

Caries Challenge in Native American Children
Although the prevalence and increased severity of caries in Native American children is well documented, the causes — and solutions — are less clear-cut.
Although the prevalence and increased severity of caries in Native American children is well documented, the causes — and solutions — are less clean-cut.
PURCHASE COURSE
This course was published in the November 2016 issue and expires 11/30/19. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
OBJECTIVES
After reading this course, the participant should be able to:
- Describe caries prevalence and severity in American Indian/Alaska Native (AI/AN) pediatric populations.
- List the key factors behind the caries epidemic in AI/AN children.
- Explain the geographic challenges that affect oral health interventions in this patient cohort.
- Discuss possible solutions for caries prevention and treatment in AI/AN children.
During a research project several years ago, I visited an American Indian reservation to train examiners to diagnose dental caries in young children. Prior to this visit, I had examined hundreds of children in schools, Head Start programs, and Women, Infants, and Children (WIC) programs for other studies, during which I had witnessed all levels and patterns of decay. Moreover, I was aware of the high prevalence and severity of this disease among American Indian communities. Thus, I felt prepared for what I was likely to see on the reservation. Instead, I found caries in the American Indian population to be an altogether different disease, with nearly every child having rampant and severe decay, often with multiple abscesses.
Unfortunately, my experience is typical of American Indian and Alaska Native (AI/AN) communities, where dental caries has long plagued the population. This paper documents the problem, likely causes and contributing factors, and possible solutions.
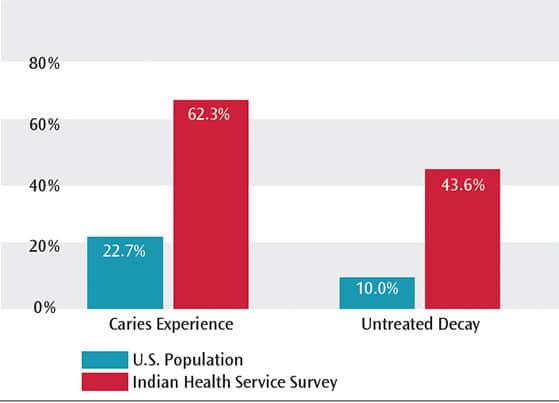
Dental caries affects a large percentage of AI/AN children before they begin school, and at levels of severity that surpass other population groups. As reported in the Indian Health Service’s (IHS) 2010 Survey of Preschool Children, 62.3% of AI/AN children ages 2 to 5 had decay experience, with a mean of 4.2 teeth affected per child.1 In comparison, a recent National Health and Nutrition Examination Survey (NHANES) reported that 22.7% of general-population children ages 2 to 5 had caries experience, with a mean of 1.2 teeth affected (Figure 1).2
Although data on American Indian children’s dental caries prevalence and severity prior to the 1960s are scarce, available evidence suggests that caries was uncommon in this population in the first half of the 20th century.3 By the 1960s, however, caries in American Indian children had become rampant.>sup>4,5 Indeed, despite general population declines in caries prevalence and severity over the past 50 years,6,7 this has not been the case for American Indian children.8–10
Studies in the 1990s reported high prevalence of caries and high levels of decayed, missing, or filled (dmf) teeth among children in the state of Washington,11 as well as children in the Navajo community,12 Alaska Head Start,13 Arizona Head Start and Arizona WIC programs.14 The first two studies11,12 suggested that inappropriate bottle feeding was strongly associated with caries. The latter studies13,14 documented that caries prevalence and severity (i.e., dmf) among AI/AN children were much higher than other groups of children attending the same programs. A more recent longitudinal study of American Indian children in a Northern Plains tribal community reported that 80% of children had caries experience by age 3. Additionally, the study found that caries was strongly associated with the following factors: consumption of sugarsweetened beverages, young mothers, mothers with increased caries rates, and a high number of individuals living in the same household.15
POVERTY
Dental caries is a disease closely related to poverty, with data from NHANES showing that children living at or below the U.S. federal poverty level have substantially higher rates of caries than those not living in poverty.7 Income also appears to be a contributing factor to caries in the AI/AN population, as many reservations — particularly those in the plains and West — are situated in some of the most impoverished counties in the U.S.16 There is considerable variation in the prevalence and severity of caries within the American Indian population,10 with higher prevalence reported among groups living in the poorest counties. Associations between poverty and high caries prevalence and severity are not fully understood, but it appears that poor diet, lack of self-care, and limited access to preventive and treatment services play key roles.
CARIOGENIC DIETS
A fundamental cause of dental caries is sugar consumption.17 Recent studies of early childhood caries have found that sugar consumption, often in the form of sugar-sweetened beverages (such as soda), is associated with both high caries prevalence18–21 and increased severity.21,22 As mentioned, a recent longitudinal study found sugar-sweetened beverages were associated with caries among 3-year-old American Indian children,15 suggesting that consuming sugar-sweetened beverages is a risk factor in this community.18–22
Addressing the dietary shortcomings of AI/AN groups is made especially difficult by the geographic isolation of many tribal communities. Reservations are typically served by small grocery stores that, to stay profitable, focus on products with relatively long shelf lives and high profit margins. As a result, processed foods and sugar-sweetened beverages are common, while healthy food choices, such as fresh fruits or vegetables, are limited.23 The availability of cheap, highsugar foods, combined with high poverty rates, can lead to cariogenic diets. Moreover, with limited food choices available — or affordable — efforts to improve dietary practices have little chance for success.
SELF-CARE PRACTICES
A growing body of literature suggests family and social factors — including parental stress — can impact parents’ oral self-care practices, and in turn, the oral health of their children.24–26 While there is limited evidence of this phenomenon in AI/AN communities, studies suggest that AI/AN parents have sufficient oral health knowledge, but may find it difficult to perform appropriate health behaviors.27,28 In light of social problems in AI/AN communities — including substance abuse and domestic violence, particularly affecting women — it is not surprising that AI/AN parents may struggle to implement optimal oral health behaviors on behalf of their children.27,29,30 Additionally, many AI/AN children are not consuming optimally fluoridated water8,31 or using fluoride toothpaste.28
LACK OF ACCESS TO DENTAL CARE
As discussed by Phipps et al,1 a severe dental access problem exists in AI/AN communities. Simply put, there are not enough dental providers to meet the needs of these communities. While many dental clinics, whether operated by IHS or tribal communities, are modern facilities, the remoteness of many AI/AN communities makes it difficult to recruit and retain dentists and other oral health professionals.1 As a result, 15% to 20% of dentist positions remain consistently vacant within IHS.1,10 The dental professionals who are employed by IHS or tribal communities are sometimes overwhelmed by emergency needs, leaving insufficient time to provide routine care or focus on prevention. Moreover, there is a shortage of pediatric dentists in tribal communities. As such, appropriate care may only be available offsite (e.g., hospital settings) for the numerous children who have extensive oral health care needs. In addition to these challenges, adequate housing is often difficult to find in or near tribal communities, and there may be limited employment opportunities for dentists’ family members.
ADDITIONAL FACTORS
Compared to other populations, studies suggest that tooth eruption in children from AI/AN communities tends to occur earlier for both primary32 and permanent33 dentitions. It has been hypothesized these early erupting teeth may be less well-developed and more prone to hypoplasia, a condition associated with a high caries rate.34 In addition, early eruption may contribute to the early onset of caries.
Finally, there is limited evidence to suggest that microbiota profiles in AI/AN children may differ from other populations. One study found that Northern Plains tribal children harbored an abundance of highly cariogenic Streptococcus sobrinus, in addition to typical caries-causative bacteria, such as Streptococcus mutans.35
In summary, while there is limited evidence regarding the specific causes of rampant caries in AI/AN populations, many factors common to these communities have been associated with caries in other populations. These include poverty, high-sugar diets, limited exposure to fluoride, lack of self-care, and poor access to professional dental services. In addition, AI/AN children may face other risk factors, including early tooth eruption and increased exposure to cariogenic microorganisms.
POTENTIAL SOLUTIONS
A common finding in studies of caries in AI/AN children is that severe disease often occurs at a very young age.1,8–12,15,36Thus, preventive and mitigative efforts must begin early and should likely include oral health education and behavioral modification by expectant mothers. Unfortunately, while numerous efforts have been attempted over the years, these have typically met with little success. Thus, any proposed solutions to this problem must be recognized as speculative.
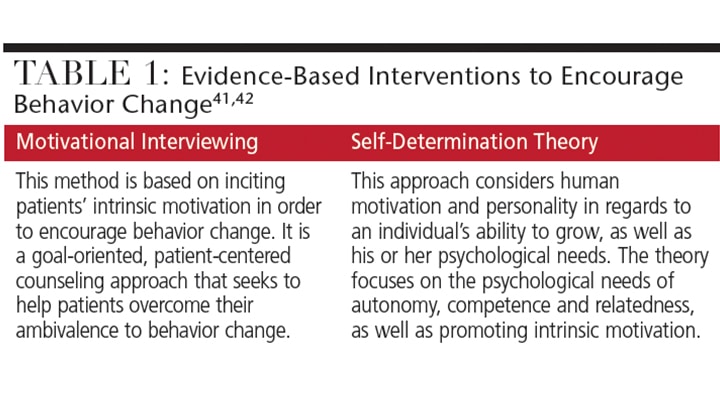
As suggested here, oral health education and behavioral modification aimed at new and expectant mothers appear to be key elements of any solution, especially in light of the early onset of caries in AI/AN children. Such efforts should be based on theoretical frameworks that use proven tools, including motivational interviewing and interventions based on the self-determination theory — both of which have been shown to improve parental oral health behaviors (Table 1).37–42
Another potential solution is to use a health management approach to provide early screening and referral for caries prevention and treatment. Under this approach, dental hygienists, nurses or other licensed clinicians perform oral health screenings to determine how urgently an individual needs professional dental care. If treatment is needed, dental care options are provided based on location, availability of appointments, and the type of care required. The care coordinator assists in arranging transportation to dental offices, finding child care, and communicating appointment reminders to patients to help ensure scheduled dental visits occur. The care coordinator might also provide direct preventive care, including fluoride varnish application, in a variety of dental and nondental settings.
 Finally, traditional dental preventive strategies — including the use of fluoride toothpaste, frequent application of fluoride varnish, and use of new anticaries products, such as silver diamine fluoride (SDF) — should be considered. It has been suggested that fluoride toothpaste is used less frequently than recommended in AI/AN populations,28 which may be related to the high rates of poverty in these communities. As such, one possible solution would be to provide fluoride toothpaste and instructions for use to parents/caregivers of young AI/AN children. Similarly, although biannual application of fluoride varnish has been shown to be effective in some populations,43 evidence is lacking as to whether monthly or quarterly applications would offer increased levels of prevention in disease-prone AI/AN communities.
Finally, traditional dental preventive strategies — including the use of fluoride toothpaste, frequent application of fluoride varnish, and use of new anticaries products, such as silver diamine fluoride (SDF) — should be considered. It has been suggested that fluoride toothpaste is used less frequently than recommended in AI/AN populations,28 which may be related to the high rates of poverty in these communities. As such, one possible solution would be to provide fluoride toothpaste and instructions for use to parents/caregivers of young AI/AN children. Similarly, although biannual application of fluoride varnish has been shown to be effective in some populations,43 evidence is lacking as to whether monthly or quarterly applications would offer increased levels of prevention in disease-prone AI/AN communities.
Recently, SDF has become available to U.S. clinicians, which may aid in the primary and secondary prevention of caries in young children.44 At least two clinical trials outside of the U.S. have demonstrated that, compared with placeboes or traditional fluoride applications, SDF provides significant preventive effects and better arrests existing lesions.45,46 Projects to test and demonstrate the effectiveness of silver products (such as SDF and silver nitrate) in AI/AN communities are underway, and preliminary results are promising.47 Although it is premature to suggest that meaningful progress has been made in addressing the problem of rampant caries in AI/AN children, the use of SDF and other approaches offers reason for hope.
REFERENCES
- Phipps KR, Ricks TL, Manz MC, Blahut P. Prevalence and severity of dental caries among American Indian and Alaska Native preschool children. J Public Health Dent. 2012;72:208–215.
- Dye BA, Thornton-Evans G, Li X, Iafolla TJ. Dental caries and sealant prevalence in children and adolescents in the United States, 2011–2012. NCHS Data Brief. 2015;191:1–8.
- Klein H, Palmer CE. Dental Caries in American Indian Children. United States. Government Printing Office, 1937. Public Health Bulletin No. 239.
- Ship II. Dental caries incidence in North and South Dakota Indian school children during 30 years. J Dent Res. 1966;45:359–363.
- Infante PF, Owen GM, Russell AL. Dental caries in preschool Apache Indian children. J Dent Res.1975:54:915.
- Hicks MJ, Flaitz CM. Epidemiology of dental caries in the pediatric and adolescent population: a review of past and current trends. J Clin Ped Dent.1993;18:43–49.
- Dye BA, Tan S, Smith V, et al. Trends in oral health status: United States, 1988–1994 and 1999–2004. Vital Health Stat. 2007;11:1–92.
- Niendorff W. The oral health of Native Americans: a summary of recent findings, trends and regional differences. Available at: repository.unm.edu/bitstream/handle/1928/27273/9702041-pt2-.pdf?sequence=2&isAllowed=y. Accessed September 30, 2016.
- Phipps KR, Ricks TL. The Oral Health of American Indian and Alaska Native Children Aged 1–5 Years: Results of the 2014 IHS Oral Health Survey. Rockville, Maryland: Indian Health Service; 2015.
- 2010 Indian Health Service Oral Health Survey of American Indian and Alaska Native Preschool Children. Rockville, Maryland: Indian Health Service; 2013.
- Tsubouchi J, Tsubouchi M, Maynard RJ, Domoto PK, Weinstein P. A study of dental caries and risk factors among Native American infants. J Dent Child.1995;62:283–287.
- O’Sullivan DM, Douglass JM, Champany R, Eberling S, Tetrev S, Tinanoff N. Dental caries prevalence and treatment among Navajo preschool children. J Public Health Dent.1994;54:139–144.
- Jones DB, Schlife CM, Phipps KR. An oral health survey of Head Start children in Alaska: Oral health status, treatment needs and cost of treatment. J Public Health Dent. 1992;52:86–93.
- Tang JMW, Altman SD, Robertson DC, O’Sullivan DM, Douglass JM, Tinanoff N. Dental caries prevalence and treatment levels in Arizona preschool children. Pub Health Rep. 1997:112:319–331.
- Warren JJ, Blanchette D, Dawson DV, et al. Factors associated with dental caries in a group of American Indian children at age 36 months. Community Dent Oral Epidemiol. 2016;44:154–161.
- United States Census Bureau Small Area Income and Poverty Estimates Program. 2014 Poverty and Median Household Income Estimates — Counties, States, and National. Available at: census.gov/did/www/saipe/data/interactive/saipe.html?s_appName=saipe&map_yearSelector=2014&map_geoSelector=aa_c. Accessed September 30, 2016.
- Shieham AS, James WPT. A reappraisal of the quantitative relationship between sugar intake and dental caries: the need for new criteria for developing goals for sugar intake. BMC Public Health. 2014;14:863.
- Declerck D, Leroy R, Martens L, et al.Factors associated with prevalence and severity of caries experience in preschool children. Community Dent Oral Epidemiol. 2007;36:168–178.
- Llena C, Forner L. Dietary habits in a child population in relation to caries experience. Caries Res. 2008;42:387–393.
- Seow WK, Clifford H. Battistutta D, Morawska A, Holcome T. Case-control study of early childhood caries in Australia. Caries Res. 2009;43:25–35.
- Warren JJ, Weber-Gasparoni K, Marshall TA, et al. A longitudinal study of dental caries risk among very young low SES children. Community Dent Oral Epidemiol. 2008;37:116–122.
- Kolker JL, Yuan Y, Burt BA, et al.Dental caries and dietary patterns in lowincome African American children. Pediatr Dent. 2007;29:457–463.
- Moss M. Salt Sugar Fat: How the Food Giants Hooked Us. New York:Random House; 2013.
- Finlayson TL, Siefert K, Ismail AI, Sohn W. Maternal self-efficacy and 1–5-year old children’s brushing habits. Community Dent Oral Epidemiol. 2007;35:272–281.
- Finlayson TL, Siefert K, Ismail AI,Sohn W. Psychosocial factors and early childhood caries among low-income African-American children in Detroit. Community Dent Oral Epidemiol. 2007;35:439–448.
- Bramlett MD, Soobader MJ, Fisher-Owens SA, et al. Assessing a multilevel model of young children’s oral health with national survey data. Community Dent Oral Epidemiol. 2010;38:287–298.
- Wilson A, Berga AG, Batliner TS, et al. Assessment of parental oral health knowledge and behaviors among American Indians of a Northern Plains tribe. J Public Health Dent.2014;74:159–167.
- Albino J, Tiwari T, Henderson WG, et al. Learning from caries-free children in a high-caries American Indian population. J Public Health Dent. 2014;74:293–300.
- Bohn DK. Lifetime physical and sexual abuse, substance abuse, depression and suicide attempts among Native American women. Issues Ment Health Nurs. 2003;24:333–352.
- Fairchild DG, Fairchild MW, Stoner S. Prevalence of adult domestic violence among women seeking routine care in a Native American health care facility. Am J Public Health. 1998;88:1515–1517.
- Albino JEN, Orlando VA. Promising directions for caries prevention with American Indian and Alaska Native children. Int Dent J. 2010;60:216–222.
- Warren JJ, Fontana M, Blanchette DR, et al. Timing of primary tooth emergence among U.S. racial and ethnic groups. J Public Health Dent. In press.
- Phipps KR, Ricks TL, Blahut P. Permanent first molar eruption and caries patterns in American Indian and Alaska Native children: challenging the concept of targeting second grade for school-based sealant programs. J Public Health Dent. 2013;73:175–178.
- Li Y, Navia JM, Bian JY. Caries experience in deciduous dentition of rural Chinese children 3–5 years old in relation to the presence of absence of enamel hypoplasia. Caries Res.1996;30:8–15.
- Lynch DJ, Villhauer AL, Warren JJ, et al. Genotypic characterization of initial acquisition of Streptococcus mutans in American Indian children. J Oral Microbiol. 2015;7:27182.
- Warren JJ, Kramer KW, Phipps K, et al. Dental caries in a cohort of very young American Indian children. J Public Health Dent. 2012;72:265–268.
- Weinstein P, Harrison R, Benton T.Motivating mothers to prevent caries: confirming the beneficial effect of counseling. J Am Dent Assoc. 2006;137:789–793.
- Albino J, Tiwari T. Preventing childhood caries: A review of recent behavioral research. J Dent Res.2016;95:35–42.
- Weber-Gasparoni K, Reeve J, Ghosheh N, et al. An effective psychoeducational intervention for ECC prevention: Part I. Pediatr Dent.2013:35:241–246.
- Weber-Gasparoni K, Warren JJ, Reeve J, Drake DR, Kramer KWO, Dawson DV. An effective psychoeducational intervention for ECC prevention: Part II. Pediatr Dent. 2013;35:247–251.
- Shannon S, Smith VJ, Gregory JW. A pilot study of motivational interviewing in adolescents with diabetes. Arch Dis Child. 2003;88:680–683.
- Deci E, Ryan R, eds. Handbook of Self-Determination Research. Rochester, New York: University of Rochester Press; 2002.
- Weintraub JA, Ramos-Gomez F, Jue B, et al. Fluoride varnish efficacy in preventing early childhood caries. J Dent Res. 2006;85:172–176.
- Alcorn M, Johnson T. New addition to the caries armamentarium. Dimensions of Dental Hygiene.2015;13(7):24–27.
- Chu CH, Lo EC, Lin HC. Effectiveness of silver diamine fluoride and sodium fluoride varnish in arresting dentin caries in Chinese preschool children. J Dent Res. 2002;81:767–777.
- Llodra JC, Rodriguez A, Ferrer B, Menardia V, Ramos T, Morato M. Efficacy of silver diamine fluoride for caries reduction in primary teeth and first permanent molars of schoolchildren:36-month clinical trial. J Dent Res.2005;84:721–724.
- American Dental Association. Symposium on Early Childhood Caries in American Indian and Alaska Native Children. Available at: ada.org/en/education-careers/events/symposium-onearly-childhood-caries-in-americanindian-and-alaska-native-children.Accessed September 30, 2016.
Featured Photo Courtesy of ND1939/ISTOCK/ THINKSTOCK
From Decisions in Dentistry. November 2016; 2(11):42-45.

