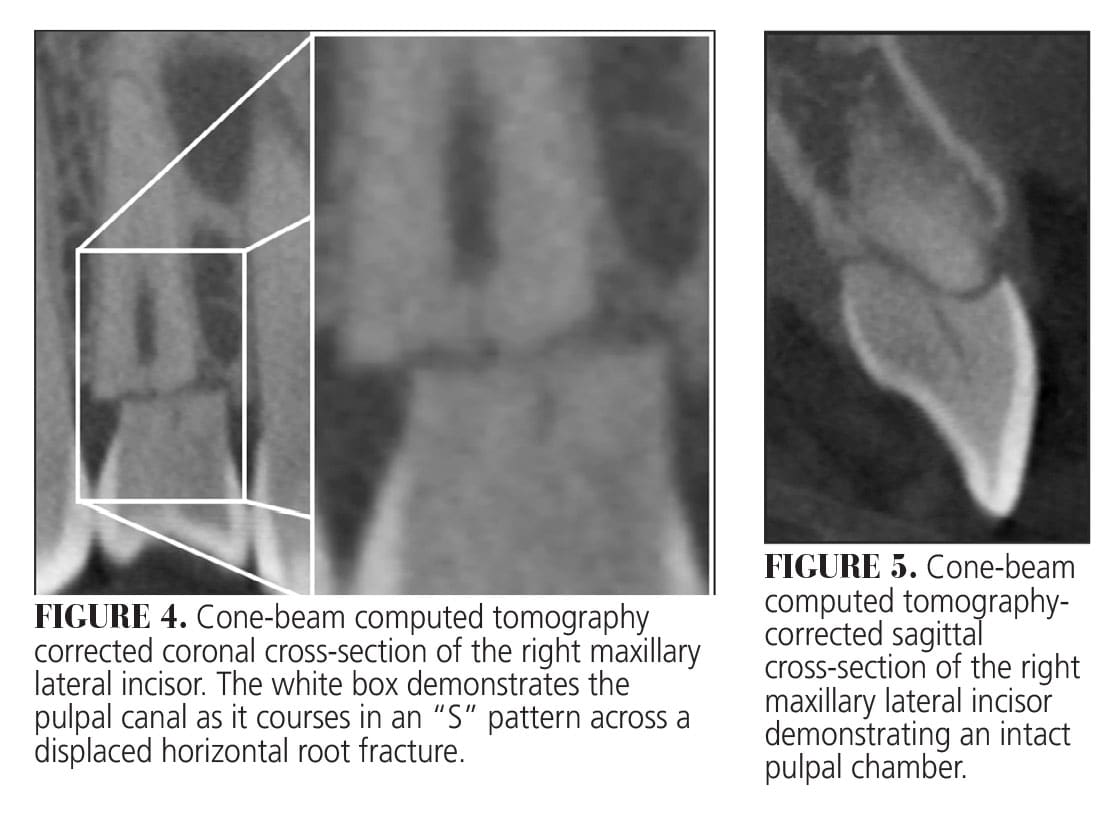
The coronal segment appears to be retained primarily by soft tissue, with only 0.6 mm of the lingual collar retained within the alveolus. Since the diagnosis, the patient has experienced increased mobility and pain on percussion, particularly when food directly contacts tooth #7. The patient adapts by chewing on the opposite side and cutting up certain foods, such as apples.
Treatment options, including conservative monitoring with avoidance of excessive occlusal loads, were discussed. Endodontic and orthodontic consultations suggested various interventions, ranging from orthodontic extrusion with root canal therapy (RCT), fixed orthodontic retention, core and crown, and implant options. This sparked a discussion on whether it was suitable to leave the tooth alone or take proactive intervention measures.
The patient opted for regular monitoring, acknowledging the guarded prognosis and risks of infection and damage to periodontal structures. Due to the development of recent sensitivity and pain, alternative treatment, such as flexible splinting, was discussed in the likely case of future complications. The challenge of restoring a single anterior tooth was also noted given the patient’s high esthetic demands.
Discussion
This case report demonstrates a 34-year-old patient with a complete, displaced HRF in the coronal root third that is primarily soft tissue retained of a vital maxillary lateral incisor which has remained relatively asymptomatic for 20 years. Not only did the patient live comfortably with a severely fractured tooth, but he also went through multiple rounds of orthodontics, which may have contributed to the displacement of the coronal segment but also caused no apparent long-term harm in pulp vitality.
Conservative Approach
The conservative management of HRFs is well established and includes repositioning the coronal segment, applying flexible splinting as needed, and observing the pulpal response with routine radiographic monitoring.5 The likelihood of pulpal necrosis following an HRF at any position within the root is 22% where the coronal segment becomes necrotic, and less than 1% of the apical segment becoming necrotic. The poorest prognosis was found in teeth showing HRF in the cervical part of the root; about 70% of these teeth required extraction by month 30.7 Fagundes4 notes that these fractures are more prone to contamination by bacterial invasion due to their proximity to anatomic grooves.
The longevity of pulpal stability of this patient’s case, soft tissue retainment, and multiple orthodontic treatments make it unique. Intra-alveolar stabilization is limited in the coronal root portion and healing by hard tissue occurs less frequently in the coronal third compared to other areas of the root, likely due to persistent mobility and occlusal forces.8,9 Despite the mobility of the transverse coronal segment and lack of support, the shorter length of this segment favors revascularization, which has shown to provide a better long-term prognosis.4,8
According to Lo Giudice et al,5 successful management of HRFs relies on three factors:
- Repositioning of displaced fragments
- Immobilization
- Presence of pulpal pathology
RCT is not dependent on fracture diagnosis alone but is indicated in cases of pulp necrosis.10-12 The pulpal response, in the absence of bacterial leakage and infection, depends on pulpal integrity.13 International Association for Dental Traumatology guidelines recommend that the pulpal response to cold and EPT should be evaluated at the time of trauma and up to 1 year after and annually for 5 years.14
Endodontic treatment should be planned only if pulp testing or EPT is negative after several months or there is another sign of pathosis such as radiographic PDL space widening, pain, swelling, sinus tract, and/or resorption detected.10 According to the American Academy of Endodontics,15 HRFs at the cervical level should be repositioned, stabilized with flexible splinting for up to 4 months, and monitored clinically and radiographically for at least 1 year, though healing is unlikely.
Responses to HRFs may include healing with hard dental tissue, healing with connective tissue, healing with connective tissue and bone, or no healing with granulation tissue developing within the fracture line.16 Andreasen et al17 found that the most important factors in healing vs pulpal necrosis are mobility or dislocation of the coronal segment and subsequent diastasis. If the pulpal tissue remains intact, healing may occur with the formation of a hard tissue barrier, fibrous tissue, or granulation tissue between the two fragments.9,18,19
Proactive Treatment
Traditionally, the proactive treatment option for a HRF at the coronal level would likely involve coronal segment extraction with RCT or tooth extraction.16 However, as evidenced by this case report, a more conservative management approach should be considered. This case demonstrates an opportunity for conservative treatment such as monitoring and periodic radiographic examination, particularly in cases of maintained vitality.
Regarding extraction of supracrestal HRFs, a risk/benefit analysis should be conducted including but not limited to vitality, pain, infection, potential bone and attachment loss and age of onset as viable conservative treatment options exist without extraction. This can be critical especially in an adolescent population experiencing trauma as premature dentition loss can have complex, severe, and long-term impacts.
Conclusion
This case report highlights the importance of assessing HRFs at the cervical level including regular monitoring, appropriate diagnostic imaging, vitality testing, and individualized patient care as conservative management can yield favorable long-term results. Further research and discussion are necessary to refine treatment protocols and enhance patient care.
References
- Petti S, Glendor U, Andersson L. World traumatic dental injury prevalence and incidence, a meta-analysis — one billion living people have had traumatic dental injuries. Dent Traumatol. 2018;34:71-86.
- Andreasen FM, Andreasen JO, Cvek M. Root fractures. In: Andreasen JO, Andreasen FM, Andersson L, eds. Textbook and Color Atlas of Traumatic Injuries to the Teeth. 4th ed. Kopenhagen: Blackwell Munksgaard; 2007:337-371.
- Oenning AC, de Azevedo Vaz SL, Melo SL, Haiter-Neto F. Usefulness of cone-beam CT in the evaluation of a spontaneously healed root fracture case. Dent Traumatol. 2013;29:489-493.
- Fagundes Ddos S, de Mendonça IL, de Albuquerque MT, Inojosa Ide F. Spontaneous healing responses detected by cone-beam computed tomography of horizontal root fractures: a report of two cases. Dent Traumatol. 2014;30:484-487.
- Lo Giudice R, Lizio A, Cervino G, et al. The horizontal root fractures: diagnosis, clinical management, and three-year follow-up. Open Dent J. 2018;12:540-552.
- Zaleckiene V, Peciuliene V, Brukiene V, Drukteinis S. Traumatic dental injuries: etiology, prevalence and possible outcomes. Stomatologija. 2014;16:7-14.
- Cvek M, Tsilingaridis G, Andreasen JO. Survival of 534 incisors after intra-alveolar root fracture in patients aged 7-17 years. Dent Traumatol. 2008;24:379-387.
- Cvek M, Mejare I, Andreasen JO. Healing and prognosis of teeth with intra-alveolar fractures involving the cervical part of the root. Dent Traumatol. 2002;18:57-65.
- Cvek M. Healing of 208 intraalveolar root fractures in patients aged 7–17 years. Dent Traumatol. 2001;17:53-59.
- Diangelis AJ, Andreasen JO, Ebeleseder KA, et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations of permanent teeth. Dent Traumatol. 2012;28:2-12.
- Tziafas D, Margelos I. Repair of untreated root fracture: A case report. Endod Dent Traumatol. 1993;9:40-43.
- Caliskan MK, Pehlivan Y. Prognosis of root-fractured permanent incisors. Endod Dent Traumatol. 1996;12:129-136.
- Lo Giudice G, Lizio A, Giudice RL, et al. The effect of different cleaning protocols on post space: A SEM study. Int J Dent. 2016;2016:1907124.
- Bourguignon C, Cohenca N, Lauridsen E, et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations. Dent Traumatol. 2020;36:314-330.
- American Association of Endodontics. The Recommended Guidelines of the American Academy of Endodontics for the Treatment of Traumatic Dental Injuries.Available at aae.org/specialty/wp-content/uploads/sites/2/2019/02/19_TraumaGuidelines.pdf. Accessed May 1, 2025.
- Abbott PV. Diagnosis and management of transverse root fractures. J Endod. 2019;45:S13-S27.
- Andreasen JO, Andreasen FM, Mejàre I, Cvek M. Healing of 400 intra-alveolar root fractures. 1. Effect of pre-injury and injury factors such as sex, age, stage of root development, fracture type, location of fracture and severity of dislocation. Dent Traumatol. 2004;20:192-202.
- Reis A, Loguercio AD, Kraul A, Matson E. Reattachment of fractured teeth: A review of literature regarding techniques and materials. Oper Dent. 2004;29:226-233.
- Cervino G, Fiorillo L, Spagnuolo G, et al. Interface between MTA and dental bonding agents: Scanning electron microscope evaluation. J Int Soc Prev Community Dent. 2017;7:64-68.
From Decisions in Dentistry. May/June 2025;11(3):36-39.

